Fundamental Elements for Successful Performance of CT Colonography (Virtual Colonoscopy)
- Affiliations
-
- 1Department of Radiology and the Research Institute of Radiology, University of Ulsan College of Medicine, Asan Medical Center, Seoul, Korea. seongho@amc.seoul.kr
- 2Department of Radiology, University of California at San Francisco, San Francisco Veterans Administration Medical Center, 4150 Clement St., San Francisco, Canada.
- 3Department of Radiology and the Institute of Radiation Medicine, Seoul National University Hospital, Seoul, Korea.
- 4Department of Radiology, Seoul National University Bundang Hospital, Seongnam-si, Korea.
- KMID: 1110723
- DOI: http://doi.org/10.3348/kjr.2007.8.4.264
Abstract
- There are many factors affecting the successful performance of CT colonography (CTC). Adequate colonic cleansing and distention, the optimal CT technique and interpretation with using the newest CTC software by a trained reader will help ensure high accuracy for lesion detection. Fecal and fluid tagging may improve the diagnostic accuracy and allow for reduced bowel preparation. Automated carbon dioxide insufflation is more efficient and may be safer for colonic distention as compared to manual room air insufflation. CT scanning should use thin collimation of < or =3 mm with a reconstruction interval of < or =1.5 mm and a low radiation dose. There is not any one correct method for the interpretation of CTC; therefore, readers should be well-versed with both the primary 3D and 2D reviews. Polyps detected at CTC should be measured accurately and reported following the "polyp size-based" patient management system. The time-intensive nature of CTC and the limited resources for training radiologists appear to be the major barriers for implementing CTC in Korea.
Keyword
MeSH Terms
Figure
-

Fig. 1 A 68-year-old male with fecal residue that is tagged with orally-administered barium. A. 3D endoluminal view shows an 8-mm polypoid structure (arrowhead) on a haustral fold of the sigmoid colon. B. 2D transverse image using a wide-window setting (width: 1500 HU, level: -400 HU) shows very high attenuation of the olypoid structure (white arrowhead), which clearly demonstrates it is tagged stool. Another piece of tagged stool is noted in the sigmoid colon (black arrowhead).

Fig. 2 A 42-year-old male with fecal residue that is tagged with orally-administered gastrografin. A. 3D endoluminal view shows a 10-mm polypoid structure (arrowhead) in the descending colon. B. 2D transverse image with using a wide-window setting (width: 1500 HU, level: -400 HU) shows very high attenuation of the polypoid structure (arrowhead), and this consistent with tagged stool.

Fig. 3 A 65-year-old male with a 6-mm tubulovillous adenoma in the sigmoid colon. A. Optical colonoscopy shows a sessile polyp (arrowhead) in the sigmoid colon. B. 3D supine endoluminal view shows the corresponding polyp (arrowhead) in a well-distended segment of the sigmoid colon. C. 3D endoluminal view of the same area as figure B, with the patient in a prone position, shows the same lesion (arrowhead) obscured by suboptimal distention.
