Transcatheter Arterial Embolization of Renal VX-2 Carcinoma: Ethiodol-Ethanol Capillary Embolization Combined with Carboplatin
- Affiliations
-
- 1Vascular and Interventional Radiology, Division of Diagnostic Imaging, Unit 057, The University of Texas MD Anderson Cancer Center, TX, USA. akonya@mdanderson.org
- 2Department of Radiology, Kangnam St. Mary's Hospital, College of Medicine, The Catholic University of Korea, Seoul, Korea.
- 3Department of Veterinary Medicine and Surgery, The University of Texas MD Anderson Cancer Center, TX, USA.
- KMID: 1126837
- DOI: http://doi.org/10.3348/kjr.2007.8.2.136
Abstract
OBJECTIVE
We wanted to determine whether transcatheter Ethiodol-based capillary embolization in combination with carboplatin could improve the efficiency of a 1:1 Ethiodol-ethanol mixture (EEM) to ablate kidneys that been inoculated with VX-2 carcinoma. MATERIALS AND METHODS: The right kidney in 34 New Zealand white rabbits were inoculated with fresh VX-2 tumor fragments. One week later, the kidneys were subjected to transarterial treatment (4-5 rabbits/group): Saline infusion (Group 1); carboplatin infusion (5 or 10 mg, Groups 2A and 2B); carboplatin-Ethiodol (CE) alone (Group 3) and followed by main renal artery occlusion with ethanol (RAO) (Group 4); carboplatin-EEM (C-EEM) followed by RAO (Group 5); carboplatin infusion followed by EEM plus RAO (Group 6); and EEM followed by RAO (Group 7). The animals were followed for up to 3-weeks. The treated kidneys were evaluated angiographically and macroscopically. The kidneys that showed successful embolization macroscopically were entirely cut into serial sections, and these were examined microscopically. Histologically, the kidneys were evaluated on the basis of the residual tumor found in the serial sections. RESULTS: The results obtained with carboplatin infusion alone (Groups 2A and 2B) and CE without RAO (Group 3) were similar to those of the control animals (Group 1). Kidneys from Groups 4-7 demonstrated macroscopically successful embolization with histologically proven complete renal parenchyma infarction; however, some residual tumor was evident in all but one animal. CONCLUSION: None of the Ethiodol-based modalities combined with locoregional carboplatin were more efficacious for tumor ablation than EEM alone.
Keyword
MeSH Terms
Figure
