Diagnosing Small Hepatic Cysts on Multidetector CT: an Additional Merit of Thinner Coronal Reformations
- Affiliations
-
- 1Department of Radiology and the Research Institute of Radiological Science, Yonsei University College of Medicine, Gangnam Severance Hospital, Seoul 135-720, Korea. yjsrad97@yuhs.ac
- KMID: 1122331
- DOI: http://doi.org/10.3348/kjr.2011.12.3.341
Abstract
OBJECTIVE
We wanted to validate the additional merit of the thinner coronal reformation images from multidetector CT (MDCT) for making the diagnosis of hepatic cysts.
MATERIALS AND METHODS
For the 90 benign hepatic cysts confirmed on MRI, the transverse (5-mm thickness) and additional coronal (2-mm thickness) reformation images from MDCT were compared with each other in terms of the Hounsfield units (HUs) and the size of each hepatic cyst.
RESULTS
The attenuations (mean: 17.2 HUs, standard deviation: +/- 14.4) on the thinner coronal images were significantly lower than those (mean: 40.7 HUs; standard deviation: +/- 20.6) on the thicker transverse images for the small hepatic cysts (< or = 10 mm on the transverse image, p < 0.01). Twenty-three (79%) of the 29 cysts between 5 mm and 10 mm and 21 (51%) of 41 lesions up to 5 mm showed a mean HU value of 20 or less on the coronal reformation images.
CONCLUSION
By reducing the partial volume effect, routine coronal reformation of MDCT with a thinner section thickness can provide another merit for making a confidential diagnosis of many small sub-centimeter hepatic cysts, and these small cysts are not easily characterized on the conventional transverse images.
Keyword
MeSH Terms
-
Adult
Analysis of Variance
Contrast Media/diagnostic use
Cysts/*radiography
Female
Gadolinium DTPA/diagnostic use
Humans
Iohexol/analogs & derivatives/diagnostic use
Liver Diseases/*radiography
Magnetic Resonance Imaging/methods
Male
Middle Aged
