Arthroscopic Repair of Combined Bankart and SLAP Lesions: Operative Techniques and Clinical Results
- Affiliations
-
- 1Department of Orthopaedic Surgery, Good Samsun Hospital, Busan, Korea.
- 2Department of Orthopaedic Surgery, Pusan National University College of Medicine, Busan, Korea. kuentak@pusan.ac.kr
- KMID: 1110348
- DOI: http://doi.org/10.4055/cios.2010.2.1.39
Abstract
-
BACKGROUND: To evaluate the clinical results and operation technique of arthroscopic repair of combined Bankart and superior labrum anterior to posterior (SLAP) lesions, all of which had an anterior-inferior Bankart lesion that continued superiorly to include separation of the biceps anchor in the patients presenting recurrent shoulder dislocations.
METHODS
From May 2003 to January 2006, we reviewed 15 cases with combined Bankart and SLAP lesions among 62 patients with recurrent shoulder dislocations who underwent arthroscopic repair. The average age at surgery was 24.2 years (range, 16 to 38 years), with an average follow-up period of 15 months (range, 13 to 28 months). During the operation, we repaired the unstable SLAP lesion first with absorbable suture anchors and then also repaired Bankart lesion from the inferior to superior fashion. We analyzed the preoperative and postoperative results by visual analogue scale (VAS) for pain, the range of motion, American Shoulder and Elbow Surgeon (ASES) and Rowe shoulder scoring systems. We compared the results with the isolated Bankart lesion.
RESULTS
VAS for pain was decreased from preoperative 4.9 to postoperative 1.9. Mean ASES and Rowe shoulder scores were improved from preoperative 56.4 and 33.7 to postoperative 91.8 and 94.1, respectively. There were no specific complication and no significant limitation of motion more than 10 degree at final follow-up. We found the range of motions after the arthroscopic repair in combined lesions were gained more slowly than in patients with isolated Bankart lesions.
CONCLUSIONS
In recurrent dislocation of the shoulder with combined Bankart and SLAP lesion, arthroscopic repair using absorbable suture anchors produced favorable clinical results. Although it has technical difficulty, the concomitant unstable SLAP lesion should be repaired in a manner that stabilizes the glenohumeral joint, as the Bankart lesion can be repaired if the unstable SLAP lesion is repaired first.
MeSH Terms
-
Adolescent
Adult
Arthroscopy/*methods
Humans
Magnetic Resonance Imaging
Male
Orthopedic Procedures/*methods
Pain Measurement
Postoperative Care
Range of Motion, Articular
Shoulder Dislocation/diagnosis/etiology/physiopathology/*surgery
Tendon Injuries/complications/diagnosis/physiopathology/*surgery
Treatment Outcome
Young Adult
Figure
-

Fig. 1 MRI findings showing the Bankart lesion (A) and the superior labrum anterior to posterior lesion (B).

Fig. 2 Arthroscopic portals were designed at the right shoulder. Arrow is the anterosuperior portal and arrow head is the port of Wilmington.
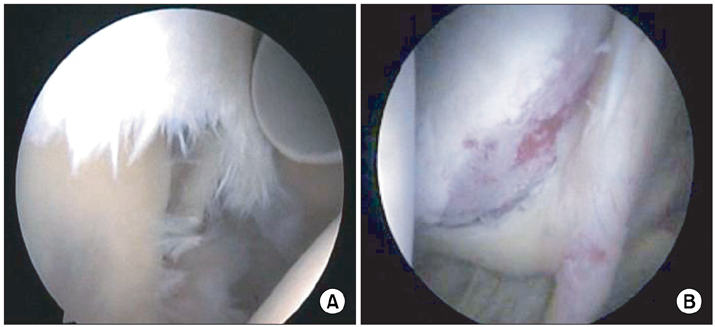
Fig. 3 Arthroscopic image of the combined Bankart and superior labrum anterior to posterior lesion showing (A) inferiorly displaced superior labrum with significant fraying (right shoulder, from posterior viewing portal) and (B) medially displaced superior and anteroinferior labral complex (right shoulder, from anterior working portal).

Fig. 4 The effect of the superior labrum anterior to posterior (SLAP) repair revealing (A) medially an inferiorly displaced anteroinferior labrum before the repair of the SLAP lesion (right shoulder, from posterior viewing portal) and (B) relatively anatomically reduced Bankart lesion after the repair of the SLAP lesion (right shoulder, from posterior viewing portal).