-

Fig. 1 The amount of residual tumor remaining in the kidney at post treatment was assessed from H & E stained sections of paraffin-embedded, formalin-fixed tissues (see text). The figure contains all the slides (2/kidney) analyzed for the non-responder kidneys from Group 1 ("sham" treatment).

Fig. 2 "Sham treatment" (03L-306). A. Selective right renal arteriogram (for technical reasons, the access was created from the right carotid artery): Normal right kidney (electronic magnification 1X). B. Selective right renal arteriography: 25-day post inoculation (18-day post saline infusion): The right kidney is enormously increased in size and is completely occupied by multifocal tumors (same electronic magnification)
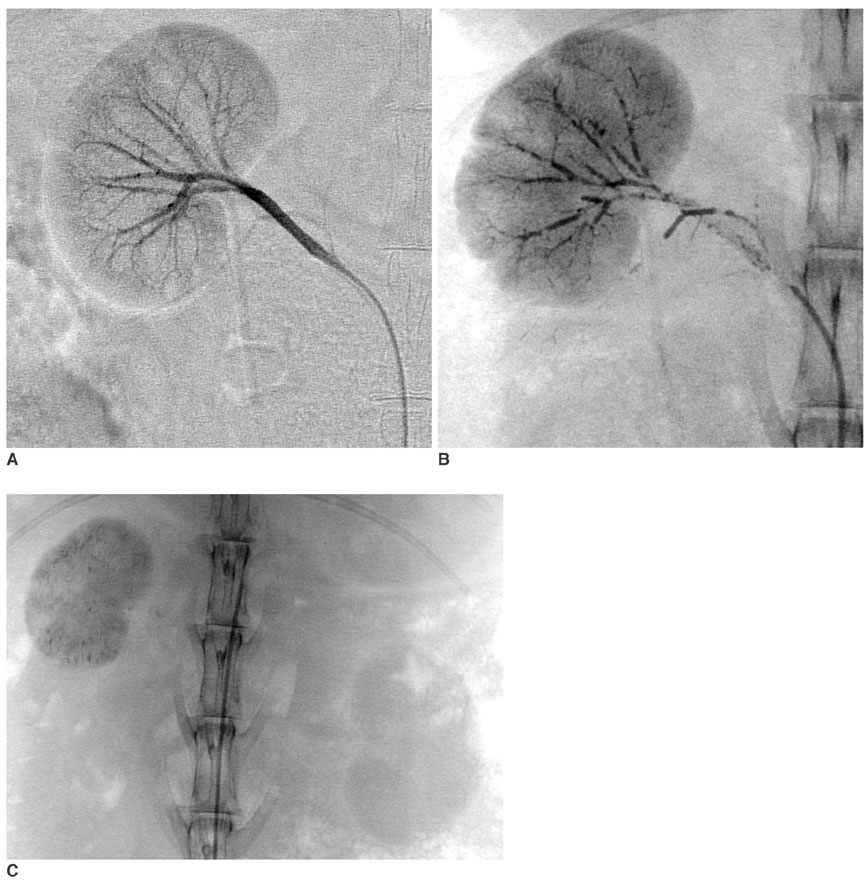
Fig. 3 Carboplatin-EEM Embolization (04L-408). A. Right renal arteriogram: Normal vasculature (electronic magnification 2X). B. Plain film obtained immediately after embolization. 0.42 mL of embolic agent completely filled the arteriocapillary system: The parenchyma stains densely and homogeneously, while the segmental-interlobar-interlobular arteries are almost contiguously filled. The EEM embolization resulted in complete arterial stasis; no ethanol was injected into the renal artery. Note that the capsular artery is also occluded. C. Plain abdominal film obtained 3-week post treatment. The right kidney is reduced in size, and its parenchymal density is almost homogeneously increased. The left kidney shows compensatory hypertrophy.

Fig. 4 EEM embolization (03L-326). A. Normal selective right renal arteriogram (magnification 1X). B. Selective right renal angiogram 1-week post VX-2 tumor inoculation: Several peripheral branches are occluded at the interlobar-interlobular-arcuate level throughout the kidney, the intensity of the parenchymal staining is slightly uneven (magnification 1X). C. Selective right renal arteriogram obtained 3-weeks post EEM embolization: The right renal artery is occluded, except for a 1-cm long stump that carries the patent capsular artery. The capsular artery increased in caliber, (its branches supply the perirenal soft tissue), but there is no parenchymal staining. Note that the right kidney is slightly reduced in size with moderately increased radiopacity, indicating residual Ethiodol and mineralization (normal view).