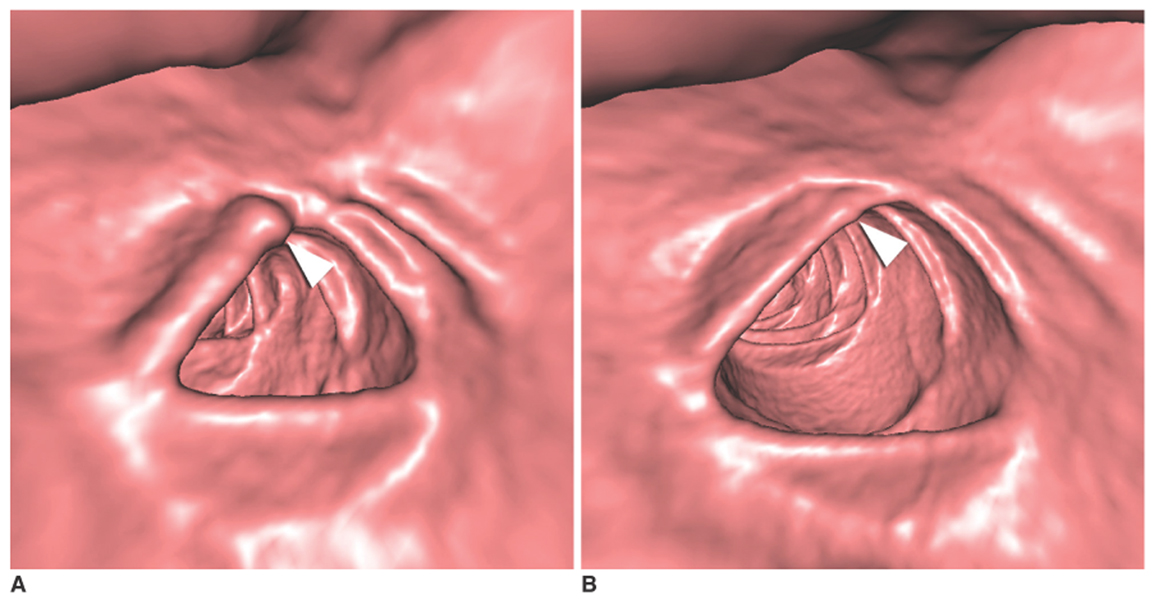
Fig. 4 A 68-year-old female with a pseudopolyp in the transverse colon. A. 3D prone endoluminal view shows focal bulbous thickening (arrowhead) of a haustral fold in the suboptimally-distended transverse colon, which resembles a sessile polyp. B. 3D endoluminal view of the same area as figure A, with the patient in a supine position, shows the disappearance of the pseudopolyp (arrowhead) when the colon is well-distended.
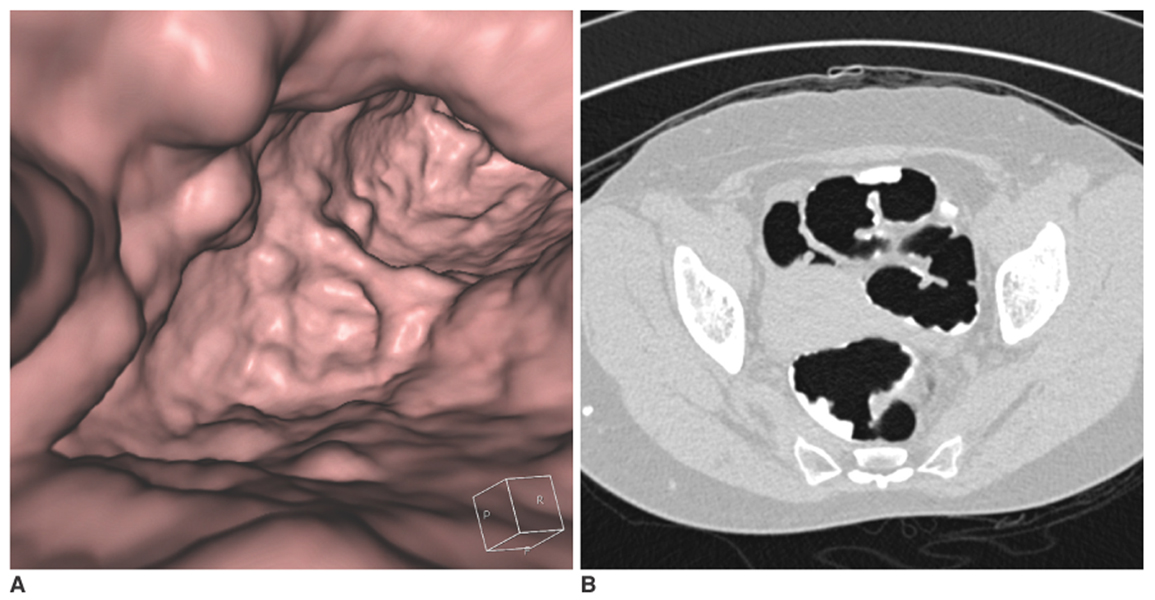
Fig. 5 A 54-year-old female with a large amount of tagged fecal residue in the sigmoid colon. A. The 3D endoluminal view shows many polypoid and mass-like structures in the sigmoid colon. Examining each polypoid or mass-like structure to distinguish a true polyp/mass from fecal residue is tiresome. Additionally, lesions buried under fecal material are not detected at all during the 3D fly-through. B. Using a wide-window setting (width: 1500 HU, level: -400 HU) for the 2D transverse image, all the pseudolesions (i.e. tagged fecal residue) are easily recognized.
