A Case of B-cell Lymphoma, Unclassifiable, with Features Intermediate between Diffuse Large B-cell Lymphoma and Burkitt Lymphoma in a Korean Child
- Affiliations
-
- 1Department of Laboratory Medicine, Gachon University Gil Hospital, Incheon, Korea. jyahn@gilhospital.com
- KMID: 1245258
- DOI: http://doi.org/10.3343/alm.2012.32.2.162
Abstract
- B-cell lymphoma, unclassifiable, with features intermediate between diffuse large B-cell lymphoma (DLBCL) and Burkitt lymphoma (BL) (intermediate DLBCL/BL), is a heterogeneous group with some features resembling DLBCL and others resembling BL. Here, we report a case of intermediate DLBCL/BL in a Korean child. A 2-yr-old male was admitted for evaluation and management of left hip pain. Immunohistochemistry of a biopsy of the femur neck revealed tumor cells positive for CD20, CD10, BCL2, BCL6, and Ki67. A bone marrow (BM) aspirate smear revealed that 49.3% of all nucleated cells were abnormal lymphoid cells, composed of large- and medium-sized cells. Immunophenotyping of the neoplastic cells revealed positivity for CD19, CD10, CD20, and sIg lambda and negativity for CD34, Tdt, and myeloperoxidase (MPO). Cytogenetic and FISH analyses showed a complex karyotype, including t(8;14)(q24.1;q32) and IGH-MYC fusion. Intensive chemotherapy was initiated, including prednisone, vincristine, L-asparaginase, daunorubicin, and central nervous system prophylaxis with intrathecal methotrexate (MTX) and cytarabine. One month after the initial diagnosis, BM examination revealed the persistent of abnormal lymphoid cells; cerebrospinal fluid cytology, including cytospin, showed atypical lymphoid cells. The patient was treated again with cyclophosphamide, vincristine, prednisone, adriamycin, MTX, and intrathecal MTX and cytarabine. The patient died of sepsis 5 months after the second round of chemotherapy.
MeSH Terms
-
Antineoplastic Agents/therapeutic use
Bone Marrow Cells/pathology
Child, Preschool
Chromosomes, Human, Pair 14
Chromosomes, Human, Pair 8
Cyclophosphamide/therapeutic use
Doxorubicin/therapeutic use
Drug Therapy, Combination
Femur Neck/pathology
Humans
Immunohistochemistry
Immunophenotyping
In Situ Hybridization, Fluorescence
Karyotyping
Lymphoma, B-Cell/*diagnosis/drug therapy
Male
Methotrexate/therapeutic use
Oncogene Proteins, Fusion/genetics
Prednisolone/therapeutic use
Republic of Korea
Translocation, Genetic
Treatment Outcome
Vincristine/therapeutic use
Figure
-
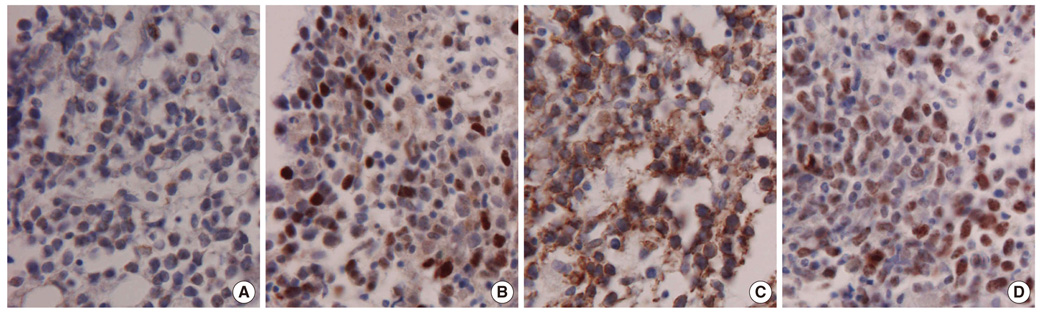
Fig. 1 Immunohistochemistry shows positivity for BCL2 (A), BCL6 (B), CD10 (C), and Ki67 (D) of tumor cells (Femur neck, immunohistochemical stains, 400× magnification).
