Pure and Mixed Tubular Carcinoma of the Breast: Mammographic and Sonographic Differential Features
- Affiliations
-
- 1Department of Radiology and Research Institute of Radiology, University of Ulsan College of Medicine, Asan Medical Center, Seoul, Korea. hhkim@amc.seoul.kr
- 2Department of Pathology, University of Ulsan College of Medicine, Asan Medical Center, Seoul, Korea.
- KMID: 1126833
- DOI: http://doi.org/10.3348/kjr.2007.8.2.103
Abstract
OBJECTIVE
We wanted to evaluate the mammographic and sonographic differential features between pure (PT) and mixed tubular carcinoma (MT) of the breast. MATERIALS AND METHODS: Between January 1998 and May 2004, 17 PTs and 14 MTs were pathologically confirmed at our institution. The preoperative mammography (n = 26) and sonography (n = 28) were analyzed by three radiologists according to BI-RADS. RESULTS: On mammography, a mass was not detected in eight patients with PT and in one patient with MT (57% vs. 8%, respectively, p = 0.021), which was statistically different. The other findings on mammography and sonography showed no statistical differences between the PT and MT, although the numerical values were different. When the lesions were detected mammographically, an irregularly shaped mass with a spiculated margin was more frequently found in the MT than in the PT (100% vs. 83%, respectively, p = 0.353). On sonography, all 28 patients presented with a mass and most lesions showed as not being circumscribed, hypoechoic masses with an echogenic halo. Surrounding tissue changes and posterior shadowing were more frequently found in the MT than in the PT (75% vs. 50%, respectively, p = 0.253, 58% vs. 19%, respectively, p = 1.000). An oval shaped mass was more frequently found in the PT than in the MT (44% vs. 25%, respectively; p = 0.434). CONCLUSION: PT and MT cannot be precisely differentiated on mammography and sonography. However, the absence of a mass on mammography or the presence of an oval shaped mass would favor the diagnosis of PT. An irregularly shaped mass with surrounding tissue change and posterior shadowing on sonography would favor the diagnosis of MT and also a less favorable prognosis.
MeSH Terms
Figure
-
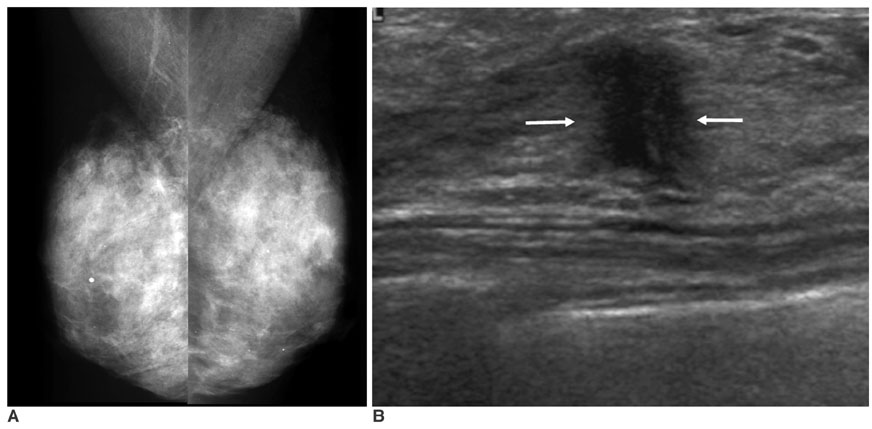
Fig. 1 A 46-year-old woman with pure tubular carcinoma (95% tubular component) with a palpable lump in the right breast. A. Mammogram shows no definite abnormal focal lesion and both breasts are diffusely dense. B. Sonography shows an approximately 0.9-cm sized, spiculated, irregularly shaped hypoechoic mass (arrows) in the subareolar area of the right breast.
