Transient Ischemic Attack and Stroke Can Be Differentiated by Analyzing the Diffusion Tensor Imaging
- Affiliations
-
- 1Department of Radiology, Fudan University Shanghai Cancer Center, The Department of Oncology, Shanghai Medical College, Fudan University, Shanghai 200032, China. t983352@126.com
- 2Department of Radiology, Huashan Hospital, Shanghai Medical College, Fudan University, Shanghai 200040, China.
- KMID: 1122325
- DOI: http://doi.org/10.3348/kjr.2011.12.3.280
Abstract
OBJECTIVE
We wanted to differentiate between transient ischemic attack (TIA) and minor stroke using fractional anisotropy and three-dimensional (3D) fiber tractography.
MATERIALS AND METHODS
The clinical data, conventional magnetic resonance imaging (MRI), diffusion weighted imaging (DWI) and diffusion tensor imaging (DTI) were obtained for 45 TIA patients and 33 minor stroke patients. The fractional anisotrophy ratio (rFA) between the lesion and the mirrored corresponding contralateral normal tissue was calculated and analyzed. The spatial relationship between the lesion and the corticospinal tract (CST) was analyzed and the lesion sizes in the minor stroke patients and TIA patients were compared.
RESULTS
Twenty-two of the 45 TIA patients (49%) revealed focal abnormalities following DWI. The rFA was significantly lower (p < 0.05) in the stroke patients (0.71 +/- 0.29) compared to that of the TIA patients (1.05 +/- 0.37). The CST was involved in almost all stroke lesions, but it was not involved in 68% of the TIA lesions. The TIA patients had significantly lower CST injury scores (3.25 +/- 1.75) than did the stroke patients (8.80 +/- 2.39) (p = 0.004).
CONCLUSION
Our data indicate that TIA and minor stroke can be identified by analyzing the rFA and the degree of CST involvement, and this may also allow more accurate prediction of a patient's long-term recovery or disability.
MeSH Terms
Figure
-
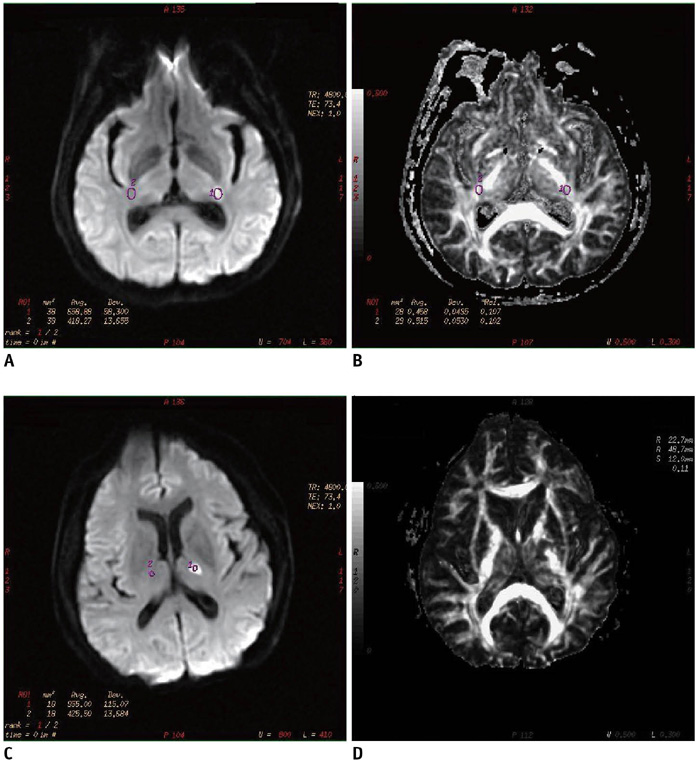