Fig. 5 Final arthroscopic findings after the completion of the repair of combined Bankart and superior labrum anterior to posterior lesion in right shoulder viewing from (A) posterior viewing portal and (B) anterior working portal.
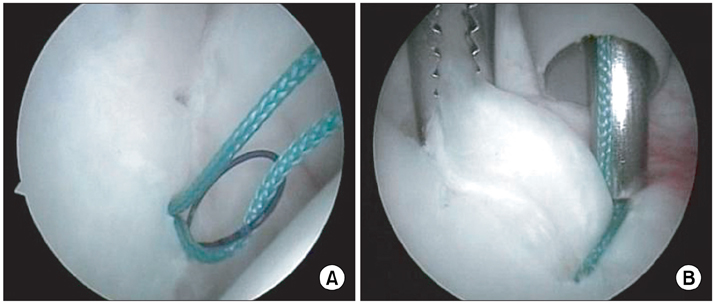
Fig. 6 Suture relay and knot tying representing (A) intra-articular suture relay using 2-0 Nylon loop which shuttles capsular side of suture limbs and (B) sliding knot tying of the most inferior suture anchor around 5 o'clock while exerting upward tension of the anteroinferior labrum using tissue grasper (right shoulder, from posterior viewing portal).
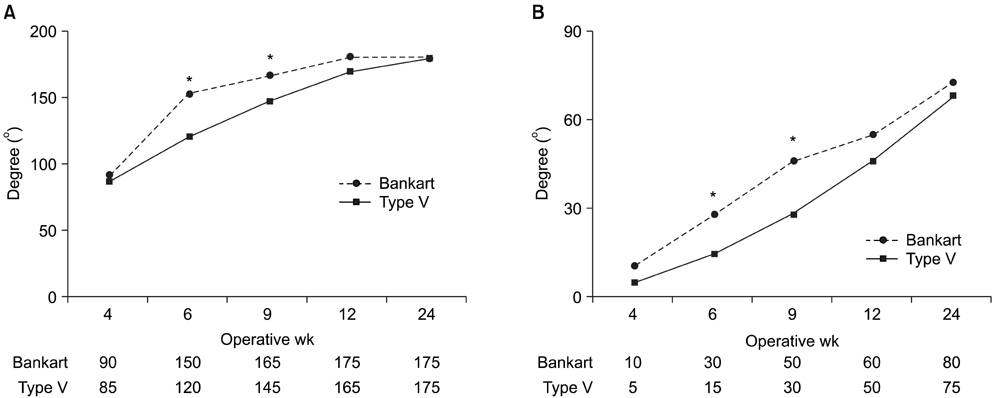
Fig. 7 In type superior labrum anterior to posterior Lesion, the range of motions in (A) forward flexion and (B) external rotation at 90 degree abduction after the arthroscopic repair were gained more slowly than in patients with isolated Bankart lesion (*p < 0.05).
Cited by 3 articles
-
Superior Labrum Anterior to Posterior (SLAP) Lesion with Glenohumeral Instability
Chul Hong Kim, Li Wang
J Korean Orthop Assoc. 2017;52(5):378-384. doi: 10.4055/jkoa.2017.52.5.378.Is Anatomical Healing Essential for Better Clinical Outcome in Type II SLAP Repair? Clinico-Radiological Outcome after Type II SLAP Repair
Piyush Suresh Nashikkar, Sung-Min Rhee, Chintan Vinod Desai, Joo Han Oh
Clin Orthop Surg. 2018;10(3):358-367. doi: 10.4055/cios.2018.10.3.358.Anterior Shoulder Instability with Concomitant Superior Labrum from Anterior to Posterior (SLAP) Lesion Compared to Anterior Instability without SLAP Lesion
Claire Marie C. Durban, Je Kyun Kim, Sae Hoon Kim, Joo Han Oh
Clin Orthop Surg. 2016;8(2):168-174. doi: 10.4055/cios.2016.8.2.168.
Reference
-
1. Snyder SJ, Karzel RP, Del Pizzo W, Ferkel RD, Friedman MJ. SLAP lesions of the shoulder. Arthroscopy. 1990. 6(4):274–279.
Article2. Maffet MW, Gartsman GM, Moseley B. Superior labrumbiceps tendon complex lesions of the shoulder. Am J Sports Med. 1995. 23(1):93–98.
Article3. Richards RR, An KN, Bigliani LU, et al. A standardized method for the assessment of shoulder function. J Shoulder and Elbow Surg. 1994. 3(6):347–352.
Article4. Rowe CR, Zarins B. Recurrent transient subluxation of the shoulder. J Bone Joint Surg Am. 1981. 63(6):863–872.