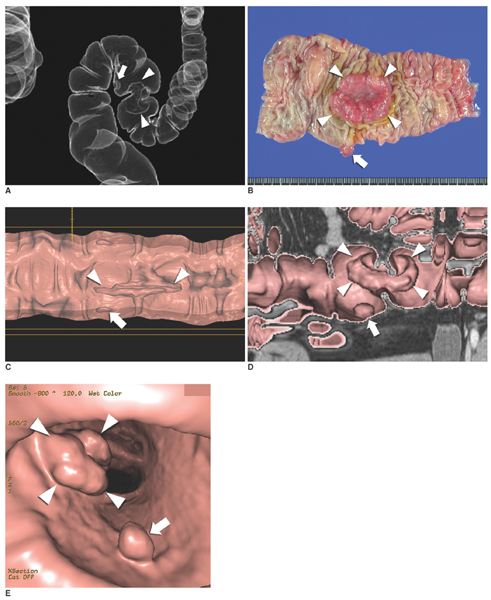
Fig. 6 A 53-year-old male with an adenocarcinoma and a tubular adenoma in the sigmoid colon. A. The locations of the adenocarcinoma (arrowheads) and the tubular adenoma (arrow) in the sigmoid colon are clearly demonstrated on the raysum image. B. The surgical specimen shows a 3.5-cm ulcerofungating adenocarcinoma (arrowheads) and an 8-mm pedunculated tubular adenoma (arrow) in the sigmoid colon. C. The 3D "virtual dissection" image shows the morphologic distortion of the cancer mass (arrowheads) and the polyp (arrow). D, E. In contrast to the virtual dissection image, image distortion is not noted on the volume-rendered image along the centerline of the colon without flattening (D) and on the 3D endoluminal view (E). Both lesions (arrowheads and arrow) show similar morphologies to those of the surgical specimen.
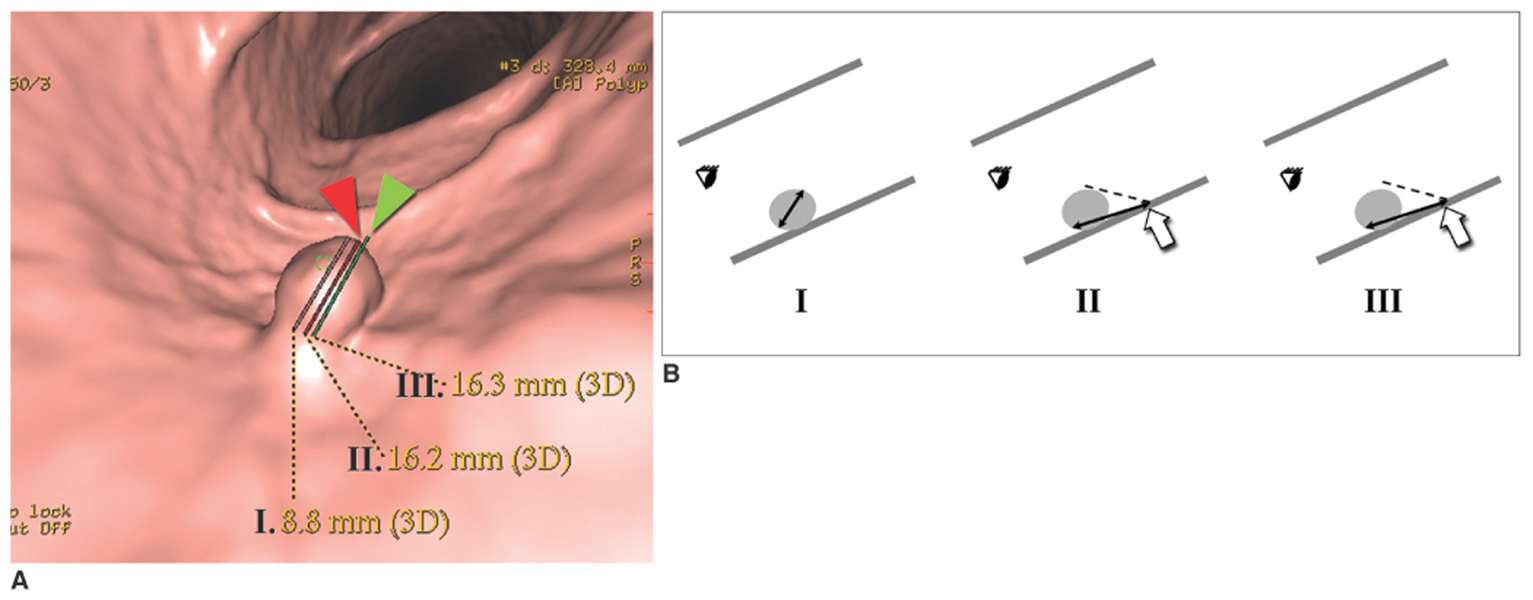
Fig. 7 A 53-year-old male with a tubular adenoma in the sigmoid colon. A. 3D endoluminal view shows three different measurements ("I, II and III") of a sessile polyp with a narrow neck. Which of the three measurements is correct? "I (8.8 mm)" is correct. In "II (16.2 mm)", the measurement cursor (red arrowhead) is placed slightly off the lesion margin and leads to an erroneous measurement. In "III (16.3 mm)", the placement of the measurement cursor (green arrowhead) is clearly incorrect, resulting in an erroneous measurement. B. Correlative measurement diagrams for "I, II and III" of figure A. If the measurement cursor is placed off the lesion boundary (II and III), then the first pixel on the colonic wall beyond the polyp in the viewing direction (arrows) is chosen for measurement (i.e. the measurement cursor cannot be placed in an "empty" luminal space, rather, it is placed on the colonic wall after progressing some distance in the viewing direction until it hits the colonic wall), causing overestimation of lesion size. Even slight misplacement of the cursor (e.g. a single pixel), which may be imperceptible by the naked eye, causes this phenomenon and this can lead to significant overestimation of lesion size as demonstrated in measurement "II".