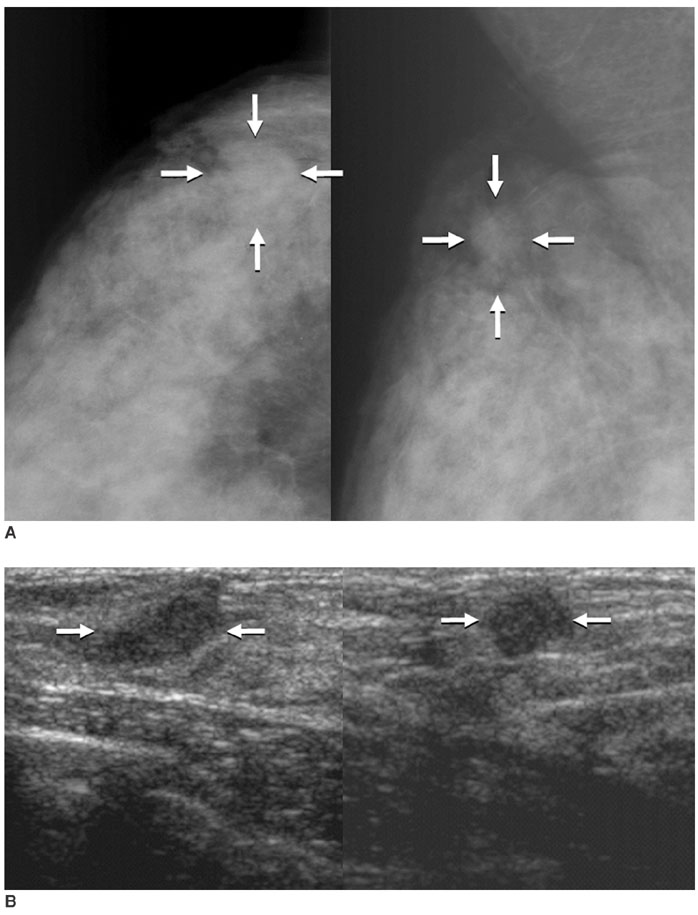
Fig. 2 A 41-year-old woman with pure tubular carcinoma (95% tubular component) with painful palpable lump in the upper outer quadrant of the right breast. A. Mammography shows an about 1.5-cm sized oval shaped isodense mass with an obscured margin (arrows) in the upper outer quadrant of the right breast. B. Sonography shows an about 1.2-cm sized oval shaped hypoechoic mass with a microlobulated margin (arrows) in the right breast.
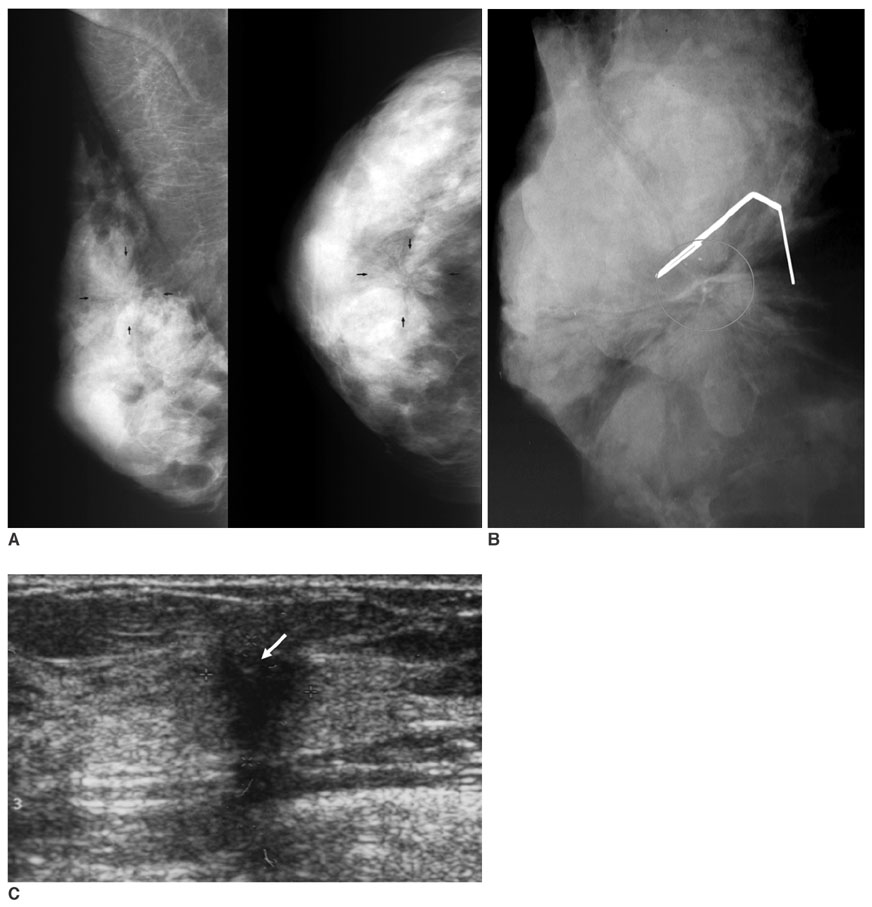
Fig. 3 A 43-year-old woman with mixed tubular carcinoma (70% tubular component) with a palpable lump in the right breast. A. Mammography shows a long spiculated mass with central lucency (arrows) in the right breast. B. Specimen mammography shows benign calcifications (circle) in the long spiculated mass. C. Sonography shows an approximately 1.2-cm sized, irregularly shaped hypoechoic mass with an indistinct margin and calcifications (arrow), and posterior shadowing.
