Follow-up CT Evaluation of the Mural Changes in Active Takayasu Arteritis
- Affiliations
-
- 1Department of Radiology, Seoul National University College of Medicine, the Institute of Radiation Medicine, Seoul National University Medical Research Center and Clinical Research Institute, Seoul National University Hospital, Seoul, Korea. parkjh@radcom
- KMID: 1110725
- DOI: http://doi.org/10.3348/kjr.2007.8.4.286
Abstract
OBJECTIVE
We wanted to evaluate the mural changes by CT on the follow-up examination of patients with active Takayasu arteritis. MATERIALS AND METHODS: The study included 18 patients, (4 males and 14 females), with active Takayasu arteritis. A total of 44 CT examinations were done during the follow-up period (mean: 55.6 months). At the time of the last follow-up CT, the disease, on the basis of the erythrocyte sedimentation rate (ESR), was found to be inactive in five patients and the disease was active and persistent in 13 patients. The thickness and CT attenuation of the aortic wall on the precontrast, arterial and venous phases were measured on the initial and the follow-up CT examinations. The ratio of the mural attenuation over that of the back muscle on the initial CT was compared with the ratio found on the follow-up CT. RESULTS: The initial CT findings included high density and calcifications of the aortic wall in the precontrast images and a thickened wall with enhancements in the arterial and the venous phases. A low-attenuation ring was demonstrated in the venous phase in 15 patients (83%). On the follow-up evaluation, the mean mural thickness decreased significantly from 4.1 mm to 2.4 mm. The mean mural attenuation ratio in the venous phase decreased significantly from 1.9 to 1.3 (p = 0.001). The low attenuation ring was identified in seven patients (39%) who had only with active, persistent Takayasu arteritis. CONCLUSION: The mural changes demonstrated by the follow-up CT evaluations for the patients with active Takayasu arteritis included a decrease of the mural thickness and enhancement, disappearance of the low-attenuation ring on the venous phase, and an increase of the mural attenuation and calcification on the precontrast phase.
MeSH Terms
Figure
-
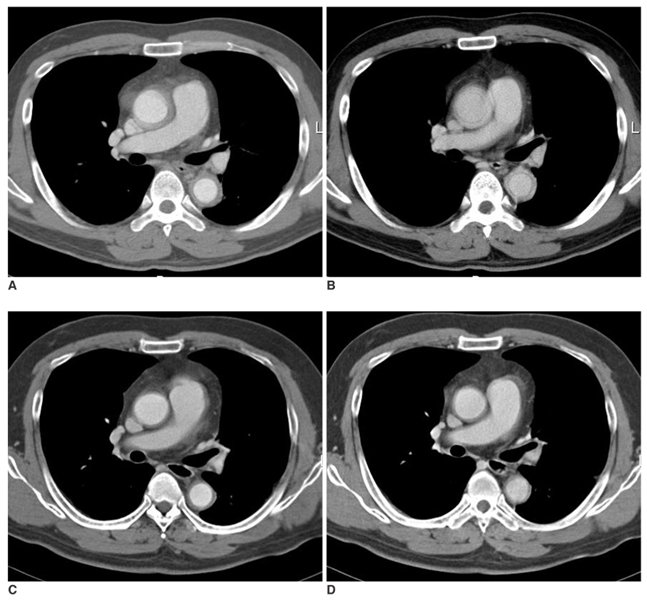
Fig. 1 A 34-year-old male patient with Takayasu arteritis (Case 7). The initial CT of the arterial phase at the level of the right pulmonary artery (A) reveals a mural thickening of the ascending and the descending aorta. In the venous phase (B), the thickened wall is enhanced with a inner low-attenuation ring. The follow-up CT evaluation made six years, four months after the initial CT reveals a significantly decreased mural thickness on the arterial phase (C). The CT image of the same level on the venous phase (D) shows a decrease of the thickness and enhancement of the aortic wall with disappearance of the inner low-attenuation ring.