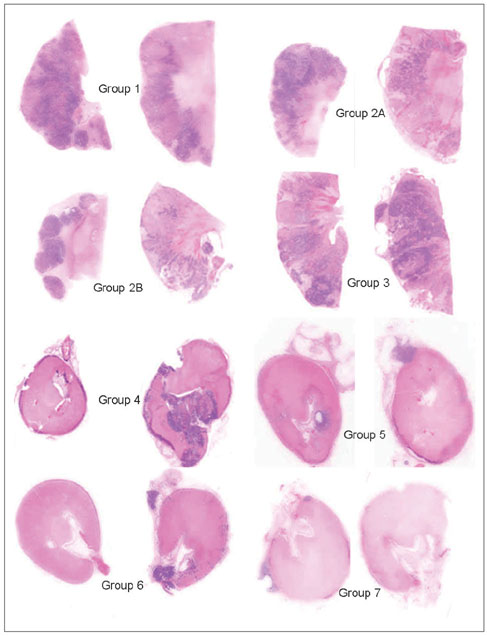
Fig. 5 A comparison of tumor retention and renal embolization between the control and treated groups. Kidney sections from two animals from each group are scanned using the HP scanjet 7400c (magnified x 2). Group 1 is the control and it has the most tumor, as demonstrated by the blue/purple areas (see also Fig. 1) and this was confirmed histologically as being VX2 carcinoma. The tumor is diffusely spread throughout the kidney. Groups 2A, 2B and Group 3 have less VX2 carcinoma than the control group, and the tumor is still distributed throughout the renal parenchyma. Groups 4, 5, 6 and 7 are all similar to each other and they are very different from Groups 1, 2A, 2B and 3. However, Group 4 appears to have more blue/purple tumor than Groups 5, 6 and 7. The kidneys of these latter 4 groups are smaller and completely embolized. The remaining tumor is not diffusely distributed throughout the parenchyma, but it is generally at the capsular surface, in the attached peri-renal fat or in the pelvis of the kidney. The blue/purple is either tumor or inflammation or mineralization, and it frequently shows all three in the sections (see Fig. 6).

Fig. 6 Embolized kidneys from Groups 6 and 7 demonstrating the pattern of tumor re-growth. A. The entire kidney is sectioned, demonstrating a smaller kidney that is completely embolized. No tumor was present in any section (score = 0) on microscopic examination. A2 (magnified x 25) and A3 (magnified x 400) demonstrate that at the capsular surface, the outermost blue/purple is mineralization (arrow), and the inner blue/purple (arrowhead) at the junction with the necrotic parenchyma is inflammation. B. The entire kidney is sectioned and this includes some adherent peri-renal fat containing blue/purple nodules (*) that are VX2 tumors. In B2 (magnified x 25), the tumor (*) is in the peri-renal fat, and the fat is separated from the renal parenchyma by blood vessels (bv) in the granulating renal capsule. The blue/purple (arrow) below the capsule is mineral on microscopy. B3 (magnified x 25) is a tumor (*) in the medulla of the same section that appears to arrive from a tumor's embolized vessel (bv). B4 (magnified x 100) demonstrated that the tumor (*) invades from the capsular surface into the pink embolized renal parenchyma.
Cited by 1 articles
-
Transcatheter Arterial Embolization in Patients with Kidney Diseases: an Overview of the Technical Aspects and Clinical Indications
Romaric Loffroy, Pramod Rao, Byung-Kook Kwak, Shinichi Ota, Ming De Lin, Eleni Liapi, Jean-François Geschwind
Korean J Radiol. 2010;11(3):257-268. doi: 10.3348/kjr.2010.11.3.257.