Reference
-
1. Pickhardt PJ, Choi JR, Hwang I, Butler JA, Puckett ML, Hildebrandt HA, et al. Computed tomographic virtual colonoscopy to screen for colorectal neoplasia in asymptomatic adults. N Engl J Med. 2003. 349:2191–2200.2. Cotton PB, Durkalski VL, Pineau BC, Palesch YY, Mauldin PD, Hoffman B, et al. Computed tomographic colonography (virtual colonoscopy): a multicenter comparison with standard colonoscopy for detection of colorectal neoplasia. JAMA. 2004. 291:1713–1719.3. Rockey DC, Paulson E, Niedzwiecki D, Davis W, Bosworth HB, Sanders L, et al. Analysis of air contrast barium enema, computed tomographic colonography, and colonoscopy: prospective comparison. Lancet. 2005. 365:305–311.4. Mulhall BP, Veerappan GR, Jackson JL. Meta-analysis: computed tomographic colonography. Ann Intern Med. 2005. 142:635–650.5. Ferrucci JT. Colonoscopy: virtual and optical-another look, another view. Radiology. 2005. 235:13–16.6. Fletcher JG, Booya F, Johnson CD, Ahlquist D. CT colonography: unraveling the twists and turns. Curr Opin Gastroenterol. 2005. 21:90–98.7. Yee J. Lefere P, Gryspeerdt S, editors. Patient preparation for CT colonography. Virtual colonoscopy: a practical guide. 2006. 1st ed. Berlin: Springer;23–34.8. Kim SH, Choi BI, Han JK, Lee JM, Eun HW, Lee JY, et al. CT colonography in a Korean population with a high residue diet: comparison between wet and dry preparations. Clin Radiol. 2006. 61:483–494.9. Hsu CW, Imperiale TF. Meta-analysis and cost comparison of polyethylene glycol lavage versus sodium phosphate for colonoscopy preparation. Gastrointest Endosc. 1998. 48:276–282.10. Ginnerup Pedersen B, Moller Christiansen TE, Viborg Mortensen F, Christensen H, Laurberg S. Bowel cleansing methods prior to CT colonography. Acta Radiol. 2002. 43:306–311.11. Ehrenpreis ED, Nogueras JJ, Botoman VA, Bonner GF, Zaitman D, Secrest KM. Serum electrolyte abnormalities secondary to Fleet's Phospho-Soda colonoscopy prep. A review of three cases. Surg Endosc. 1996. 10:1022–1024.12. Vukasin P, Weston LA, Beart RW. Oral Fleet Phospho-Soda laxative-induced hyperphosphatemia and hypocalcemic tetany in an adult: report of a case. Dis Colon Rectum. 1997. 40:497–499.13. Ristvedt SL, McFarland EG, Weinstock LB, Thyssen EP. Patient preferences for CT colonography, conventional colonoscopy, and bowel preparation. Am J Gastroenterol. 2003. 98:578–585.14. Lefere PA, Gryspeerdt SS, Dewyspelaere J, Baekelandt M, Van Holsbeeck BG. Dietary fecal tagging as a cleansing method before CT colonography: initial results polyp detection and patient acceptance. Radiology. 2002. 224:393–403.15. Lefere P, Gryspeerdt S, Marrannes J, Baekelandt M, Van Holsbeeck B. CT colonography after fecal tagging with a reduced cathartic cleansing and a reduced volume of barium. AJR Am J Roentgenol. 2005. 184:1836–1842.16. Lefere P, Gryspeerdt S. Lefere P, Gryspeerdt S, editors. The alternative: fecal tagging. Virtual colonoscopy: a practical guide. 2006. 1st ed. Berlin: Springer;35–50.17. Callstrom MR, Johnson CD, Fletcher JG, Reed JE, Ahlquist DA, Harmsen WS, et al. CT colonography without cathartic preparation: feasibility study. Radiology. 2001. 219:693–698.18. Lefere P, Gryspeerdt S, Baekelandt M, Van Holsbeeck B. Laxative-free CT colonography. AJR Am J Roentgenol. 2004. 183:945–948.19. Iannaccone R, Laghi A, Catalano C, Mangiapane F, Lamazza A, Schillaci A, et al. Computed tomographic colonography without cathartic preparation for the detection of colorectal polyps. Gastroenterology. 2004. 