Intestinal Amyloidosis with Intractable Diarrhea and Intestinal Pseudo-obstruction
- Affiliations
-
- 1Department of Internal Medicine, Chonnam National University Medical School, Gwangju, Korea. dshskim@jnu.ac.kr
- 2Department of Pathology, Chonnam National University Medical School, Gwangju, Korea.
- KMID: 1389726
- DOI: http://doi.org/10.4166/kjg.2012.60.3.172
Abstract
- We report herein a case of intestinal amyloidosis with grave prognosis that caused intractable diarrhea and intestinal pseudo-obstruction, alternately in spite of intensive conservative treatment. A 44-year-old woman was admitted for fever, diarrhea, and crampy abdominal pain which had been continuned during 6 months. Abdomen CT scan showed edematous wall thickening of the small bowel and right colon, and colonoscopic biopsy revealed amyloid deposition in the mucosa. Monoclonal light chains in serum and/or urine were not detected and highly elevated serum amyloid A was shown. In spite of intensive treatment including oral prednisolone and colchicine, diarrhea and intestinal pseudo-obstruction developed alternately, general status rapidly got worsened and died after two months.
Keyword
MeSH Terms
-
Administration, Oral
Adult
Amyloidosis/complications/*diagnosis/drug therapy
Anti-Inflammatory Agents/therapeutic use
Colchicine/therapeutic use
Colonoscopy
Diarrhea/*etiology
Female
Humans
Intestinal Mucosa/pathology
Intestinal Pseudo-Obstruction/*diagnosis/etiology
Prednisolone/therapeutic use
Serum Amyloid A Protein/metabolism
Tomography, X-Ray Computed
Tubulin Modulators/therapeutic use
Figure
-

Fig. 1 Abdominal CT finding. Abdomen CT scan showed edematous wall thickening and mural enhancement of the pelvic small bowel loop and increased vascularity of the corresponding mesentery, mild edematous wall thickening of the colonic loop.

Fig. 2 Colonoscopic findings. Colonoscopy showed diffusely distributed petechial mucosal suggillations in the ascending colon (A) and shallow erosions in the terminal ileum (B).