Fig. 1 Diffusion weighted imaging (A) and fractional anisotrophy (B) measurement in patient with transient ischemic attack (64-year-old man with transient right extremity weakness. Yet neurologic deficits were completely resolved in 6 h). Diffusion weighted imaging (C) and fractional anisotrophy (D) measurement in patient with stroke (50-year-old man with dysarthria and right extremity weakness). In transient ischemic attack patient, rAIb = 1000 was 1.58 and rFA was 0.89. In stroke patient, rAIb = 1000 was 2.25 and rFA was 0.57. rAIb = 1000 was significantly lower in transient ischemic attack patients compared with that of stroke patients, while rFA was significantly higher in transient ischemic attack patients compared with that of stroke patients. rAI = average signal intensity, rFA = fractional anisotrophy ratio

Fig. 2 Percentile rank map of rAIb = 1000 (A) and rFA (B) between transient ischemic attack and stroke patients at different time intervals. At all time intervals, rAIb = 1000 and rFA were significantly different in stroke patients as compared with those values in transient ischemic attack patients. rAI = average signal intensity, rFA = fractional anisotrophy ratio, TIA = transient ischemic attack

Fig. 3 Receiver operating characteristic curve analysis for rFA of transient ischemic attack and stroke patients. Area under curve shows good accuracy (0.86) for discriminating transient ischemic attack from stroke using rAI measurement on fractional anisotrophy maps. rAI = average signal intensity, rFA = fractional anisotrophy ratio, ROC curve = receiver operating characteristic curve, TIA = transient ischemic attack
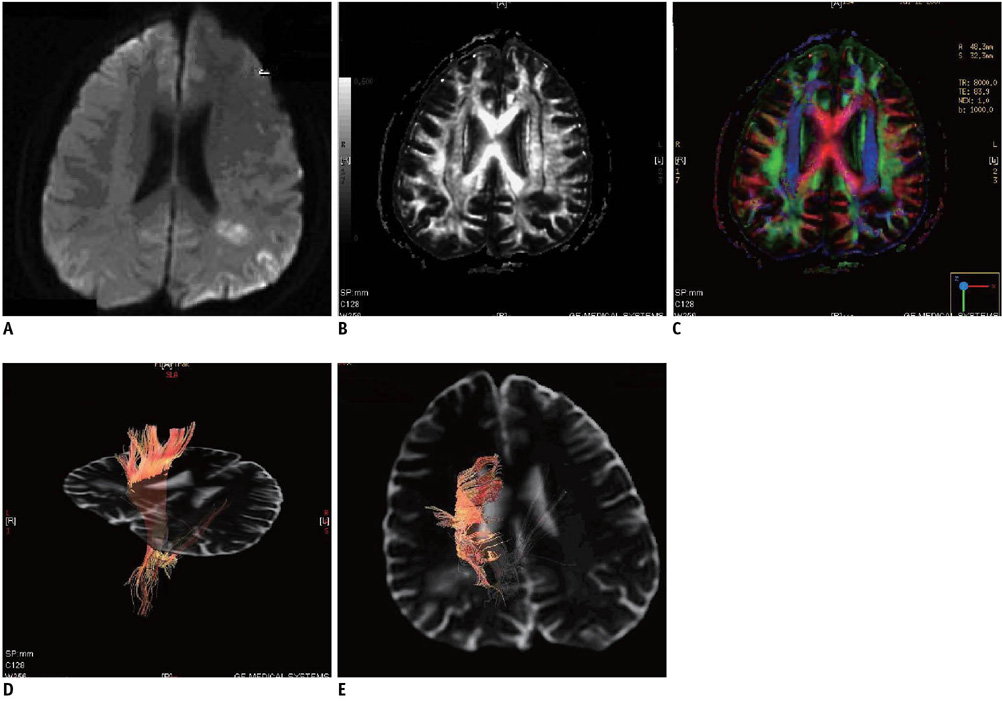
Fig. 4 Diffusion weighted imaging and diffusion tensor imaging scans from transient ischemic attack patient (53-year-old man with transient right hemisensory loss, weakness and dysarthria. Yet neurologic deficits completely resolved in 2-4 hours.) A. Axial diffusion weighted imaging showed small hyperintense lesion near left cornu posterius ventriculi lateralis. B, C. Lesion volume was 2.87 cm3. Fiber tracts reconstructed in 3-dimensional space were superimposed on fractional anisotrophy map (B) and directional encoded color map (C). D, E. Fiber tract results showed corticospinal tract (orange) of affected cerebral hemisphere appeared near lesion, but it was not running through it.