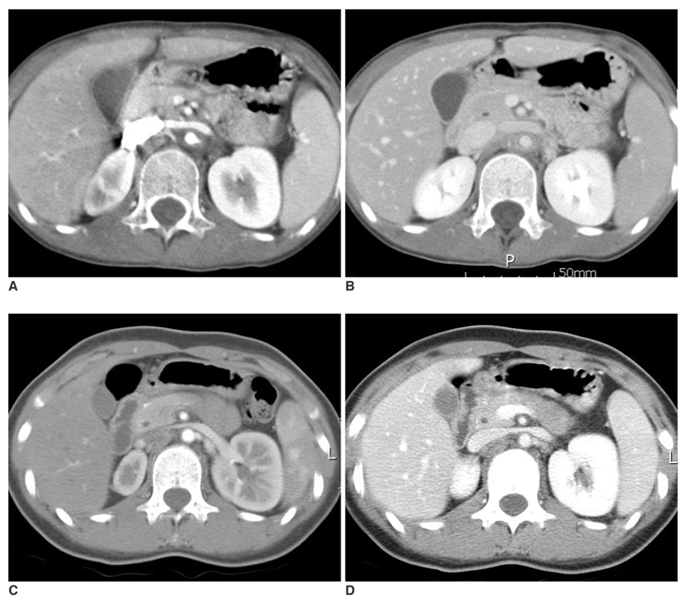
Fig. 2 An 11-year-old female patient with Takayasu arteritis (Case 1). Abdominal CT of the arterial phase at the level of the renal vein (A) shows a concentric wall thickening of the aorta at the origin of the left renal artery. On the venous phase (B), the wall is enhanced significantly with a low-attenuation ring. After three years, seven months, the follow-up CT on the arterial phase (C) and the venous phase (D) reveals a marked decrease of the mural thickening. The disease was defined as inactive at the time of the follow-up CT, with normal erythrocyte sedimentation rate without steroid treatment. Focal stenosis developed at the proximal left renal artery, which was later successfully treated with percutaneous balloon angioplasty.
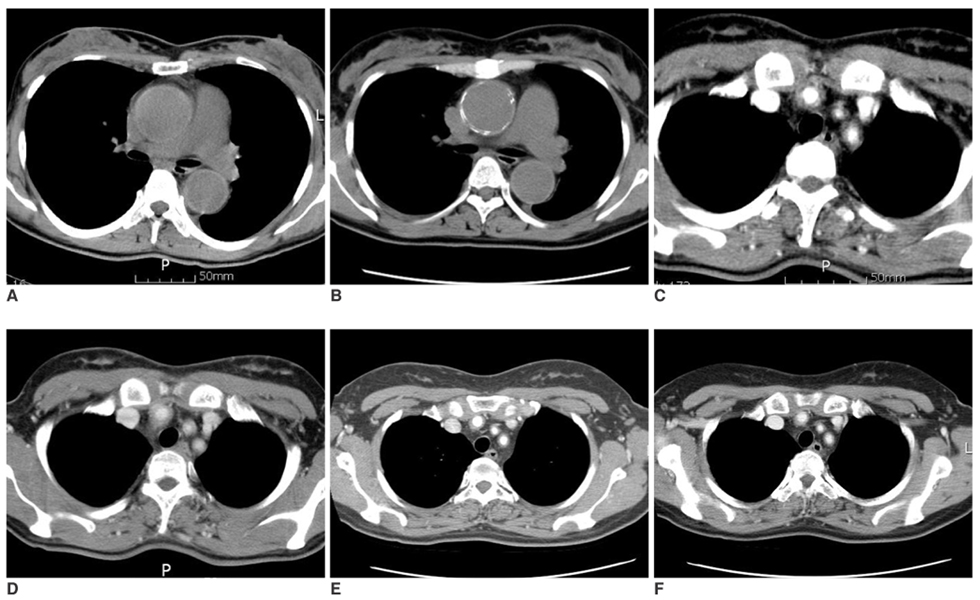
Fig. 3 A 40-year-old female patient with Takayasu arteritis (Case 9). In comparison with the initial precontrast CT (A), the follow-up CT at five years, two months reveals a progressive calcification of the ascending aorta that was noted (B). Transverse CT of the arch vessels demonstrates significant wall thickening on the arterial phase (C) and enhancement on the venous phase (D) at the time of the initial study. The mural changes were found to persist on the follow-up CT of the arterial phase (E) and the venous phase (F) even after five years two months of steroid treatment.