Radiographic Image Interpretation, Computer-Assisted/*methods
Tomography, X-Ray Computed/*methods
Figure
-
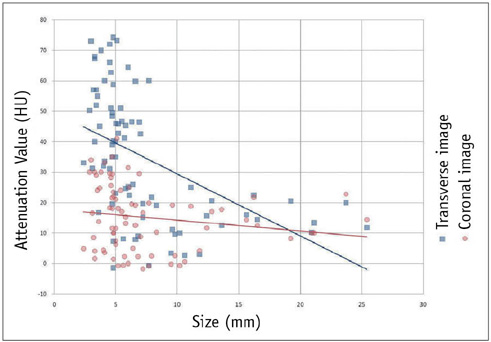
Fig. 1 Interactive dot diagram that plots attenuation values on y axis according to sizes of hepatic cysts on x axis shows significant attenuation difference between transverse and coronal images for small hepatic cysts less than 10 mm in size (p < 0.01).
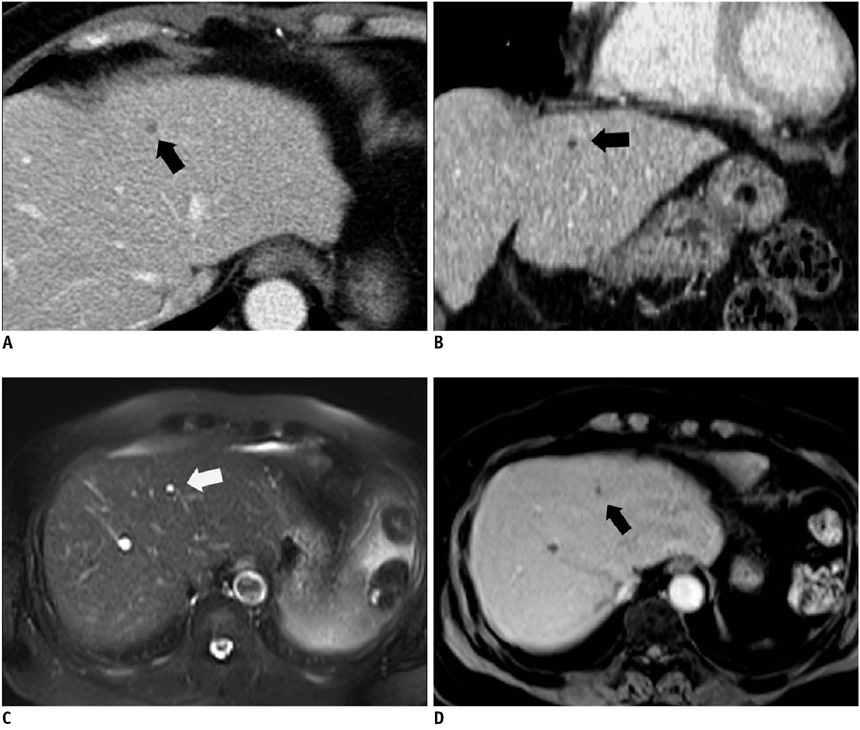
Fig. 2 50-year-old man with group I (≤ 5 mm) hepatic cyst in cirrhotic liver. A. Transverse image with 5-mm section thickness from portal venous phase contrast-enhanced CT section of abdomen reveals 4-mm hypoattenuating lesion (66 HUs), as compared with liver parenchyma, in right lobe of liver (arrow). B. Coronal image with 2-mm section thickness demonstrates that right hepatic lesion corresponding to that shown in A has 4-mm height and 30 HUs (arrow). C, D. Hepatic lesion (arrow) corresponding to that shown in A and B reveals typical appearance of hepatic cyst with markedly hyperintensity on transverse T2-weighted image (C) and no internal enhancement on transverse contrast-enhanced T1-weighted MR image (D).
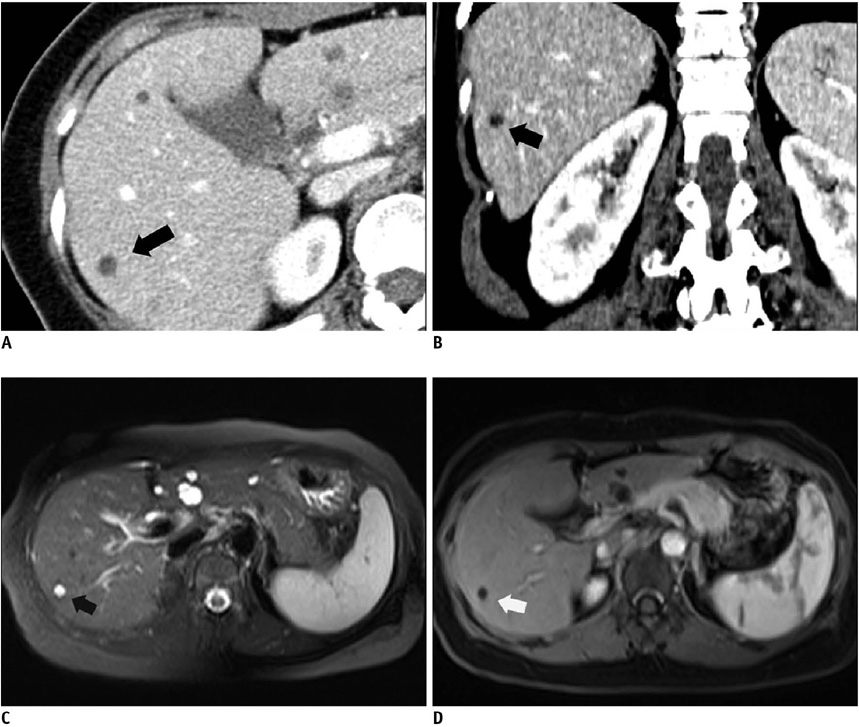
Fig. 3 41-year-old man with group II (> 5 mm and ≤ 10 mm) hepatic cyst in right lobe. A. Transverse image with 5-mm section thickness from portal venous phase contrast-enhanced CT section of abdomen reveals 7-mm hypoattenuating lesion (43 HUs), as compared with liver parenchyma, in right lobe of liver (arrow). B. Coronal image with 2-mm section thickness demonstrates that right hepatic lesion corresponding to that shown in A has 4-mm height and 9 HUs (arrow). C, D. Hepatic lesion (arrows) corresponding that shown in A and B reveals typical appearance of hepatic cyst with markedly hyperintensity on transverse T2-weighted image (C) and no internal enhancement on transverse contrast-enhanced T1-weighted MR image (D).