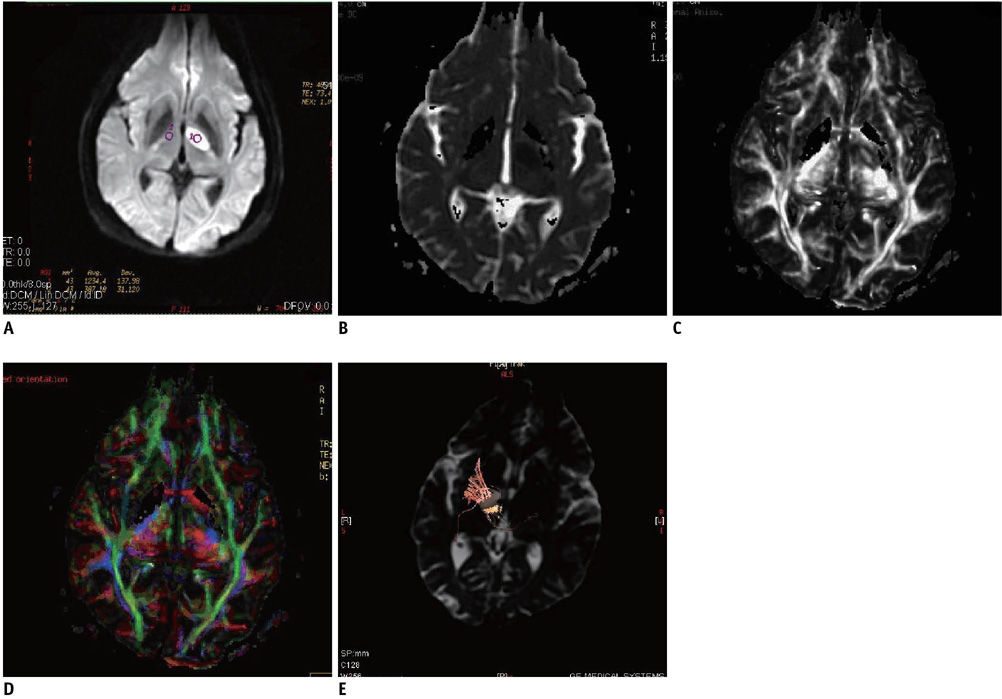
Fig. 5 Diffusion weighted imaging and diffusion tensor imaging scans from stroke patient (62-year-old man with right extremity weakness). A, B. Axial diffusion weighted imaging (A) and apparent diffusion coefficient (B) showed small hyperintense lesion on left thalamus and internal capsule. Lesion volume was 3.12 cm3. C, D. Fiber tracts reconstructed in 3-dimensional space were superimposed on fractional anisotrophy map (C) and directional encoded color map (D). E. Fiber tract results showed left corticospinal tract (orange) was only partially involved.

Fig. 6 Diffusion weighted imaging and diffusion tensor imaging scans from stroke patient (66-year-old man with left extremity weakness). A, B. Axial diffusion weighted imaging (A) and apparent diffusion coefficient (B) showed small hyperintense lesion on right thalamus and internal capsule. Lesion volume was 2.86 cm3. C, D. Fiber tracts reconstructed in 3-dimensional space were superimposed on fractional anisotrophy map (C) and directional encoded color map (D). E. Fiber tract results revealed lesion was fully involved in right corticospinal tract (orange).
Reference
-
1. Mukherjee P, Berman JI, Chung SW, Hess CP, Henry RG. Diffusion tensor MR imaging and fiber tractography: theoretic underpinnings. AJNR Am J Neuroradiol. 2008. 29:632–641.2. Mukherjee P, Chung SW, Berman JI, Hess CP, Henry RG. Diffusion tensor MR imaging and fiber tractography: technical considerations. AJNR Am J Neuroradiol. 2008. 29:843–852.3. Pierpaoli C, Barnett A, Pajevic S, Chen R, Penix LR, Virta A, et al. Water diffusion changes in Wallerian degeneration and their dependence on white matter architecture. Neuroimage. 2001. 13:1174–1185.4. Virta A, Barnett A, Pierpaoli C. Visualizing and characterizing white matter fiber structure and architecture in the human pyramidal tract using diffusion tensor MRI. Magn Reson Imaging. 1999. 17:1121–1133.5. Thomalla G, Glauche V, Koch MA, Beaulieu C, Weiller C, Rother J. Diffusion tensor imaging detects early Wallerian degeneration of the pyramidal tract after ischemic stroke. Neuroimage. 2004. 22:1767–1774.6. Ahlhelm F, Reith W. Modern diagnosis in acute cerebral infarct. Diffusion weighted imaging and ADC (apparent diffusion coefficient) calculations. Nervenarzt. 2002. 73:736–774.7. Crisostomo RA, Garcia MM, Tong DC. Detection of diffusion-weighted MRI abnormalities in patients with transient ischemic attack: correlation with clinical characteristics. Stroke. 2003. 34:932–937.8. Kidwell CS, Alger JR, Di Salle F, Starkman S, Villablanca P, Bentson J, et al. Diffusion MRI in patients with transient ischemic attacks. Stroke. 1999. 30:1174–1180.9. Ay H, Oliveira-Filho J, Buonanno FS, Schaefer PW, Furie KL, Chang YC, et al. 'Footprints' of transient ischemic attacks: a diffusion-weighted MRI study. Cerebrovasc Dis. 2002. 14:177–186.10. Marx JJ, Mika-Gruettner A, Thoemke F, Fitzek S, Fitzek C, Vucurevic G, et al. Diffusion weighted magnetic resonance imaging in the diagnosis of reversible ischaemic deficits of the brainstem. J Neurol Neurosurg Psychiatry. 2002. 