Intraductal Tubular Carcinoma of the Pancreas: a Case Report with the Imaging Findings
- Affiliations
-
- 1Department of Radiology and Center for Imaging Science, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea. kshyun@skku.edu
- 2Department of Surgery, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea.
- 3Department of Pathology, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea.
- KMID: 1385409
- DOI: http://doi.org/10.3348/kjr.2008.9.5.473
Abstract
- We describe here a case of intraductal tubular carcinoma of the main pancreatic duct. Gadolinium-enhanced pancreas magnetic resonance (MR) imaging showed an enhancing mass that was confined in the dilated main pancreatic duct of the pancreatic body, along with dilatation of the upstream main pancreatic duct and chronic pancreatitis that was due to obstruction. MR cholangiopancreatography and an endoscopic retrograde pancreatogram showed a filling defect that was due to an intraductal mass of the pancreatic body, along with dilatation of the upstream main pancreatic duct and no dilatation of the downstream main pancreatic duct. The pathological findings demonstrated an intraductal nodular appearance without papillary projection or mucin hypersecretion.
Keyword
MeSH Terms
-
Adenocarcinoma/*diagnosis/pathology
Carcinoma, Intraductal, Noninfiltrating/*diagnosis/pathology
Cholangiopancreatography, Endoscopic Retrograde
Cholangiopancreatography, Magnetic Resonance
Diagnosis, Differential
Female
Humans
Magnetic Resonance Imaging
Middle Aged
Neoplasm Staging
Pancreatic Neoplasms/*diagnosis/pathology
Tomography, X-Ray Computed
Figure
-
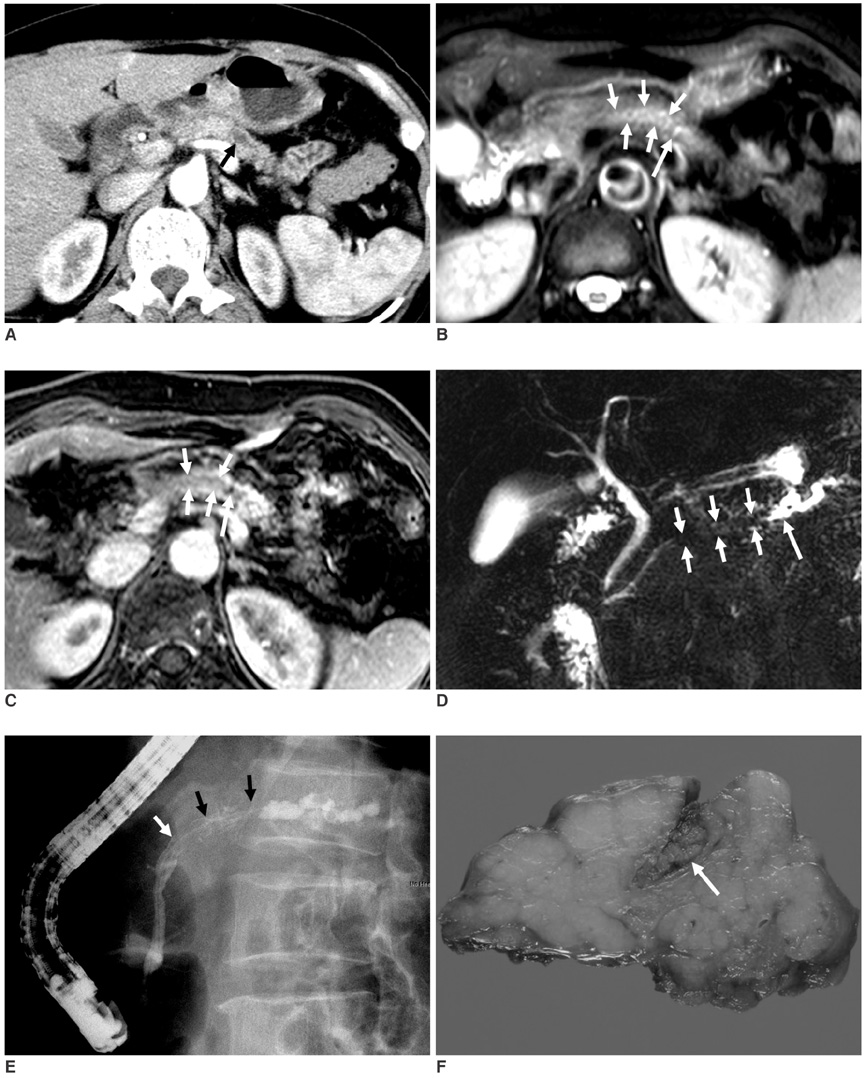
Fig. 1 63-year-old woman with intraductal tubular carcinoma of pancreas that presented as intraductal mass. A. Contrast-enhanced pancreas CT scan obtained at arterial phase shows only moderate dilatation of main pancreatic duct (arrow) in tail of pancreas, and there is no evidence of obstructive mass. Atrophy with decreased enhancement of pancreatic tail is due to chronic pancreatitis. B, C. T2-weighted (B) and gadolinium-enhanced (C) pancreas MR images show enhancing intraductal mass (short arrows) of main pancreatic duct in pancreatic body with dilatation of upstream main pancreatic duct (long arrow). D. MR cholangiopancretography shows filling defect (short arrows) that is due to intraductal mass with dilatation of upstream main pancreatic duct (long arrow) and there is no dilatation of downstream main pancreatic duct. E. Endoscopic retrograde pancreatogram shows filling defect (arrows) of contrast media that is due to mass in main pancreatic duct in pancreatic body. F. Photograph of resected specimen shows mass (arrow) in dilated main pancreatic duct.