127:1300–1311.20. Seymour CW, Pryor JP, Gupta R, Schwab CW. Anaphylactoid reaction to oral contrast for computed tomography. J Trauma. 2004. 57:1105–1107.21. Miller SH. Anaphylactoid reaction after oral administration of diatrizoate meglumine and diatrizoate sodium solution. AJR Am J Roentgenol. 1997. 168:959–961.22. New Zealand Medicines and Medical Devices Safety Authority. Medicine data sheet. Accessed August 23, 2006. In Medsafe Web site. http://www.medsafe.govt.nz.23. Shinners TJ, Pickhardt PJ, Taylor AJ, Jones DA, Olsen CH. Patient-controlled room air insufflation versus automated carbon dioxide delivery for CT colonography. AJR Am J Roentgenol. 2006. 186:1491–1496.24. Pickhardt PJ. Incidence of colonic perforation at CT colonography: review of existing data and implications for screening of asymptomatic adults. Radiology. 2006. 239:313–316.25. Burling D, Halligan S, Slater A, Noakes MJ, Taylor SA. Potentially serious adverse events at CT colonography in symptomatic patients: national survey of the United Kingdom. Radiology. 2006. 239:464–471.26. Sosna J, Blachar A, Amitai M, Barmeir E, Peled N, Goldberg SN, et al. Colonic perforation at CT colonography: assessment of risk in a multicenter large cohort. Radiology. 2006. 239:457–463.27. Triester SL, Hara AK, Young-Fadok TM, Heigh RI. Colonic perforation after computed tomographic colonography in a patient with fibrostenosing Crohn's disease. Am J Gastroenterol. 2006. 101:189–192.28. Kamar M, Portnoy O, Bar-Dayan A, Amitai M, Munz Y, Ayalon A, et al. Actual colonic perforation in virtual colonoscopy: report of a case. Dis Colon Rectum. 2004. 47:1242–1246.29. Coady-Fariborzian L, Angel LP, Procaccino JA. Perforated colon secondary to virtual colonoscopy: report of a case. Dis Colon Rectum. 2004. 47:1247–1249.30. Young BM, Fletcher JG, Earnest F, Fidler JL, MacCarty RL, Johnson CD, et al. Colonic perforation at CT colonography in a patient without known colonic disease. AJR Am J Roentgenol. 2006. 186:119–121.31. Dachman AH. Advice for optimizing colonic distention and minimizing risk of perforation during CT colonography. Radiology. 2006. 239:317–321.32. Glick SG, Johnson CD, Macari M, Yee J. ACR practice guideline for the performance of computed tomography (CT) colonography in adults. ACR Practice Guidelines and Technical Standards. 2005-2006. 295–299.33. Taylor SA, Halligan S, Goh V, Morley S, Bassett P, Atkin W, et al. Optimizing colonic distention for multi-detector row CT colonography: effect of hyoscine butylbromide and rectal balloon catheter. Radiology. 2003. 229:99–108.34. Morrin MM, Farrell RJ, Keogan MT, Kruskal JB, Yam CS, Raptopoulos V. CT colonography: colonic distention improved by dual positioning but not intravenous glucagon. Eur Radiol. 2002. 12:525–530.35. Yee J, Kumar NN, Hung RK, Akerkar GA, Kumar PR, Wall SD. Comparison of supine and prone scanning separately and in combination at CT colonography. Radiology. 2003. 226:653–661.36. Chen SC, Lu DS, Hecth JR, Kadell BM. CT colonography: value of scanning in both supine and prone position. AJR Am J Roentgenol. 1999. 172:595–599.37. Iannaccone R, Laghi A, Catalano C, Brink JA, Mangiapane F, Trenna S, et al. Detection of colorectal lesions: lower-dose multi-detector row helical CT colonography compared with conventional colonoscopy. Radiology. 2003. 229:775–781.38. Kemerink GJ, Borstlap AC, Frantzen MJ, Schultz FW, Zoetelief J, van Engelshoven JM. Patient and occupational dosimetry in double contrast barium enema examinations. Br J Radiol. 2001. 