Cited by 1 articles
-
Tubular Carcinoma of the Breast: Clinicopathologic Features and Survival Outcome Compared with Ductal Carcinoma
In Situ
Yejin Min, Soo Youn Bae, Hyun-Chul Lee, Jun Ho Lee, Minkuk Kim, Jiyoung Kim, Se Kyung Lee, Won Ho Kil, Seok Won Kim, Jeong Eon Lee, Seok Jin Nam
J Breast Cancer. 2013;16(4):404-409. doi: 10.4048/jbc.2013.16.4.404.
Reference
-
1. Tavassoli FA, Devilee P. Jaffe ES, Harris NL, Stein H, editors. Pathology and genetics. World Health Organization classification of tumours: tumours of the breast and female genital organs. 2003. Lyon: IARC Press;26–28.2. Rosen PP. Rosen's breast pathology. 2001. 2nd ed. Philadelphia: Lippincott-Williams & Wilkins;365–380.3. Deos PH, Norris HJ. Well-differentiated (tubular) carcinoma of the breast. A clinicopathologic study of 145 pure and mixed cases. Am J Clin Pathol. 1982. 78:1–7.4. Leibman AJ, Lewis M, Kruse B. Tubular carcinoma of the breast: mammographic appearance. AJR Am J Roentgenol. 1993. 160:263–265.5. Sheppard DG, Whitman GJ, Huynh PT, Sahin AA, Fornage BD, Stelling CB. Tubular carcinoma of the breast: mammographic and sonographic features. AJR Am J Roentgenol. 2000. 174:253–257.6. Elson BC, Helvie MA, Frank TS, Wilson TE, Adler DD. Tubular carcinoma of the breast: mode of presentation, mammographic appearance, and frequency of nodal metastases. AJR Am J Roentgenol. 1993. 161:1173–1176.7. American College of Radiology. Breast Imaging Reporting and Data System (BI-RADS). 2003. 4th ed. Reston, VA: American College of Radiology.8. Carstens PH, Huvos AG, Foote FW Jr, Ashikari R. Tubular carcinoma of the breast: a clinicopathologic study of 35 cases. Am J Clin Pathol. 1972. 58:231–238.9. Cooper HS, Patchefsky AS, Krall RA. Tubular carcinoma of the breast. Cancer. 1978. 42:2334–2342.10. Oberman HA, Fidler WJ Jr. Tubular carcinoma of the breast. Am J Surg Pathol. 1979. 3:387–395.11. Peters GN, Wolff M, Haagensen CD. Tubular carcinoma of the breast. Clinical pathologic correlations based on 100 cases. Ann Surg. 1981. 193:138–149.12. Carstens PH, Greenberg RA, Francis D, Lyon H. Tubular carcinoma of the breast. A long term follow-up. Histopathology. 1985. 9:271–280.13. Carstens PH. Tubular carcinoma of the breast. A study of frequency. Am J Clin Pathol. 1978. 70:204–210.14. McDivitt RW, Boyce W, Gersell D. Tubular carcinoma of the breast. Clinical and pathological observations concerning 135 cases. Am J Surg Pathol. 1982. 6:401–411.15. Lagios MD, Rose MR, Margolin FR. Tubular carcinoma of the breast: association with multicentricity, bilaterality, and family history of mammary carcinoma. Am J Clin Pathol. 1980. 73:25–30.16. Mitnick JS, Gianutsos R, Pollack AH, Susman M, Baskin BL, Ko WD, et al. Tubular carcinoma of the breast: sensitivity of diagnostic techniques and correlation with histopathology. AJR Am J Roentgenol. 1999. 172:319–323.17. Feig SA, Shaber GS, Patchefsky AS, Schwartz GF, Edeiken J, Nerlinger R. Tubular carcinoma of the breast. Mammographic appearance and pathological correlation. Radiology. 1978. 129:311–314.18. McBoyle MF, Razek HA, Carter JL, Helmer SD. Tubular carcinoma of the breast: an institutional review. Am Surg. 1997. 63:639–644.19. Vega A, Garijo F. Radial scar and tubular carcinoma. Mammographic and sonographic findings. Acta Radiol. 1993. 34:43–47.20. Mitnick JS, Vazquez MF, Harris MN, Roses DF. Differentiation of radial scar from scirrhous carcinoma of the breast: mammographic-pathologic correlation. Radiology. 1989. 173:697–700.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Radiologic Findings of Tubular Adenoma of the Breast
- Correlation of Imaging Findings with Pathologic Findings of Sclerosing Adenosis
- MR Imaging Findings and Texture Analysis of Pure and Mixed Mucinous Breast Carcinoma
- Mammographic and Sonographic Findings of Metaplastic Carcinoma of the Breast
- Analysis of X-ray Mammographic Findings of Breast Carcinoma according to Histopathologic Classification