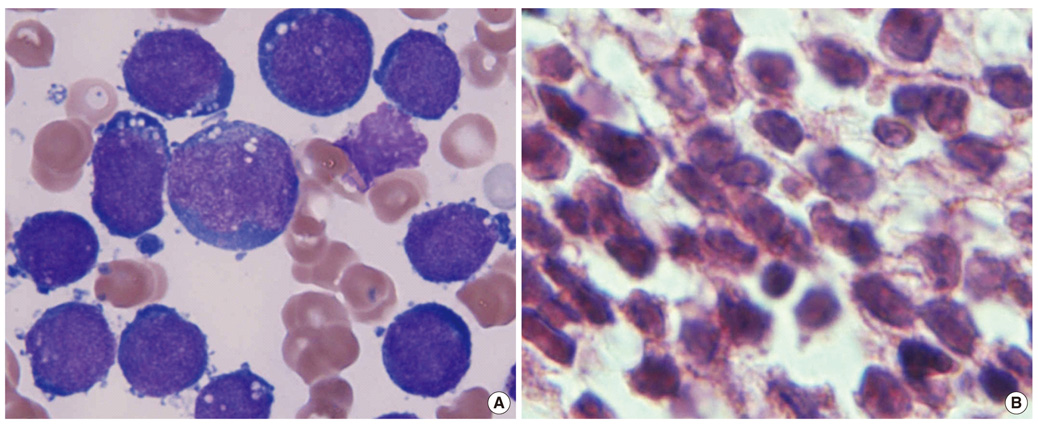
Fig. 2 Bone marrow smear (A, Wright-Giemsa stain, 1,000× magnification) and biopsy (B, H&E stain, 1,000× magnification) reveal abnormal lymphoid cells composed of large and medium sized cells. Large neoplastic cells showed irregular nuclei with 1-2 distinct nucleoli and abundant deeply basophilic cytoplasm. Medium-sized cells showed round nuclei with 1-4 prominent nucleoli and had scantly to moderately basophilic cytoplasm with some vacuoles.
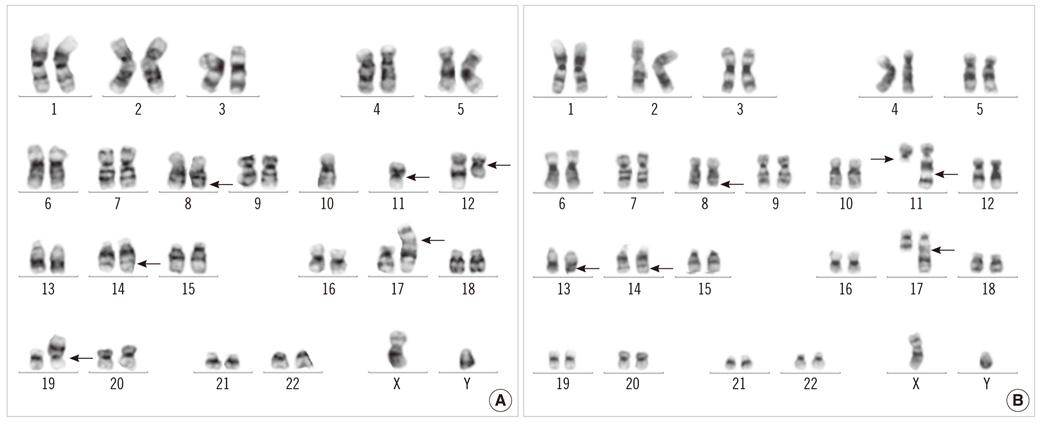
Fig. 3 Giemsa-trypsin banding showed the following karyotypes: 46,XY,t(8;14)(q24.1;q32),del(11)(q13),dup(11)(q22q13),der(17)del(17)(p12)t(1;17)(q21;q25)[29]/46,idem,t(12;19)(q13;p13.2)[4]/46,idem,add(19))(p11)[4]/46,idem,add(13)(q34)[3].
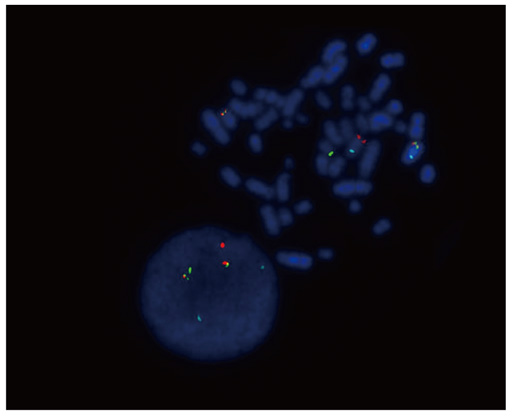
Fig. 4 FISH analysis using Vysis LSI IGH/MYC, CEP 8 tri-color, dual fusion translocation probe reveals IGH-MYC rearrangement with 2 fusions (IGH-MYC fusions on der(8)t(8;14) and der(14)t(8;14)), 1 orange (native MYC), 1 green (native IGH), and 2 aqua (D8Z2) signals.
