18F-Fluorodeoxyglucose PET/CT in a Patient with Esophageal and Genital Leiomyomatosis
- Affiliations
-
- 1Department of Nuclear Medicine, School of Medicine, Kyung Hee University, Seoul 130-702, Korea. petct@paran.com
- KMID: 1102567
- DOI: http://doi.org/10.3348/kjr.2009.10.6.632
Abstract
- Diffuse esophageal leiomyomatosis is a rare benign tumor, which can be associated with leiomyoma in female genital tracts involving the uterus, vagina, and vulva. Alport syndrome, an inherited disorder that includes the kidneys, eyes, and sensorineural hearing loss, is also rarely associated with these multiple leiomyomatosis. In our case, 18F-fluoroseoxyglucose positron emission tomography/computed tomography was used to distinguish esophageal and genital leiomyomatosis from malignant masses.
Keyword
MeSH Terms
-
Diagnosis, Differential
Esophageal Neoplasms/*radiography/*radionuclide imaging
Female
Fluorodeoxyglucose F18/diagnostic use
Genital Neoplasms, Female/*radiography/*radionuclide imaging
Humans
Leiomyomatosis/*radiography/*radionuclide imaging
Middle Aged
Positron-Emission Tomography/*methods
Radiographic Image Interpretation, Computer-Assisted
Radiopharmaceuticals/diagnostic use
Tomography, X-Ray Computed/*methods
Figure
-
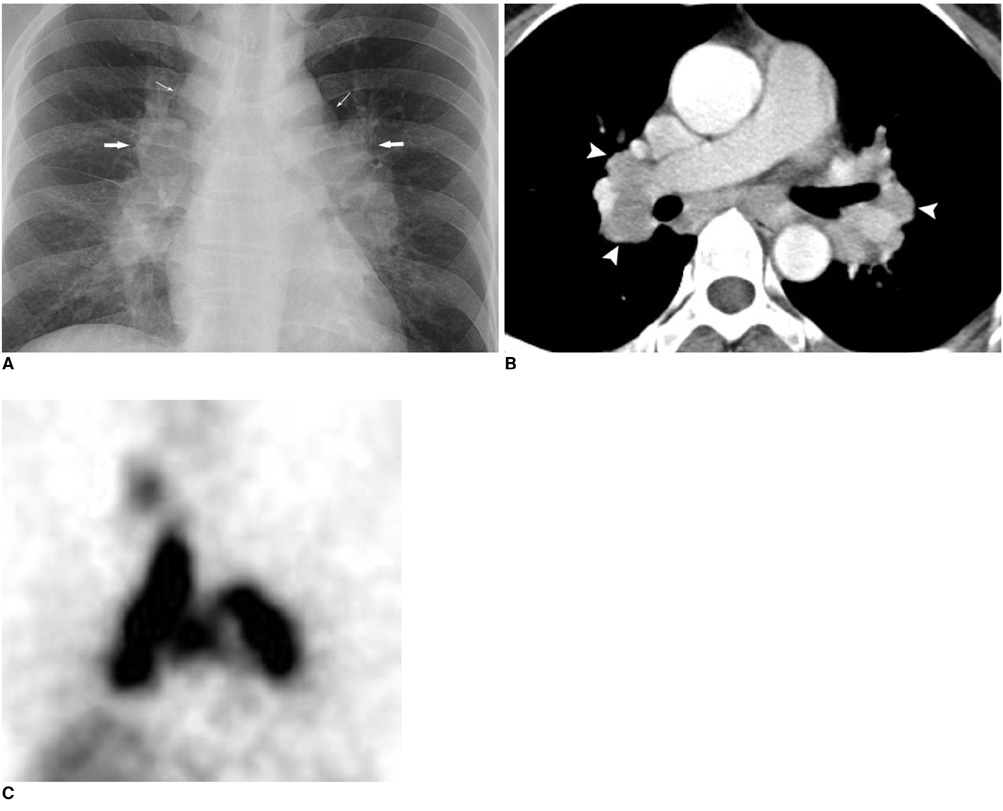
Fig. 1 Esophageal and genital leiomyomatosis A. Huge abnormal increased 18F-FDG uptake lesion (arrows) in esophagus (maximal SUV: 3.8) noted on PET/CT image (upper row). Corresponding contrast enhanced CT images demonstrate abnormal mass lesions in each organ. B. Hypermetabolic lesions (arrows) were evident in pelvic region including uterus (maximal SUV: 6.13) (middle row). C. Hypermetabolic lesions (arrows) were evident in vulvar region (maximal SUV: 2.81) (lower row). D. Arrows point to lesions evident in on PET. E-J. Pathologic examination. Grossly, 13 cm (length)×8 cm (width)×6 cm (depth) poorly circumscribed, sausage-like, white/pink, firm muscular mass oriented across distal esophagus and gastric cardia was evident. Diffusely thickened esophageal wall measured 2 cm in maximal thickness (E). Histologically, Hematoxylin & Eosin staining (×40 in panel F, ×200 in panel G) reveals characteristics of leiomyoma. Multiple confluent well-differentiated smooth muscle proliferations were evident. Cells formed fascicles and interlacing bundles without cytologic atypia. Immunostaining for smooth-muscle actin (×40) was strongly positive in smooth-muscle origin tumor cells with control reaction of microvillous projections in apical cell membrane (H). Uterus lesion also demonstrates as leiomyoma pattern in Hematoxylin & Eosin staining (×100 in panel I, ×400 in panel J).
