Tumor Response to Transcatheter Arterial Chemoembolization in Recurrent Hepatocellular Carcinoma after Living Donor Liver Transplantation
- Affiliations
-
- 1Department of Radiology, Severance Hospital, University of Yonsei, College of Medicine, Seoul, Korea. kbsung@amc.seoul.kr
- 2Department of Radiology, Seoul Asan Medical Center, University of Ulsan, College of Medicine, Seoul, Korea.
- KMID: 1110729
- DOI: http://doi.org/10.3348/kjr.2007.8.4.320
Abstract
OBJECTIVE
To evaluate the tumor response and patient survival rate following transcatheter arterial chemoembolization (TACE) in recurrent hepatocellular carcinoma (r-HCC) after living donor liver transplantation (LDLT). MATERIALS AND METHODS: Twenty-eight patients with r-HCC underwent one or more cycles of TACE after LDLT (mean, 2.5 cycles). After a mixture of iodized oil and anti-cancer drugs was injected via the arteries feeding the tumors, these vessels were embolized with a gelatin sponge. Tumor response was determined by follow-up CT imaging on all patients four weeks after each TACE procedure. Patient survival was calculated using the Kaplan-Meier survival curve. RESULTS: After TACE, targeted tumor reduced in size by 25% or more in 19 of the 28 study patients (67.9%). However, intrahepatic recurrence or extrahepatic metastasis occurred in 21 of the 28 patients (75.0%) during the 3-month follow-up period and in 26 of the 28 patients (92.9%) during the 6-month period following TACE. Extrahepatic metastasis was noted in 18 of the 28 patients (64.3%). The 1-, 3- and 5-year survival rates following TACE were 47.9, 6.0 and 0%, respectively, with a mean survival of nine months in all patients. There were no significant complications related to TACE. CONCLUSION: TACE produces an effective tumor response for targeted r-HCC after LDLT. However, the survival rate of patients with r-HCC after LDLT is poor due to extrahepatic metastasis and intrahepatic recurrence.
MeSH Terms
-
Adult
Aged
Antineoplastic Agents/administration & dosage
Carcinoma, Hepatocellular/blood supply/mortality/*therapy
*Chemoembolization, Therapeutic
Cisplatin/administration & dosage
Contrast Media/administration & dosage
Female
Follow-Up Studies
Humans
Iodized Oil/administration & dosage
Liver Neoplasms/blood supply/mortality/*therapy
Liver Transplantation
Living Donors
Male
Middle Aged
Neoplasm Metastasis
Neoplasm Recurrence, Local/mortality/*therapy
Survival Rate
Figure
-
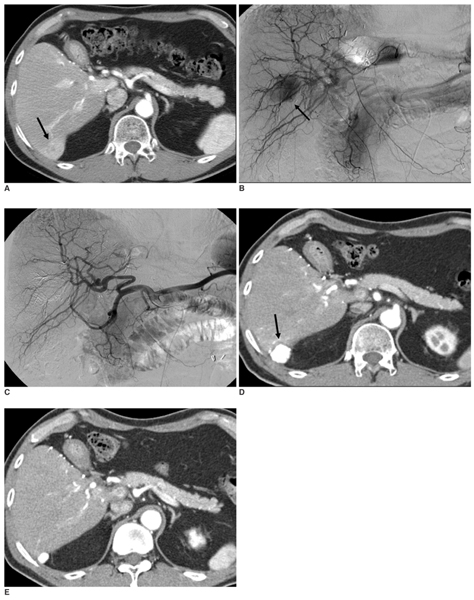
Fig. 1 A.Contrast-enhanced arterial-phase axial CT image of the liver 17 months after living donor liver transplantation shows the single arterial enhancing mass (arrow) in the posterior portion of the transplanted liver. B.Arteriogram from the celiac trunk (late arterial phase) shows an area of tumor blush in the transplanted liver (arrow). C.Arteriogram from the celiac trunk immediately after embolization shows that the tumor blush has disappeared. D.Contrast-enhanced arterial-phase axial CT image of the liver one month after transcatheter arterial chemoembolization reveals complete iodized oil accumulation (arrow) in the tumor. We interpreted this patient as having CR. E.Contrast-enhanced arterial-phase axial CT image of the liver 22 months after transcatheter arterial chemoembolization shows a decrease in the size of the recurrent hepatocellular carcinoma with iodized oil accumulation.