72:572–575.11. Kastrup A, Schulz JB, Mader I, Dichgans J, Kuker W. Diffusion-weighted MRI in patients with symptomatic internal carotid artery disease. J Neurol. 2002. 249:1168–1174.12. Rovira A, Rovira-Gols A, Pedraza S, Grive E, Molina C, Alvarez-Sabin J. Diffusion-weighted MR imaging in the acute phase of transient ischemic attacks. AJNR Am J Neuroradiol. 2002. 23:77–83.13. Lecouvet FE, Duprez TP, Raymackers JM, Peeters A, Cosnard G. Resolution of early diffusion-weighted and FLAIR MRI abnormalities in a patient with TIA. Neurology. 1999. 52:1085–1087.14. Winbeck K, Bruckmaier K, Etgen T, von Einsiedel HG, Rottinger M, Sander D. Transient ischemic attack and stroke can be differentiated by analyzing early diffusion-weighted imaging signal intensity changes. Stroke. 2004. 35:1095–1099.15. Faraggi D, Reiser B. Estimation of the area under the ROC curve. Stat Med. 2002. 21:3093–3106.16. Nagai Y, Kitagawa K, Yamagami H, Kondo K, Hougaku H, Hori M, et al. Carotid artery intima-media thickness and plaque score for the risk assessment of stroke subtypes. Ultrasound Med Biol. 2002. 28:1239–1243.17. Sorensen AG, Wu O, Copen WA, Davis TL, Gonzalez RG, Koroshetz WJ, et al. Human acute cerebral ischemia: detection of changes in water diffusion anisotropy by using MR imaging. Radiology. 1999. 212:785–792.18. Zelaya F, Flood N, Chalk JB, Wang D, Doddrell DM, Strugnell W, et al. An evaluation of the time dependence of the anisotropy of the water diffusion tensor in acute human ischemia. Magn Reson Imaging. 1999. 17:331–348.19. Duong TQ, Ackerman JJ, Ying HS, Neil JJ. Evaluation of extra- and intracellular apparent diffusion in normal and globally ischemic rat brain via 19F NMR. Magn Reson Med. 1998. 40:1–13.20. Yamada K, Mori S, Nakamura H, Ito H, Kizu O, Shiga K, et al. Fiber-tracking method reveals sensorimotor pathway involvement in stroke patients. Stroke. 2003. 34:E159–E162.21. Easton JD, Saver JL, Albers GW, Alberts MJ, Chaturvedi S, Feldmann E, et al. Definition and evaluation of transient ischemic attack: a scientific statement for healthcare professionals from the American Heart Association/American Stroke Association Stroke Council; Council on Cardiovascular Surgery and Anesthesia; Council on Cardiovascular Radiology and Intervention; Council on Cardiovascular Nursing; and the Interdisciplinary Council on Peripheral Vascular Disease. The American Academy of Neurology affirms the value of this statement as an educational tool for neurologists. Stroke. 2009. 40:2276–2293.22. Tong T, Yao Z, Feng X. Combined diffusion- and perfusion-weighted imaging: a new way for the assessment of hemispheric transient ischemic attack patients. Int J Dev Neurosci. 2011. 29:63–69.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Small Vessel Transient Ischemic Attack and Lacunar Infarction Detected with Perfusion-Weighted MRI
- Lacunar Infarction Following Recurrent Transient Ischemic Attack During Consecutive Hemodialysis
- Selective Gray Matter Infarction in the Basal Ganglia Associated With Transient Ischemic Attack
- Transient Global Amnesia Due to Hippocampal Infarction
- Antiplatelet Therapy for Secondary Stroke Prevention in Patients with Ischemic Stroke or Transient Ischemic Attack