Cited by 2 articles
-
Pediatric B-cell Lymphoma, Unclassifiable, With Intermediate Features Between Those of Diffuse Large B-cell Lymphoma and Burkitt Lymphoma: A Report of Two Cases
Shanxiang Zhang, David Wilson, Magdalena Czader
Ann Lab Med. 2015;35(2):254-256. doi: 10.3343/alm.2015.35.2.254.Primary bone lymphoma with multifocal osteolytic lesions: a rare case report with review of literature
Prakas Kumar Mandal, Shuvraneel Baul, Tuphan Kanti Dolai
Blood Res. 2015;50(4):256-260. doi: 10.5045/br.2015.50.4.256.
Reference
-
1. Hummel M, Bentink S, Berger H, Klapper W, Wessendorf S, Barth TF, et al. A biologic definition of Burkitt's lymphoma from transcriptional and genomic profiling. N Engl J Med. 2006. 354:2419–2430.
Article2. Saglio G, Bosa M, Gino M, Ulisciani S, Parvis G. Molecular pathogenesis of diffuse large B-cell lymphoma. Hematologica reports. 2006. 2:68–69.3. Carbone A, Gloghini A, Aiello A, Testi A, Cabras A. B-cell lymphomas with features intermediate between distinct pathologic entities. From pathogenesis to pathology. Hum Pathol. 2010. 41:621–631.
Article4. Kluin PM, Harris NL, Stein H, Leoncini L, Raphael M, Campo E, et al. Swerdlow SH, Campo E, editors. B-cell lymphoma, unclassifiable, with features intermediate between diffuse large B-cell lymphoma and Burkitt lymphoma. WHO classification of tumours of haematopoietic and lymphoid tissues. 2008. 4th ed. Lyon: IARC Press;265–266.5. Klapper W, Szczepanowski M, Burkhardt B, Berger H, Rosolowski M, Bentink S, et al. Molecular profiling of pediatric mature B-cell lymphoma treated in population-based prospective clinical trials. Blood. 2008. 112:1374–1381.
Article6. Salaverria I, Siebert R. The gray zone between Burkitt's lymphoma and diffuse large B-cell lymphoma from a genetics perspective. J Clin Oncol. 2011. 29:1835–1843.
Article7. Hasserjian RP, Ott G, Elenitoba-Johnson KS, Balague-Ponz O, de Jong D, de Leval L. Commentary on the WHO classification of tumors of lymphoid tissues (2008): "Gray zone" lymphomas overlapping with Burkitt lymphoma or classical Hodgkin lymphoma. J Hematop. 2009. 2:89–95.
Article8. Liang X, Greffe B, Cook B, Giller R, Graham DK, McGranahan AN, et al. Gray zone lymphomas in pediatric patients. Pediatr Dev Pathol. 2011. 14:57–63.
Article9. Patte C, Auperin A, Gerrard M, Michon J, Pinkerton R, Sposto R, et al. Results of the randomized international FAB/LMB96 trial for intermediate risk B-cell non-Hodgkin lymphoma in children and adolescents: it is possible to reduce treatment for the early responding patients. Blood. 2007. 109:2773–2780.
Article10. Quintanilla-Martinez L, de Jong D, de Mascarel A, Hsi ED, Kluin P, Natkunam Y, et al. Gray zones around diffuse large B cell lymphoma. Conclusions based on the workshop of the XIV meeting of the European Association for Hematopathology and the Society of Hematopathology in Bordeaux, France. J Hematop. 2009. 2:211–236.
Article11. Le Gouill S, Talmant P, Touzeau C, Moreau A, Garand R, Juge-Morineau N, et al. The clinical presentation and prognosis of diffuse large B-cell lymphoma with t(14;18) and 8q24/c-MYC rearrangement. Haematologica. 2007. 92:1335–1342.
Article12. Bellan C, Stefano L, Giulia de F, Rogena EA, Lorenzo L. Burkitt lymphoma versus diffuse large B-cell lymphoma: a practical approach. Hematol Oncol. 2009. 27:182–185.
Article13. Aukema SM, Siebert R, Schuuring E, van Imhoff GW, Kluin-Nelemans HC, Boerma EJ, et al. Double-hit B-cell lymphomas. Blood. 2011. 117:2319–2331.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Pediatric B-cell Lymphoma, Unclassifiable, With Intermediate Features Between Those of Diffuse Large B-cell Lymphoma and Burkitt Lymphoma: A Report of Two Cases
- Primary Burkitt's Lymphoma in the Nasal Cavity and Paranasal Sinuses
- Relapse of Ocular Lymphoma following Primary Testicular Diffuse Large B-cell Lymphoma
- Primary Cutaneous T-cell/histiocyte-rich B-cell Lymphoma
- A Case of Sporadic Nasopharyngeal Burkitt's Lymphoma