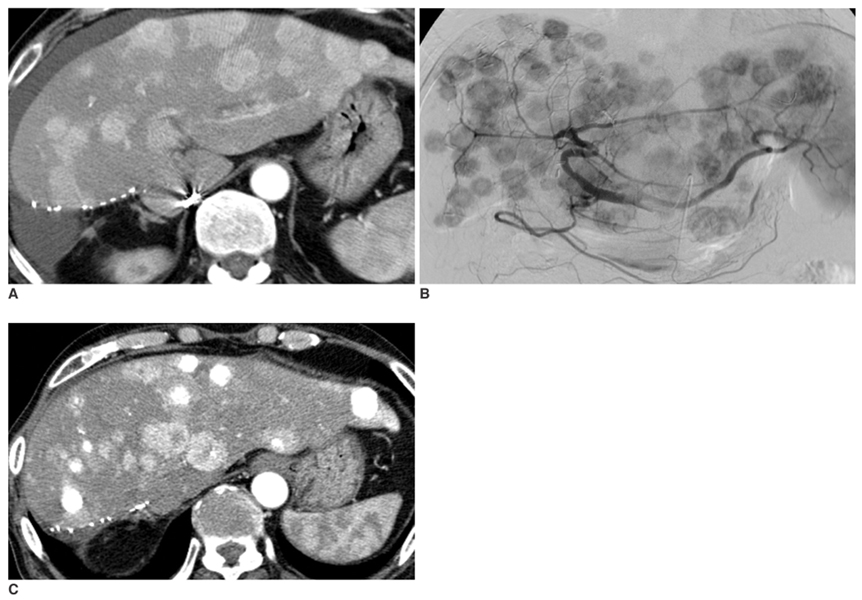
Fig. 2 A.Contrast-enhanced delayed-phase axial CT image of a transplanted liver six months after living donor liver transplantation, with the left lobe showing multiple recurrent hepatocellular carcinomas in the entire transplanted liver; however, blood flow is preserved in the portal vein. B.Arteriogram from the celiac trunk (late arterial phase) shows multiple hypervascular tumors in the entire transplanted liver. C.Contrast-enhanced arterial-phase axial CT image of the transplanted liver one month after transcatheter arterial chemoembolization shows progression of the recurrent hepatocellular carcinomas in both size and number. Some nodules show partial accumulation of iodized oil. We interpreted this patient as having progressive disease.
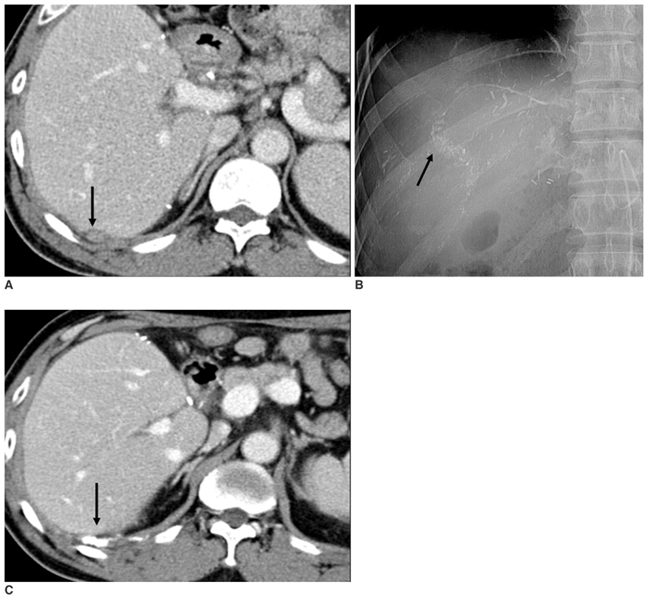
Fig. 3 A.Contrast-enhanced delayed-phase axial CT image of the liver after living donor liver transplantation reveals a small nodule in the extrahepatic space of the transplanted liver (arrow). This patient had an elevated alpha fetoprotein level at that time. B.Digital image of the intercostal and right inferior phrenic arteries after transcatheter arterial chemoembolization shows subtle accumulation of iodized oil (arrow). C.Contrast-enhanced arterial-phase axial CT image of a transplanted liver one month after transcatheter arterial chemoembolization shows completed accumulation of iodized oil in the nodule (arrow). This patient's alpha fetoprotein level decreased after transcatheter arterial chemoembolization.