74:420–428.39. Neri E, Vagli P, Picchietti S, Vannozzi F, Linsalata S, Bardine A, et al. CT colonography: contrast enhancement of benign and malignant colorectal lesions versus fecal residuals. Abdom Imaging. 2005. 30:694–697.40. Oto A, Gelebek V, Oguz BS, Sivri B, Deger A, Akhan O, et al. CT attenuation of colorectal polypoid lesions: evaluation of contrast enhancement in CT colonography. Eur Radiol. 2003. 13:1657–1663.41. Morrin MM, Farrell RJ, Kruskal JB, Reynolds K, McGee JB, Raptopoulos V. Utility of intravenously administered contrast material at CT colonography. Radiology. 2000. 217:765–771.42. Fletcher JG, Johnson CD, Krueger WR, Ahlquist DA, Nelson H, Ilstrup D, et al. Contrast-enhanced CT colonography in recurrent colorectal carcinoma: feasibility of simultaneous evaluation for metastatic disease, local recurrence, and metachronous neoplasia in colorectal carcinoma. AJR Am J Roentgenol. 2002. 178:283–290.43. Laghi A, Iannaccone R, Bria E, Carbone I, Trasatti L, Piacentini F, et al. Contrast-enhanced computed tomographic colonography in the follow-up of colorectal cancer patients: a feasibility study. Eur Radiol. 2003. 13:883–889.44. Horton KM, Eng J, Fishman EK. Normal enhancement of the small bowel: evaluation with spiral CT. J Comput Assist Tomogr. 2000. 24:67–71.45. Yee J, Sun Y. . Performance of contrast-enhanced CT colonography (CTC) (abstr). 2005. Oak Brook, Ill: Radiological Society of North America;185.46. Taylor SA, Halligan S, Slater A, Goh V, Burling DN, Roddie ME, et al. Polyp detection with CT colonography: primary 3D endoluminal analysis versus primary 2D transverse analysis with computer-assisted reader software. Radiology. 2006. 239:759–767.47. Macari M, Milano A, Lavelle M, Berman P, Megibow AJ. Comparison of time-efficient CT colonography with two- and three-dimensional colonic evaluation for detecting colorectal polyps. AJR Am J Roentgenol. 2000. 174:1543–1549.48. Dachman AH, Kuniyoshi JK, Boyle CM, Samara Y, Hoffmann KR, Rubin DT, et al. CT colonography with three-dimensional problem solving for detection of colonic polyps. AJR Am J Roentgenol. 1998. 171:989–995.49. McFarland EG, Brink JA, Pilgram TK, Heiken JP, Balfe DM, Hirselj DA, et al. Spiral CT colonography: reader agreement and diagnostic performance with two- and three-dimensional image-display techniques. Radiology. 2001. 218:375–383.50. Zalis ME, Perumpillichira J, Hahn PF. Digital subtraction bowel cleansing for CT colonography using morphological and linear filtration methods. IEEE Trans Med Imaging. 2004. 23:1335–1343.51. Pickhardt PJ, Choi JH. Electronic cleansing and stool tagging in CT colonography: advantages and pitfalls with primary three-dimensional evaluation. AJR Am J Roentgenol. 2003. 181:799–805.52. Juchems MS, Fleiter TR, Pauls S, Schmidt SA, Brambs HJ, Aschoff AJ. CT colonography: comparison of a colon dissection display versus 3D endoluminal view for the detection of polyps. Eur Radiol. 2006. 16:68–72.53. Johnson KT, Johnson CD, Fletcher JG, MacCarty RL, Summers RL. CT colonography using 360-degree virtual dissection: a feasibility study. AJR Am J Roentgenol. 2006. 186:90–95.54. Hoppe H, Quattropani C, Spreng A, Mattich J, Netzer P, Dinkel HP. Virtual colon dissection with CT colonography compared with axial interpretation and conventional colonoscopy: preliminary results. AJR Am J Roentgenol. 2004. 182:1151–1158.55. Fletcher JG, Johnson CD, MacCarty R, Harmsen WS, Mandrekar JN, Hara AK. . Primary 2D versus primary 3D endoluminal virtual dissection interpretation at CT colonography (CTC): results in 452 asymptomatic patients (abstr). 