Reference
-
1. Compagnoni GM, Talamonti MS, Joob A, Ergun GA, Rao S. Esophageal leiomyomatosis in a woman with a history of vulvar leiomyoma and Barrett's esophagus: a case report and review of the literature. Dig Surg. 2000. 17:306–309.2. Kugelman A, Greif Y, Gershoni-Baruch R, Berkowitz D, Best LA, Guralnik L, et al. Pulmonary presentation of esophageal leiomyomatosis associated with Alport syndrome in childhood. Isr Med Assoc J. 2003. 5:293–294.3. Pujol J, Parés D, Mora L, Sans M, Jaurrieta E. Diagnosis and management of diffuse leiomyomatosis of the oesophagus. Dis Esophagus. 2000. 13:169–171.4. Rabushka LS, Fishman EK, Kuhlman JE, Hruban RH. Diffuse esophageal leiomyomatosis in a patient with Alport syndrome: CT demonstration. Radiology. 1991. 179:176–178.5. Garcia-Torres R, Cruz D, Orozco L, Heidet L, Gubler MC. Alport syndrome and diffuse leiomyomatosis. Clinical aspects, pathology, molecular biology and extracellular matrix studies. A synthesis. Nephrologie. 2000. 21:9–12.6. Kilian AK, Ringle T, Waag KL, Düber C, Neff KW. Pre- and postoperative MRI of esophageal and gastric leiomyomatosis in a pediatric patient. AJR Am J Roentgenol. 2005. 184:S129–S131.7. Dahan K, Heidet L, Zhou J, Mettler G, Leppig KA, Proesmans W, et al. Smooth muscle tumors associated with X-linked Alport syndrome: carrier detection in females. Kidney Int. 1995. 48:1900–1906.8. Meirelles GS, Ravizzini G, Yeung HW, Akhurst T. Esophageal leiomyoma: a rare cause of false-positive FDG scans. Clin Nucl Med. 2006. 31:342–344.9. Memisoglu E, Agarwal B, Akduman I, Prather C, Collins B, Civelek AC. Multimodality diagnostic imaging of diffuse esophageal leiomyomatosis. J Comput Assist Tomogr. 2006. 30:100–104.10. Ak I, Ozalp S, Yalçin OT, Zor E, Vardareli E. Uptake of 2-[18F]fluoro-2-deoxy-D-glucose in uterine leiomyoma: imaging of four patients by coincidence positron emission tomography. Nucl Med Commun. 2004. 25:941–945.11. Lee SM, Bae SK. Esophageal Leiomyoma with intense FDG uptake on 18F-FDG PET/CT. Nucl Med Mol Imaging. 2008. 42:410–413.12. Nishizawa S, Inubushi M, Kido A, Miyagawa M, Inoue T, Shinohara K, et al. Incidence and characteristics of uterine leiomyomas with FDG uptake. Ann Nucl Med. 2008. 22:803–810.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Esophageal Leiomyoma with intense FDG uptake on 18F-FDG PET/CT
- A Comparison Study of Esophageal Findings on 18F-FDG PET/CT and Esophagogastroduodenoscopy
- Use of 18F-FDG PET/CT in Second Primary Cancer
- Nodular Fasciitis Mimicking Malignant Tumor on 18F-FDG PET/CT
- Supraclavicular Lymph Node Metastasis from Various Malignancies: Assessment with 18F-Fluorodeoxyglucose Positron Emission Tomography/CT, Contrast-Enhanced CT and Ultrasound