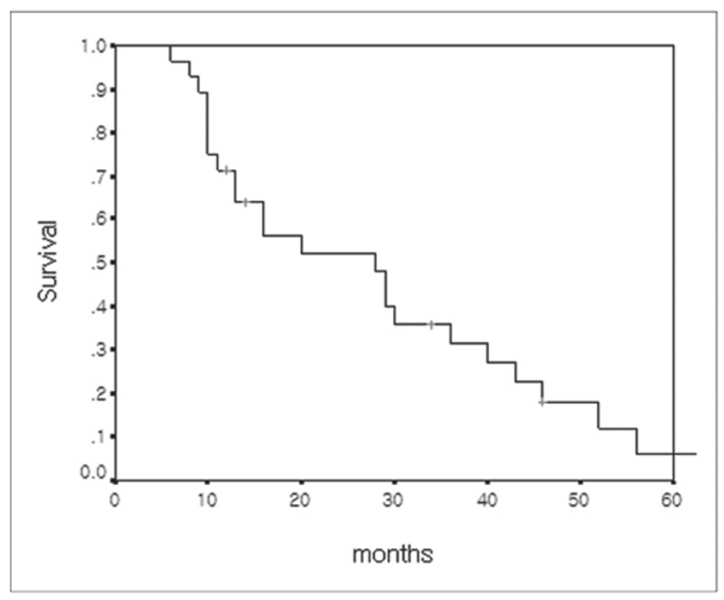
Fig. 4 Overall cumulative survival curve of 28 patients with recurrent hepatocellular carcinoma calculated from the time of living donor liver transplantation.
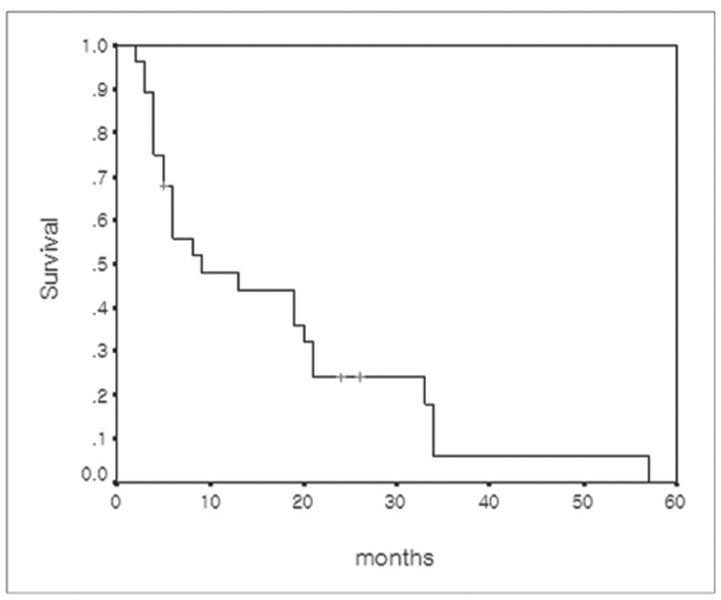
Fig. 5 Cumulative survival curve of 28 patients with recurrent hepatocellular carcinoma calculated from the time of recurrent hepatocellular carcinoma diagnosis.
