Yonsei Med J.
2011 Sep;52(5):779-786. 10.3349/ymj.2011.52.5.779.
Prognostic Implications of the NIH Consensus Criteria in Children with Chronic Graft-versus-Host Disease
- Affiliations
-
- 1Department of Pediatrics, The Catholic University of Korea, College of Medicine, Seoul, Korea. cngped@cmcnu.or.kr
- 2Department of Pediatrics, Hallym University, College of Medicine, Seoul, Korea.
- 3Department of Biostatistics, The Catholic University of Korea, College of Medicine, Seoul, Korea.
- KMID: 1108071
- DOI: http://doi.org/10.3349/ymj.2011.52.5.779
Abstract
- PURPOSE
In this study, we analyzed a cohort of children with chronic graft-versus-host disease (GvHD) according to the NIH consensus classification (NCC) in order to observe whether global assessment at diagnosis correlates with GvHD-specific endpoints. We then studied the clinical course of these patients, specifically with regards to episodes of GvHD exacerbation requiring treatment escalation.
MATERIALS AND METHODS
Recipients of either allogeneic bone marrow transplantation (BMT) or peripheral blood stem cell transplantation (PBSCT) from January 2006 to August 2008 at the Department of Pediatrics, The Catholic University of Korea were evaluated for chronic GvHD, which was diagnosed according to the NCC. The course of chronic GvHD in these patients was then followed.
RESULTS
Of 59 evaluable patients, 23 developed chronic GvHD for a cumulative incidence of 39.3%. Upon multivariate analysis, previous acute GvHD (> or =grade II) had a significant impact on chronic GvHD incidence. With a median duration of systemic treatment for chronic GvHD of 501 days, no significant relationship was found between initial global severity of chronic GvHD and either duration of immunosuppressive treatment or final clinical response to treatment. Fifteen patients (65%) experienced at least one episode of chronic GvHD exacerbation during the period of follow-up, with a median of four exacerbations in the subgroup of patients who experienced such events. Lung GvHD resulted in the highest number of exacerbations per diagnosed patient, followed by oral GvHD.
CONCLUSION
Analysis of this small cohort indicates that global assessment as proposed by the NCC may have limited correlations with GvHD-specific endpoints, possibly due to the favorable response of children to treatment.
Keyword
MeSH Terms
-
Adolescent
Bone Marrow Transplantation/adverse effects
Child
Child, Preschool
Chronic Disease
Cohort Studies
Consensus Development Conferences, NIH as Topic
Female
Graft vs Host Disease/classification/*diagnosis/drug therapy/etiology
Humans
Immunosuppressive Agents/administration & dosage
Infant
Male
National Institutes of Health (U.S.)
Peripheral Blood Stem Cell Transplantation/adverse effects
Prognosis
Republic of Korea
Risk Factors
United States
Figure
-
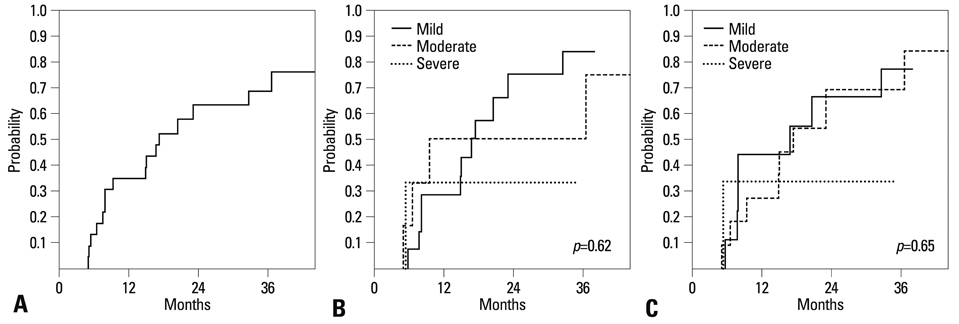
Fig. 1 (A) Probability of withdrawal of systemic IST. (B) Probability of withdrawal of systemic IST according to initial global severity of chronic GvHD. (C)Probability of withdrawal of systemic IST according to initial global severity of chronic GvHD (with inclusion of hepatic GvHD). GvHD, graft-versus-host disease.
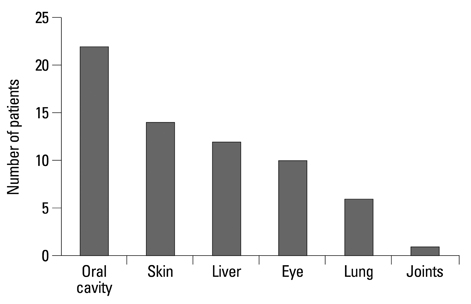
Fig. 2 Chronic GvHD organ involvement throughout the follow-up period. GvHD, graft-versus-host disease.
Cited by 1 articles
-
Lung Transplantation for Bronchiolitis Obliterans after Allogeneic Hematopoietic Stem Cell Transplantation
Yu Ri Kim, Seok Jin Haam, Yoon Ghil Park, Beom Jin Lim, Yoo Mi Park, Hyo Chae Paik
Yonsei Med J. 2012;53(5):1054-1057. doi: 10.3349/ymj.2012.53.5.1054.