Reference
-
1. Longnecker DS, Adler G, Hruban RH, Kloppel G. Hamilton SR, Aaltonen LA, editors. Intraductal papillary mucinous neoplasms of the pancreas. Pathology and genetics of tumours of the digestive system. WHO classification of tumours. 2000. Lyon: IARC Press;237–240.2. Japan Pancreas Society. General Rules for the Study of Pancreatic Cancer. 2002. 2nd ed. Tokyo: Kanehara.3. Tajiri T, Tate G, Inagaki T, Kunimura T, Inoue K, Mitsuya T, et al. Intraductal tubular neoplasms of the pancreas: histogenesis and differentiation. Pancreas. 2005. 30:115–121.4. Itatsu K, Sano T, Hiraoka N, Ojima H, Takahashi Y, Sakamoto Y, et al. Intraductal tubular carcinoma in an adenoma of the main pancreatic duct of the pancreas head. J Gastroenterol. 2006. 41:702–705.5. Tajiri T, Tate G, Kunimura T, Inoue K, Mitsuya T, Yoshiba M, et al. Histologic and immunohistochemical comparison of intraductal tubular carcinoma, intraductal papillary-mucinous carcinoma, and ductal adenocarcinoma of the pancreas. Pancreas. 2004. 29:116–122.6. Ito K, Fujita N, Noda Y, Kobayashi G, Kimura K, Horaguchi J, et al. Intraductal tubular adenocarcinoma of the pancreas diagnosed before surgery by transpapillary biopsy: case report and review. Gastrointest Endosc. 2005. 61:325–329.7. Thirot-Bidault A, Lazure T, Ples R, Dimet S, Dhalluin-Venier V, Fabre M, et al. Pancreatic intraductal tubular carcinoma: a subgroup of intraductal papillary-mucinous tumors or a distinct entity? A case report and review of the literature. Gastroenterol Clin Biol. 2006. 30:1301–1304.8. Hisa T, Nobukawa B, Suda K, Ohkubo H, Shiozawa S, Ishigame H, et al. Intraductal carcinoma with complex fusion of tubular glands without macroscopic mucus in main pancreatic duct: dilemma in classification. Pathol Int. 2007. 57:741–745.9. Suda K, Hirai S, Matsumoto Y, Mogaki M, Oyama T, Mitsui T, et al. Variant of intraductal carcinoma (with scant mucin production) is of main pancreatic duct origin: a clinicopathological study of four patients. Am J Gastroenterol. 1996. 91:798–800.10. Albores-Saavedra J, Sheahan K, O'Riain C, Shukla D. Intraductal tubular adenoma, pyloric type, of the pancreas: additional observations on a new type of pancreatic neoplasm. Am J Surg Pathol. 2004. 28:233–238.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Squamous cell carcinoma of the pancreas with a pancreatic intraductal papillary mucinous neoplasm: a case report
- Intraductal Papillary Mucinous Tumor Simultaneously Involving the Liver and Pancreas: A Case Report
- Squamous Cell Carcinoma of the Pancreas: A Case Report
- Radiologic Findings of Pancreatic Cystic Neoplasms
- Evaluation of malignant intraductal papillary mucinous neoplasms of the pancreas on computed tomography and magnetic resonance imaging