Reference
-
1. Cobb WS, Heniford BT, Matthews BD, Carbonell AM, Kercher KW. Advanced age is not a prohibitive factor in laparoscopic nephrectomy for renal pathology. Am J Surg. 2004. 70:537–542.2. Murphy DP, Gill IS. Energy-based renal tumor ablation: a review. Semin Urol Oncol. 2001. 19:133–140.3. Gervais DA, Arellano RS, Mueller PR. Percutaneous radiofrequency ablation of renal cell carcinoma. Eur Radiol. 2005. 15:960–967.4. Yamakado K, Nakatsuka A, Kobayashi S, Akeboshi M, Takaki H, Kariya Z. Radiofrequency ablation combined with renal arterial embolization for the treatment of unresectable renal cell carcinoma larger than 3.5 cm: initial experience. Cardiovasc Intervent Radiol. 2006. 29:389–394.5. Lanigan D, Jurriaans E, Hammonds JC, Wells IP, Choa RG. The current status of embolization in renal cell carcinoma - a survey of local and national practice. Clin Radiol. 1992. 46:176–178.6. Zielinski H, Szmigielski S, Petrovich Z. Comparison of preoperative embolization followed by radical nephrectomy with radical nephrectomy alone for renal cell carcinoma. Am J Clin Oncol. 2000. 23:6–12.7. Craven WM, Redmond PL, Kumpe DA, Durham JD, Wettlaufer JN. Planned delayed nephrectomy after ethanol embolization of renal carcinoma. J Urol. 1991. 146:704–708.8. Klimberg I, Hunter P, Hawkins IF, Drylie DM, Wajsman Z. Preoperative angioinfarction of localized renal cell carcinoma using absolute ethanol. J Urol. 1985. 133:21–24.9. Imai S, Kajihara Y, Nishishita S, Hayashi T. Effect of ethanol induced occlusion of the renal artery in rabbit kidney implanted with VX2 carcinoma. Acta Radiol. 1989. 30:535–539.10. Ellman BA, Parkhill BJ, Curry TS 3rd, Marcus PB, Peters PC. Ablation of renal tumors with absolute ethanol: a new technique. Radiology. 1981. 141:619–626.11. Park JH, Jeon SC, Kang HS, Im JG, Han MC, Kim CW. Transcatheter renal arterial embolization with the mixture of ethanol and iodized oil (Lipiodol®). Invest Radiol. 1986. 21:577–580.12. Wright KC, Loh G, Wallace S, Stephens LC. Experimental evaluation of ethanol-ethiodol for transcatheter renal embolization. Cardiovasc Intervent Radiol. 1990. 13:309–313.13. Park JH, Han JK, Chung JW, Choi BI, Han MC, Kim YI. Superselective transcatheter arterial embolization with ethanol and iodized oil for hepatocellular carcinoma. J Vasc Interv Radiol. 1993. 4:333–339.14. Konya A, Wright KC. Capillary embolization using ethiodol-ethanol for complete renal ablation in Swine. Invest Radiol. 2002. 37:512–520.15. Konya A, Van Pelt CS, Wright KC. Ethiodized oil-ethanol capillary embolization in rabbit kidneys: temporal histopathological findings. Radiology. 2004. 232:147–153.16. Kónya A, Wright KC. Ethiodol-ethanol capillary embolization in rabbit kidney implanted with VX-2 carcinoma. Radiological Society of North America (RSNA) Scientific Assembly and Annual Meeting Program 2001. Radiology. 2001. 221(P):184.17. Pohlen U, Berger G, Binnenhei M, Reszka R, Buhr HJ. Increased carboplatin concentration in liver tumors through temporary flow retardation with starch microspheres (Spherex) and gelatin powder (Gelfoam): an experimental study in liver tumor-bearing rabbits. J Surg Res. 2000. 92:165–170.18. Buchta K, Sands J, Rosenkrantz H, Roche WD. Early mechanism of action of arterially infused alcohol U.S.P. in renal devitalization. Radiology. 1982. 145:45–48.19. Konya A, Stephens CL, Wright KC. A new transcatheter method for renal ablation: pure ethiodized oil is an efficient ablative agent. 2005. In : Radiological Society of North America (RSNA) Scientific Assembly and Annual Meeting Program; 409.20. Kauffmann GW, Richter GM, Rohrbach R, Wenz W. Prolonged survival following palliative renal tumor embolization by capillary occlusion. Cardiovasc Intervent Radiol. 1989. 12:22–28.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Renal Arterial Embolization in Metastatic Renal Cell Carcinoma with Absolute Ethanol
- Renal arterial embolization with absolute ethanol
- A Comparative Study on Transcatheter Renal Arterial Embolization (TRAE) in Rabbits with Absolute Ethanol and Gelfoam Particles
- Transcatheter arterial embolization for congenital renal arteriovenous fistula
- Percutaneous transcatheter embolization
