Biliary Cast Formation with Sclerosing Cholangitis in Critically Ill Patient: Case Report and Literature Review
- Affiliations
-
- 1Department of Radiology, Daegu Fatima Hospital, Daegu 701-600, Korea.
- 2Department of Radiology, Kyungpook National University, School of Medicine, Daegu 700-422, Korea. shcho2405@gmail.com
- 3Department of Internal Medicine, Daegu Fatima Hospital, Daegu 701-600, Korea.
- 4Department of Radiology, Catholic University of Daegu, School of Medicine, Daegu 705-718, Korea.
- KMID: 1372858
- DOI: http://doi.org/10.3348/kjr.2012.13.3.358
Abstract
- Sclerosing cholangitis in critically ill patients (SC-CIP) is a rare condition that is not familiar to many radiologists. In addition, the associated imaging findings have not been described in the radiological literature. We report a case of biliary cast formation with SC-CIP and describe the radiological findings of CT, magnetic resonance cholangiopancreatography (MRCP), and endoscopic retrograde cholangiography (ERC). A diagnosis of SC-CIP should be considered in intensive care unit (ICU) patients with persistent cholestasis during or after a primary illness. The typical CT, MRCP and ERC findings include new biliary casts in the intrahepatic duct with multiple irregular strictures, dilatations, and relative sparing of the common bile duct.
Keyword
MeSH Terms
-
Aged
Cholangiopancreatography, Endoscopic Retrograde
Cholangiopancreatography, Magnetic Resonance
Cholangitis, Sclerosing/*diagnosis/drug therapy
Contrast Media/diagnostic use
*Critical Illness
Cryptogenic Organizing Pneumonia/diagnosis/surgery
Diagnosis, Differential
Humans
Liver Function Tests
Male
Thoracic Surgery, Video-Assisted
Tomography, X-Ray Computed
Figure
-
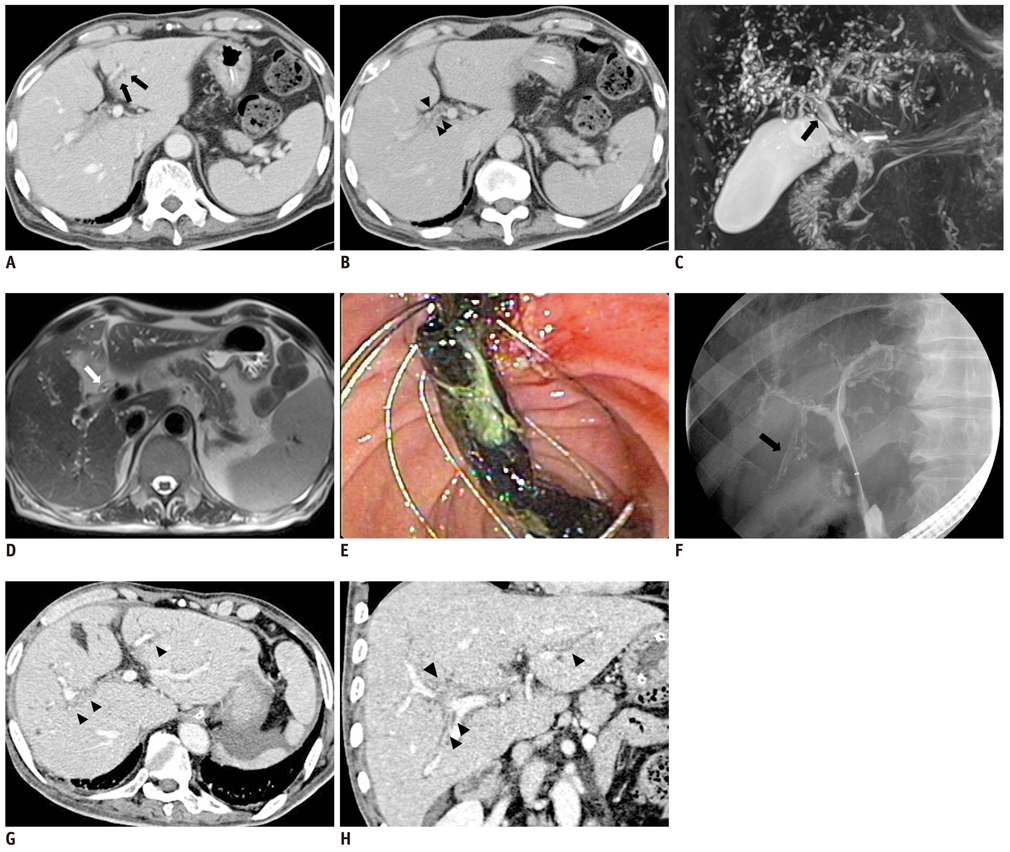
Fig. 1 68-year-old man with biliary cast formation with sclerosing cholangitis in critically ill patients. A. Contrast-enhanced axial computed tomography (CT) scan (5 mm slice thickness, portal phase) is suspicious of multifocal strictures and irregularities (arrows) in left intrahepatic duct (IHD). B. Contrast-enhanced axial CT scan (5 mm slice thickness, 3 min delayed phase) is suspicious of diffuse mild wall thickening (arrowheads) with increased intraluminal attenuation in right main IHD. C. 3D MIP magnetic resonance cholangiopencreatography image also reveals multiple strictures, irregularity, and beaded appearance in both IHDs. Elongated intraluminal filling defect, which indicates biliary cast (arrow) in proximal common bile duct (CBD) is seen. D. Heavily T2-weighted axial image shows intraductal filling defect, which is representative of biliary cast, in proximal CBD (arrow). E. Endoscopic removal of biliary cast after sphincterotomy. Endoscopic image shows black pigmented biliary cast that was retrieved