Reference
-
1. Kaihara S, Kiuchi T, Ueda M, Oike F, Fujimoto Y, Ogawa K, et al. Living-donor liver transplantation for hepatocellular carcinoma. Transplantation. 2003. 75:S37–S40.2. Kulik L, Abecassis M. Living donor liver transplantation for hepatocellular carcinoma. Gastroenterology. 2004. 127:S277–S282.3. O'Grady JG, Polson RJ, Rolles K, Calne RY, Williams R. Liver transplantation for malignant disease. Results in 93 consecutive patients. Ann Surg. 1988. 207:373–379.4. Ringe B, Pichlmayr R, Wittekind C, Tusch G. Surgical treatment of hepatocellular carcinoma: experience with liver resection and transplantation in 198 patients. World J Surg. 1991. 15:270–285.5. Bismuth H, Chiche L, Adam R, Castaing D, Diamond T, Dennison A. Liver resection versus transplantation for hepatocellular carcinoma in cirrhotic patients. Ann Surg. 1993. 218:145–151.6. Tan KC, Rela M, Ryder SD, Rizzi PM, Karani J, Portmann B, et al. Experience of orthotopic liver transplantation and hepatic resection for hepatocellular carcinoma of less than 8 cm in patients with cirrhosis. Br J Surg. 1995. 82:253–256.7. Todo S, Furukawa H. Living donor liver transplantation for adult patients with hepatocellular carcinoma: experience in Japan. Ann Surg. 2004. 240:451–459. discussion 459-461.8. Gondolesi GE, Roayaie S, Munoz L, Kim-Schluger L, Schiano T, Fishbein TM, et al. Adult living donor liver transplantation for patients with hepatocellular carcinoma: extending UNOS priority criteria. Ann Surg. 2004. 239:142–149.9. Regalia E, Fassati LR, Valente U, Pulvirenti A, Damilano I, Dardano G, et al. Pattern and management of recurrent hepatocellular carcinoma after liver transplantation. J Hepatobiliary Pancreat Surg. 1998. 5:29–34.10. Schwartz M, Roayaie S, Llovet J. How should patients with hepatocellular carcinoma recurrence after liver transplantation be treated? J Hepatol. 2005. 43:584–589.11. Margarit C, Charco R, Hidalgo E, Allende H, Castells L, Bilbao I. Liver transplantation for malignant diseases: selection and pattern of recurrence. World J Surg. 2002. 26:257–263.12. Mazzaferro V, Regalia E, Doci R, Andreola S, Pulvirenti A, Bozzetti F, et al. Liver transplantation for the treatment of small hepatocellular carcinomas in patients with cirrhosis. N Engl J Med. 1996. 334:693–699.13. Atiq OT, Kemeny N, Niedzwiecki D, Botet J. Treatment of unresectable primary liver cancer with intrahepatic fluorodeoxyuridine and mitomycin C through an implantable pump. Cancer. 1992. 69:920–924.14. Llovet JM, Bruix J. Systematic review of randomized trials for unresectable hepatocellular carcinoma: chemoembolization improves survival. Hepatology. 2003. 37:429–442.15. Llovet JM, Burroughs A, Bruix J. Hepatocellular carcinoma. Lancet. 2003. 362:1907–1917.16. Bruix J, Sala M, Llovet JM. Chemoembolization for hepatocellular carcinoma. Gastroenterology. 2004. 127:S179–S188.17. Ebied OM, Federle MP, Carr BI, Pealer KM, Li W, Amesur N, et al. Evaluation of responses to chemoembolization in patients with unresectable hepatocellular carcinoma. Cancer. 2003. 97:1042–1050.18. Roayaie S, Schwartz JD, Sung MW, Emre SH, Miller CM, Gondolesi GE, et al. Recurrence of hepatocellular carcinoma after liver transplant: patterns and prognosis. Liver Transpl. 2004. 10:534–540.19. Yokoyama I, Carr B, Saitsu H, Iwatsuki S, Starzl TE. Accelerated growth rates of recurrent hepatocellular carcinoma after liver transplantation. Cancer. 1991. 68:2095–2100.20. Steininger R, Herbst F, Fugger R, Muhlbacher F, Fritsch A. Immunosuppression does not enhance tumor growth after orthotopic liver transplantation for hepatoma. Transplant Proc. 1992. 24:2690–2692.21. Ishii H, Furuse J, Kinoshita T, Konishi M, Nakagohri T, Takahashi S, et al. Extrahepatic spread from hepatocellular carcinoma: who are candidates for aggressive anti-cancer treatment? Jpn J Clin Oncol. 2004. 34:733–739.22. Chung YH, Song IH, Song BC, Lee GC, Koh MS, Yoon HK, et al. Combined therapy consisting of intraarterial cisplatin infusion and systemic interferon-alpha for hepatocellular carcinoma patients with major portal vein thrombosis or distant metastasis. Cancer. 2000. 88:1986–1991.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Rupture of hepatocellular carcinoma after transcatheter arterial chemoembolization: A case report
- Liver transplantation for hepatocellular carcinoma with portal vein tumor thrombosis
- Indication and Outcome of Liver Transplantation In Patients with Hepatocellular Carcinoma
- Palliative Transcatheter Arterial Chemoembolization for Relieving Metastatic Bone Pain due to Hepatocellular Carcinoma: A Case Report
- Hepatocellular Carcinoma Extending to the Inferior Vena Cava and Right Atrium-A Case Report of 4 Years Survival after Repeated Transcatheter Arterial Chemoembolization Therapy -