Reference
-
1. Herrera EL, Seoane M. Lande A, Berkmen YM, McAllister HA, editors. Takayasu's arteritis (nonspecific aortitis). Aortitis: clinical, pathologic, and radiographic aspects. 1986. New York: Raven Press;173–191.2. Arend WP, Michel BA, Bloch DA, Hunder GG, Calabrese LH, Edworthy SM, et al. The american college of rheumatology 1990 criteria for the classification of Takayasu arteritis. Arthritis Rheum. 1990. 8:1129–1134.3. Park JH, Han MC, Kim SH, Oh BH, Park YB, Seo JD. Takayasu arteritis: angiographic findings and results of angioplasty. AJR Am J Roentgenol. 1989. 153:1069–1074.4. Mandalam KR, Joseph S, Rao VR, Gupta AK, Unni NM, Rao AS, et al. Aortoarteritis of abdominal aorta: an angiographic profile in 110 patients. Clini Radiol. 1993. 48:29–34.5. Hayashi K, Fukushima T, Matsunaga N, Hombo Z. Takayasu arteritis: decrease in aortic wall thickening following steroid therapy, documented by CT. Br J Radiol. 1986. 59:281–283.6. Park JH, Chung JW, Im JG, Kim SK, Park YB, Han MC. Takayasu arteritis: evaluation of mural changes in the aorta and pulmonary artery with CT angiography. Radiology. 1995. 196:89–93.7. Kerr GS, Hallahan CW, Giordano J, Leavitt RY, Fauci AS, Rottem M, et al. Takayasu arteritis. Ann Intern Med. 1994. 120:919–929.8. Paul JF, Fiessinger JN, Sapoval M, Hernigou A, Mousseaux E, Emmerich J, et al. Follow-up electron beam CT for the management of early phase Takayasu arteritis. J Comput Assist Tomogr. 2001. 25:924–931.9. Kissin EY, Merkel PA. Diagnostic imaging in Takayasu arteritis. Curr Opin Rheumatol. 2004. 16:31–37.10. Wagner AD, Andresen J, Raum E, Lotz J, Zeidler H, Kuipers JG, et al. Standardized work-up programme for fever of unknown origin and contribution of magnetic resonance imaging for the diagnosis of hidden systemic vasculitis. Ann Rheum Dis. 2005. 64:105–110.11. Park SH, Chung JW, Lee JW, Han MH, Park JH. Carotid artery involvement in Takayasu's arteritis: evaluation of the activity by ultrasonography. J Ultrasound Med. 2001. 20:371–378.12. Tanigawa K, Eguchi K, Kitamura Y, Kawakami A, Ida H, Yamashita S, et al. Magnetic resonance imaging detection of aortic and pulmonary artery wall thickening in the acute stage of Takayasu arteritis. Improvement of clinical and radiologic findings after steroid therapy. Arthritis Rheum. 1992. 35:476–480.13. Choe YH, Han BK, Koh EM, Kim DK, Do YS, Lee WR. Takayasu's arteritis: assessment of disease activity with contrast-enhanced MR imaging. AJR Am J Roentgenol. 2000. 175:505–511.14. Virmani R, Lande A, McAllister HA. Lande A, Berkmen YM, McAllister HA, editors. Pathological aspects of Takayasu's arteritis. Aortitis: clinical, pathologic, and radiographic aspects. 1986. New York: Raven Press;173–191.15. Wintersperger B, Jakobs T, Herzog P, Schaller S, Nikolaou K, Suess C, et al. Aorto-iliac multidetector-row CT angiography with low kV settings: improved vessel enhancement and simultaneous reduction of radiation dose. Eur Radiol. 2005. 15:334–341.16. Kalva SP, Sahani DV, Hahn PF, Saini S. Using the K-edge to improve contrast conspicuity and to lower radiation dose with a 16-MDCT: a phantom and human study. J Comput Assist Tomogr. 2006. 30:391–397.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Takayasu's Arteritis: report of 2 cases and review of literature
- A Case Report of Takayaeu's Arteritis Associated with, a Retinopathy
- Aortographic findings of Takayasu's arteritis
- A Case of Takayasu Arteritis with Renovascular Hypertension
- FDG PET-CT in the Diagnosis of Takayasu Arteritis Presenting as Fever of Unknown Origin: A Case Report