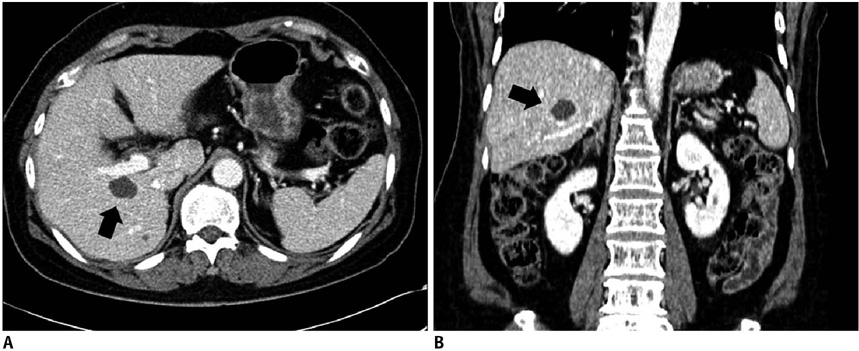
Fig. 4 60-year-old man with group III (> 10 mm) large hepatic cyst in cirrhotic liver. A. Transverse image with 5-mm section thickness from portal venous phase contrast-enhanced CT section of abdomen reveals 21-mm hypoattenuating lesion (10 HUs), as compared with liver parenchyma, in right lobe of liver (arrow). B. Coronal image with 2-mm section thickness demonstrates that right hepatic lesion corresponding to that shown in A has 16-mm height and 10 HUs (arrow).
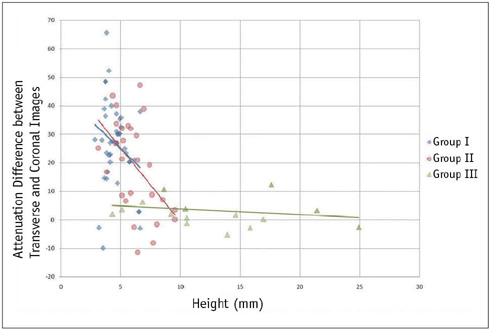
Fig. 5 Interactive dot diagram that plots attenuation differences between transverse and coronal images on y axis according to heights of hepatic cysts on x axis reveals that attenuation differences were greater for shorter lesions in group I (p = 0.02) and group II (p = 0.03).
Reference
-
1. Alfidi RJ, Haaga JR. Computed body tomography. Radiol Clin North Am. 1976. 14:563–570.2. Haaga JR, Alfidi RJ, Havrilla TR, Cooperman AM, Seidelmann FE, Reich NE, et al. CT detection and aspiration of abdominal abscesses. AJR Am J Roentgenol. 1977. 128:465–474.3. Horton KM, Bluemke DA, Hruban RH, Soyer P, Fishman EK. CT and MR imaging of benign hepatic and biliary tumors. Radiographics. 1999. 19:431–451.4. Goodenough D, Weaver K, Davis D, LaFalce S. Volume averaging limitations of computed tomography. AJR Am J Roentgenol. 1982. 138:313–316.5. Shirkhoda A. Diagnostic pitfalls in abdominal CT. Radiographics. 1991. 11:969–1002.6. Federle MP, Filly RA, Moss AA. Cystic hepatic neoplasms: complementary roles of CT and sonography. AJR Am J Roentgenol. 1981. 136:345–348.7. Jang HJ, Lim HK, Lee WJ, Lee SJ, Yun JY, Choi D. Small hypoattenuating lesions in the liver on single-phase helical CT in preoperative patients with gastric and colorectal cancer: prevalence, significance, and differentiating features. J Comput Assist Tomogr. 2002. 26:718–724.8. Patterson SA, Khalil HI, Panicek DM. MRI evaluation of small hepatic lesions in women with breast cancer. AJR Am J Roentgenol. 2006. 187:307–312.9. Paulson EK, Harris JP, Jaffe TA, Haugan PA, Nelson RC. Acute appendicitis: added diagnostic value of coronal reformations from isotropic voxels at multi-detector row CT. Radiology. 2005. 235:879–885.10. Horton KM, Fishman EK. The current status of multidetector row CT and three-dimensional imaging of the small bowel. Radiol Clin North Am. 2003. 41:199–212.11. Kundra V, Silverman PM. Impact of multislice CT on imaging of acute abdominal disease. Radiol Clin North Am. 2003. 41:1083–1093.12. Wong K, Paulson EK, Nelson RC. Breath-hold three-dimensional CT of the liver with multi-detector row helical CT. Radiology. 2001. 219:75–79.13. Caoili EM, Paulson EK. CT of small-bowel obstruction: another perspective using multiplanar reformations. AJR Am J Roentgenol. 2000. 174:993–998.14. Furukawa A, Yamasaki M, Furuichi K, Yokoyama K, Nagata T, Takahashi M, et al. Helical CT in the diagnosis of small bowel obstruction. Radiographics. 2001. 21:341–355.15. Caoili EM, Cohan RH, Korobkin M, Platt JF, Francis IR, Faerber GJ, et al. Urinary tract abnormalities: initial experience with multi-detector row CT urography. Radiology. 