2006. Oak Brook, IL: Radiological Society of North America;358.56. Summers RM, Beaulieu CF, Pusanik LM, Malley JD, Jeffrey RB Jr, Glazer DI, et al. Automated polyp detector for CT colonography: feasibility study. Radiology. 2000. 216:284–290.57. Yoshida H, Masutani Y, MacEneaney P, Rubin DT, Dachman AH. Computerized detection of colonic polyps at CT colonography on the basis of volumetric features: pilot study. Radiology. 2002. 222:327–336.58. Mani A, Napel S, Paik DS, Jeffrey RB Jr, Yee J, Olcott EW, et al. Computed tomography colonography: feasibility of computer-aided polyp detection in a "first reader" paradigm. J Comput Assist Tomogr. 2004. 28:318–326.59. Bogoni L, Cathier P, Dundar M, Jerebko A, Lakare S, Liang J, et al. Computer-aided detection (CAD) for CT colonography: a tool to address a growing need. Br J Radiol. 2005. 78:S57–S62.60. Halligan S, Altman DG, Mallett S, Taylor SA, Burling D, Roddie M, et al. Computed tomographic colonography: assessment of radiologist performance with and without computer-aided detection. Gastroenterology. 2006. 131:1690–1699.61. Summers RM, Yao J, Pickhardt PJ, Franaszek M, Bitter I, Brickman D, et al. Computed tomographic virtual colonoscopy computer-aided polyp detection in a screening population. Gastroenterology. 2005. 129:1832–1844.62. Zalis ME, Barish MA, Choi JR, Dachman AH, Fenlon HM, Ferrucci JT, et al. Working Group on Virtual Colonoscopy. CT colonography reporting and data system: a consensus proposal. Radiology. 2005. 236:3–9.63. Pickhardt PJ, Lee AD, McFarland EG, Taylor AJ. Linear polyp measurement at CT colonography: in vitro and in vivo comparison of two-dimensional and three-dimensional displays. Radiology. 2005. 236:872–878.64. Cancer statistics. Accessed July 18, 2006. National Cancer Center Web site;http://www.ncc.re.kr.65. Fisichella V, Hellstrom M. Availability, indications, and technical performance of computed tomographic colonography: a national survey. Acta Radiol. 2006. 47:231–237.66. Burling D, Halligan S, Altman DG, Atkin W, Bartram C, Fenlon H, et al. Polyp measurement and size categorization by CT colonography: effect of observer experience in a multicentre setting. Eur Radiol. 2006. 16:1737–1744.67. Soto JA, Barish MA, Yee J. Reader training in CT colonography: how much is enough? Radiology. 2005. 237:26–27.68. Park SH, Ha HK, Kim MJ, Kim KW, Kim AY, Yang DH, et al. False-negative results at multi-detector row CT colonography: multivariate analysis of causes for missed lesions. Radiology. 2005. 235:495–502.69. Kim YK, Lee JE, Lee JK, Baek SY, Song HJ, Jung SA. Efficacy of CT colonography in the detection of colorectal polypoid lesions. J Korean Radiol Soc. 2005. 52:15–22.70. Chung DJ, Huh KC, Choi WJ, Kim JK. CT colonography using 16-MDCT in the evaluation of colorectal cancer. AJR Am J Roentgenol. 2005. 184:98–103.71. ACRIN protocol 6664. Accessed July 18, 2006. American College of Radiology Imaging Network Web site; http://www.acrin.org/6664_protocol.html.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Virtual CT Colonoscopy and Virtual CT Barium Enema using Multidetector-row CT
- Efficacy of CT Colonography in the Detection of Colorectal Polypoid Lesions
- Diagnostic Performance of CT Colonography for the Detection of Colorectal Polyps
- Comparison of Colonoscopy and Virtual Colonoscopy for the Detection of Colorectal Polyps
- Clinical Significance of Preoperative Virtual Colonoscopy for Evaluation of the Proximal Colon in Patient With Obstructive Colorectal Cancer