Reference
-
1. Shulman HM, Sullivan KM, Weiden PL, McDonald GB, Striker GE, Sale GE, et al. Chronic graft-versus-host syndrome in man. A long-term clinicopathologic study of 20 Seattle patients. Am J Med. 1980. 69:204–217.2. Lee SJ, Vogelsang G, Flowers ME. Chronic graft-versus-host disease. Biol Blood Marrow Transplant. 2003. 9:215–233.
Article3. Filipovich AH, Weisdorf D, Pavletic S, Socie G, Wingard JR, Lee SJ, et al. National Institutes of Health consensus development project on criteria for clinical trials in chronic graft-versus-host disease: I. Diagnosis and staging working group report. Biol Blood Marrow Transplant. 2005. 11:945–956.
Article4. Jagasia M, Giglia J, Chinratanalab W, Dixon S, Chen H, Frangoul H, et al. Incidence and outcome of chronic graft-versus-host disease using National Institutes of Health consensus criteria. Biol Blood Marrow Transplant. 2007. 13:1207–1215.
Article5. Cho BS, Min CK, Eom KS, Kim YJ, Kim HJ, Lee S, et al. Feasibility of NIH consensus criteria for chronic graft-versus-host disease. Leukemia. 2009. 23:78–84.
Article6. Vigorito AC, Campregher PV, Storer BE, Carpenter PA, Moravec CK, Kiem HP, et al. Evaluation of NIH consensus criteria for classification of late acute and chronic GVHD. Blood. 2009. 114:702–708.
Article7. Przepiorka D, Weisdorf D, Martin P, Klingemann HG, Beatty P, Hows J, et al. 1994 Consensus Conference on Acute GVHD Grading. Bone Marrow Transplant. 1995. 15:825–828.8. Yoshihara S, Yanik G, Cooke KR, Mineishi S. Bronchiolitis obliterans syndrome (BOS), bronchiolitis obliterans organizing pneumonia (BOOP), and other late-onset noninfectious pulmonary complications following allogeneic hematopoietic stem cell transplantation. Biol Blood Marrow Transplant. 2007. 13:749–759.
Article9. Akpek G, Chinratanalab W, Lee LA, Torbenson M, Hallick JP, Anders V, et al. Gastrointestinal involvement in chronic graft-versus-host disease: a clinicopathologic study. Biol Blood Marrow Transplant. 2003. 9:46–51.
Article10. Tomas JF, Pinilla I, Garcia-Buey ML, Garcia A, Figuera A, Gomez-Garcia de Soria VGG, et al. Long-term liver dysfunction after allogeneic bone marrow transplantation: clinical features and course in 61 patients. Bone Marrow Transplant. 2000. 26:649–655.
Article11. Kim DH, Sohn SK, Baek JH, Lee KH, Lee JH, Choi SJ, et al. Time to first flare-up episode of GVHD can stratify patients according to their prognosis during clinical course of progressive- or quiescent-type chronic GVHD. Bone Marrow Transplant. 2007. 40:779–784.
Article12. Flowers ME, Storer B, Carpenter P, Rezvani AR, Vigorito AC, Campregher PV, et al. Treatment change as a predictor of outcome among patients with classic chronic graft-versus-host disease. Biol Blood Marrow Transplant. 2008. 14:1380–1384.
Article13. Zecca M, Prete A, Rondelli R, Lanino E, Balduzzi A, Messina C, et al. Chronic graft-versus-host disease in children: incidence, risk factors, and impact on outcome. Blood. 2002. 100:1192–1200.
Article14. Kondo M, Kojima S, Horibe K, Kato K, Matsuyama T. Risk factors for chronic graft-versus-host disease after allogeneic stem cell transplantation in children. Bone Marrow Transplant. 2001. 27:727–730.
Article15. Lee JH, Lee JH, Choi SJ, Kim S, Seol M, Lee YS, et al. Graft-versus-host disease (GVHD)-specific survival and duration of systemic immunosuppressive treatment in patients who developed chronic GVHD following allogeneic haematopoietic cell transplantation. Br J Haematol. 2003. 122:637–644.
Article16. Stewart BL, Storer B, Storek J, Deeg HJ, Storb R, Hansen JA, et al. Duration of immunosuppressive treatment for chronic graft-versus-host disease. Blood. 2004. 104:3501–3506.
Article17. Treister NS, Woo SB, O'Holleran EW, Lehmann LE, Parsons SK, Guinan EC. Oral chronic graft-versus-host disease in pediatric patients after hematopoietic stem cell transplantation. Biol Blood Marrow Transplant. 2005. 11:721–731.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Acute Cutaneous Graft-Versus-Host Reaction
- Chronic Graft Versus Host Disease
- Overlap Syndrome with Features of Actue and Chronic Cutaneous Graft-versus-host Disease
- Rehabilitation in Children With Sclerodermoid Chronic Graft-Versus-Host Disease: Case Series
- Acute Graft-versus-Host Disease after Liver Transplantation