through ampulla of Vater by basket. F. Seven weeks after initial cholestasis, ERC shows multifocal strictures, irregular dilatations in both IHD and biliary casts (arrow) in peripheral IHD. G, H. After 6 months, thin section contrast-enhanced axial CT scan (1.5 mm slice thickness, portal phase) and coronal scan (5 mm slice thickness) more clearly shows multiple irregular strictures and dilatations (arrowheads) in both IHD.
Reference
-
1. Gelbmann CM, Rümmele P, Wimmer M, Hofstädter F, Göhlmann B, Endlicher E, et al. Ischemic-like cholangiopathy with secondary sclerosing cholangitis in critically ill patients. Am J Gastroenterol. 2007. 102:1221–1229.2. Scheppach W, Druge G, Wittenberg G, Mueller JG, Gassel AM, Gassel HJ, et al. Sclerosing cholangitis and liver cirrhosis after extrabiliary infections: report on three cases. Crit Care Med. 2001. 29:438–441.3. Benninger J, Grobholz R, Oeztuerk Y, Antoni CH, Hahn EG, Singer MV, et al. Sclerosing cholangitis following severe trauma: description of a remarkable disease entity with emphasis on possible pathophysiologic mechanisms. World J Gastroenterol. 2005. 11:4199–4205.4. Jaeger C, Mayer G, Henrich R, Gossner L, Rabenstein T, May A, et al. Secondary sclerosing cholangitis after long-term treatment in an intensive care unit: clinical presentation, endoscopic findings, treatment, and follow-up. Endoscopy. 2006. 38:730–734.5. Parry SD, Muiesan P. Cholangiopathy and the biliary cast syndrome. Eur J Gastroenterol Hepatol. 2003. 15:341–343.6. Gleeson FC, Czaja AJ, Baron TH. Successful endoscopic management of biliary cast syndrome in nonliver transplant patients. J Clin Gastroenterol. 2008. 42:752–755.7. Ruemmele P, Hofstaedter F, Gelbmann CM. Secondary sclerosing cholangitis. Nat Rev Gastroenterol Hepatol. 2009. 6:287–295.8. Zimmer V, Raedle J, Treiber G, Lammert F. Biliary cast syndrome in sclerosing cholangitis. Dig Liver Dis. 2011. 43:e4.9. Katsinelos P, Kountouras J, Chatzimavroudis G, Zavos C, Pilpilidis I, Paroutoglou G. Combined endoscopic and ursodeoxycholic acid treatment of biliary cast syndrome in a non-transplant patient. World J Gastroenterol. 2008. 14:5223–5225.10. Esposito I, Kubisova A, Stiehl A, Kulaksiz H, Schirmacher P. Secondary sclerosing cholangitis after intensive care unit treatment: clues to the histopathological differential diagnosis. Virchows Arch. 2008. 453:339–345.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Biliary Tract & Pancreas; A Case of Cholangiocarcinoma Suggested as Developing in the Patient with Primary Sclerosing Cholangitis
- Primary Sclerosing Cholangitis: One Case Report
- A Case of Secondary Sclerosing Cholangitis in Langerhans Cell Histiocytosis
- Immunoglobulin G4-related sclerosing cholangitis
- Secondary Sclerosing Cholangitis in Critically Ill Patients