Article5. Andrews JR, Carson WG Jr, McLeod WD. Glenoid labrum tears related to the long head of the biceps. Am J Sports Med. 1985. 13(5):337–341.
Article6. Snyder SJ, Banas MP, Karzel RP. An analysis of 140 injuries to the superior glenoid labrum. J Shoulder Elbow Surg. 1995. 4(4):243–248.
Article7. Kim KT, Kim CH, Kim SH. Arthroscopic Bankart repair with suture anchor. J Korean Orthop Sports Med. 2002. 1(2):149–153.8. Rhee YG, Kim YK, Chun YS. Arthroscopic fixation for unstable SLAP lesion using biodegradable tack. J Korean Orthop Assoc. 1998. 33(3):508–514.9. Soslowsky LJ, Malicky DM, Blasier RB. Active and passive factors in inferior glenohumeral stabilization: a biomechanical model. J Shoulder Elbow Surg. 1997. 6(4):371–379.
Article10. Lo IK, Burkhart SS. Triple labral lesions: pathology and surgical repair technique-report of seven cases. Arthroscopy. 2005. 21(2):186–193.
Article11. Nam EK, Snyder SJ. The diagnosis and treatment of superior labrum, anterior and posterior (SLAP) lesions. Am J Sports Med. 2003. 31(5):798–810.
Article12. Depuy J, Steiner ME. Isolated shoulder labral tears: treatment and correlation with labral anatomy. Orthop Trans. 1990. 14(2):244.13. Resch H, Golser K, Thoeni H, Sperner G. Arthroscopic repair of superior glenoid labral detachment (the SLAP lesion). J Shoulder Elbow Surg. 1993. 2(3):147–155.
Article14. Ogilvie-Harris DJ, Wiley AM. Arthroscopic surgery of the shoulder: a general appraisal. J Bone Joint Surg Br. 1986. 68(2):201–207.
Article15. Pappas AM, Goss TP, Kleinman PK. Symptomatic shoulder instability due to lesions of the glenoid labrum. Am J Sports Med. 1983. 11(5):279–288.
Article16. Rodosky MW, Harner CD, Fu FH. The role of the long head of the biceps muscle and superior glenoid labrum in anterior stability of the shoulder. Am J Sports Med. 1994. 22(1):121–130.
Article17. Itoi E, Kuechle DK, Newman SR, Morrey BF, An KN. Stabilising function of the biceps in stable and unstable shoulders. J Bone Joint Surg Br. 1993. 75(4):546–550.
Article18. Warner JJ, Kann S, Marks P. Arthroscopic repair of combined Bankart and superior labral detachment anterior and posterior lesions: technique and preliminary results. Arthroscopy. 1994. 10(4):383–391.
Article19. Freehill MQ, Harms DJ, Huber SM, Atlihan D, Buss DD. Poly-L-lactic acid tack synovitis after arthroscopic stabilization of the shoulder. Am J Sports Med. 2003. 31(5):643–647.
Article20. Wilkerson JP, Zvijac JE, Uribe JW, Schurhoff MR, Green JB. Failure of polymerized lactic acid tacks in shoulder surgery. J Shoulder Elbow Surg. 2003. 12(2):117–121.
Article21. Oh JH, Kim SH, Lee HK, Jo KH, Bae KJ. Trans-rotator cuff portal is safe for arthroscopic superior labral anterior and posterior lesion repair: clinical and radiological analysis of 58 SLAP lesions. Am J Sports Med. 2008. 36(10):1913–1921.
Article22. Cohen DB, Coleman S, Drakos MC, et al. Outcomes of isolated type II SLAP lesions treated with arthroscopic fixation using a bioabsorbable tack. Arthroscopy. 2006. 22(2):136–142.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Arthroscopic Treatment of a Type II Superior Labrum Anterior to Posterior (SLAP) Lesion Combined with a Bankart Lesion: Comparative Study between Debridement and Repair of Type II SLAP Lesion by the Status of Lesion
- Is Anatomical Healing Essential for Better Clinical Outcome in Type II SLAP Repair? Clinico-Radiological Outcome after Type II SLAP Repair
- Results According to Arthroscopic Repair Methods of Bankart Lesion (Operative Methods According to Labral Tear)
- New V-shaped Technique in SLAP Repair (Comparison of Cinical Results Between New V-shaped Repair and Conventional Rapair Technique in Arthroscopic Type II SLAP Surgery)
- Superior Labrum Anterior to Posterior (SLAP) Lesion with Glenohumeral Instability