Fig. 3 Microscopic findings. (A) Eosinophilic proteineous material deposition was identified in the lamina propria of the colonic mucosa (H&E, ×100). (B) This material resulted in a positive reaction using the Congo red stain (×200).
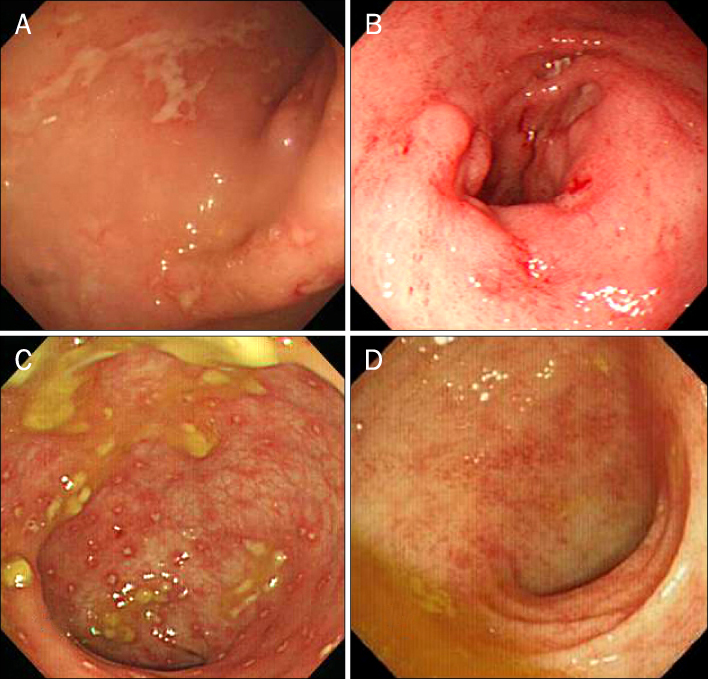
Fig. 4 Endoscopic findings. Endoscopic examinations revealed various findings such as diffuse geographic ulcerations (A), small healing ulcers or erosions (B), yellowish exudate coated hyperemic mucosal lesions (C) and mucosal and submucosal hemorrhagic spots (D).
Cited by 1 articles
-
A Case of Primary Gastric Amyloidosis with Fulminant Heart Failure
Seonghun Hong, Young-Woon Chang, Jong Kyu Byun, Min Je Kim, Jung Min Chae, Sun Hee Park, Chi Hyuk Oh, Yong-Koo Park
Korean J Gastroenterol. 2015;66(4):227-230. doi: 10.4166/kjg.2015.66.4.227.
Reference
-
1. Kala Z, Válek V, Kysela P. Amyloidosis of the small intestine. Eur J Radiol. 2007. 63:105–109.2. Fonnesu C, Giovinale M, Verrecchia E, et al. Gastrointestinal amyloidosis: a case of chronic diarrhoea. Eur Rev Med Pharmacol Sci. 2009. 13:Suppl 1. 45–50.3. Westermark P. Aspects on human amyloid forms and their fibril polypeptides. FEBS J. 2005. 272:5942–5949.4. Levine RA. Amyloid disease of the liver. Correlation of clinical, functional and morphologic features in forty-seven patients. Am J Med. 1962. 33:349–357.5. Naiki H, Nagai Y. Molecular pathogenesis of protein misfolding diseases: pathological molecular environments versus quality control systems against misfolded proteins. J Biochem. 2009. 146:751–756.6. Ebert EC, Nagar M. Gastrointestinal manifestations of amyloidosis. Am J Gastroenterol. 2008. 103:776–787.7. Röcken C, Shakespeare A. Pathology, diagnosis and pathogenesis of AA amyloidosis. Virchows Arch. 2002. 440:111–122.8. Okuda Y, Takasugi K, Oyama T, Oyama H, Nanba S, Miyamoto T. Intractable diarrhoea associated with secondary amyloidosis in rheumatoid arthritis. Ann Rheum Dis. 1997. 56:535–541.9. Fushimi T, Takahashi Y, Kashima Y, et al. Severe protein losing enteropathy with intractable diarrhea due to systemic AA amyloidosis, successfully treated with corticosteroid and octreotide. Amyloid. 2005. 12:48–53.10. Cathcart ES. Kelley WN, Harris ED, Ruddy S, Sledge CB, editors. Amyloidosis. Textbook of rheumatology. 1993. Philadelphia: W.B. Saunders Company;1413–1428.11. Feurle GE. Pathophysiology of diarrhea in patients with familial amyloid neuropathy. Digestion. 1987. 36:13–17.12. Hiramatsu K, Kaneko S, Shirota Y, et al. Gastrointestinal amyloidosis secondary to hypersensitivity vasculitis presenting with intestinal pseudoobstruction. Dig Dis Sci. 1998. 43:1824–1830.13. Braunstein JM, Aman A, Warman J. Colonic amyloidosis. Clin Gastroenterol Hepatol. 2007. 5:A30.14. Yamada M, Hatakeyama S, Tsukagoshi H. Gastrointestinal amyloid deposition in AL (primary or myeloma-associated) and AA (secondary) amyloidosis: diagnostic value of gastric biopsy. Hum Pathol. 1985. 16:1206–1211.15. Legge DA, Carlson HC, Wollaeger EE. Roentgenologic appearance of systemic amyloidosis involving gastrointestinal tract. Am J Roentgenol Radium Ther Nucl Med. 1970. 110:406–412.16. Kim SH, Han JK, Lee KH, et al. Abdominal amyloidosis: spectrum of radiological findings. Clin Radiol. 2003. 58:610–620.17. Schroeder FM, Miller FJ Jr, Nelson JA, Rankin RS. Gastrointestinal angiographic findings in systemic amyloidosis. AJR Am J Roentgenol. 1978. 131:143–146.18. Tada S, Iida M, Yao T, et al. Endoscopic features in amyloidosis of the small intestine: clinical and morphologic differences between chemical types of amyloid protein. Gastrointest Endosc. 1994. 40:45–50.19. Michael H, Brandt LJ, Tanaka KE, Berkowitz D, Cardillo M, Weidenheim K. Congo-red negative colonic amyloid with scalloping of the valvulae conniventes. Gastrointest Endosc. 2001. 53:653–655.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case of Megacystis Associated with Primary Chronic Intestinal Pseudoobstruction
- Chronic Idiopathic Intestinal Pseudo-obstruction in Adult: A Case Report with a Clinical Analysis of Other Reported Cases in Korean Literature
- Pseudo-Obstruction of Jejunum due to AA Amyloidosis Associated with Latent Syphilis
- A case of chronic intestinal pseudo-obstruction syndrome
- Acute Intestinal Pseudo-Obstruction in a Patient with MELAS Syndrome