2002. 222:353–360.16. Prokesch RW, Chow LC, Beaulieu CF, Nino-Murcia M, Mindelzun RE, Bammer R, et al. Local staging of pancreatic carcinoma with multi-detector row CT: use of curved planar reformations initial experience. Radiology. 2002. 225:759–765.17. Jones EC, Chezmar JL, Nelson RC, Bernardino ME. The frequency and significance of small (less than or equal to 15 mm) hepatic lesions detected by CT. AJR Am J Roentgenol. 1992. 158:535–539.18. Haider MA, Amitai MM, Rappaport DC, O'Malley ME, Hanbidge AE, Redston M, et al. Multi-detector row helical CT in preoperative assessment of small (< or = 1.5 cm) liver metastases: is thinner collimation better? Radiology. 2002. 225:137–142.19. Maki DD, Birnbaum BA, Chakraborty DP, Jacobs JE, Carvalho BM, Herman GT. Renal cyst pseudoenhancement: beam-hardening effects on CT numbers. Radiology. 1999. 213:468–472.20. Birnbaum BA, Maki DD, Chakraborty DP, Jacobs JE, Babb JS. Renal cyst pseudoenhancement: evaluation with an anthropomorphic body CT phantom. Radiology. 2002. 225:83–90.21. Hong C, Bruening R, Schoepf UJ, Bae KT, Reiser MF. Multiplanar reformat display technique in abdominal multidetector row CT imaging. Clin Imaging. 2003. 27:119–123.22. Schwartz LH, Gandras EJ, Colangelo SM, Ercolani MC, Panicek DM. Prevalence and importance of small hepatic lesions found at CT in patients with cancer. Radiology. 1999. 210:71–74.23. Robinson PJ, Arnold P, Wilson D. Small "indeterminate" lesions on CT of the liver: a follow-up study of stability. Br J Radiol. 2003. 76:866–874.24. Eberhardt SC, Choi PH, Bach AM, Funt SA, Felderman HE, Hann LE. Utility of sonography for small hepatic lesions found on computed tomography in patients with cancer. J Ultrasound Med. 2003. 22:335–343. quiz 345-336.25. Mueller GC, Hussain HK, Carlos RC, Nghiem HV, Francis IR. Effectiveness of MR imaging in characterizing small hepatic lesions: routine versus expert interpretation. AJR Am J Roentgenol. 2003. 180:673–680.26. Birnbaum BA, Hindman N, Lee J, Babb JS. Multi-detector row CT attenuation measurements: assessment of intra- and interscanner variability with an anthropomorphic body CT phantom. Radiology. 2007. 242:109–119.27. Yu JS, Kim KW, Kim YH, Jeong EK, Chien D. Comparison of multishot turbo spin echo and HASTE sequences for T2-weighted MRI of liver lesions. J Magn Reson Imaging. 1998. 8:1079–1084.28. Elsayes KM, Narra VR, Yin Y, Mukundan G, Lammle M, Brown JJ. Focal hepatic lesions: diagnostic value of enhancement pattern approach with contrast-enhanced 3D gradient-echo MR imaging. Radiographics. 2005. 25:1299–1320.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Multidetector-row CT of Malignant Biliary Obstruction
- Efficacy of the Focused Ultrasound as an Additional Study to Characterize Small Hepatic Lesions on CT in Patients with Cancer
- Three-Dimensional Computed Tomography of Acetabular Fractures
- Differentiation of a Femoral Hernia from an Inguinal Hernia on Isotropic Multidetector-Row CT (MDCT): the Benefit of Inguinal Ligament Coronal-Oblique Images
- Assessment of Hepatic Arterial Variation Using Multidetector Helical CT-Angiography
