Typical and Atypical Manifestations of Intrathoracic Sarcoidosis
- Affiliations
-
- 1Department of Radiology, St. Vincent's Hospital, The Catholic University of Korea, Kyunggi-do 442-723, Korea.
- 2Department of Radiology, Incheon St. Mary's Hospital, The Catholic University of Korea, Incheon 403-720, Korea. kjrad@catholic.ac.kr
- 3Department of Pathology, Seoul St. Mary's Hospital, The Catholic University of Korea, Seoul 137-107, Korea.
- KMID: 1102566
- DOI: http://doi.org/10.3348/kjr.2009.10.6.623
Abstract
- Sarcoidosis is a systemic disorder of unknown cause that is characterized by the presence of noncaseating granulomas. The radiological findings associated with sarcoidosis have been well described. The findings include symmetric, bilateral hilar and paratracheal lymphadenopathy, with or without concomitant parenchymal abnormalities (multiple small nodules in a peribronchovascular distribution along with irregular thickening of the interstitium). However, in 25% to 30% of cases, the radiological findings are atypical and unfamiliar to most radiologists, which cause difficulty for making a correct diagnosis. Many atypical forms of intrathoracic sarcoidosis have been described sporadically. We have collected cases with unusual radiological findings associated with pulmonary sarcoidosis (unilateral or asymmetric lymphadenopathy, necrosis or cavitation, large opacity, ground glass opacity, an airway abnormality and pleural involvement) and describe the typical forms of the disorder as well. The understanding of a wide range of the radiological manifestations of sarcoidosis will be very helpful for making a proper diagnosis.
Keyword
MeSH Terms
Figure
-
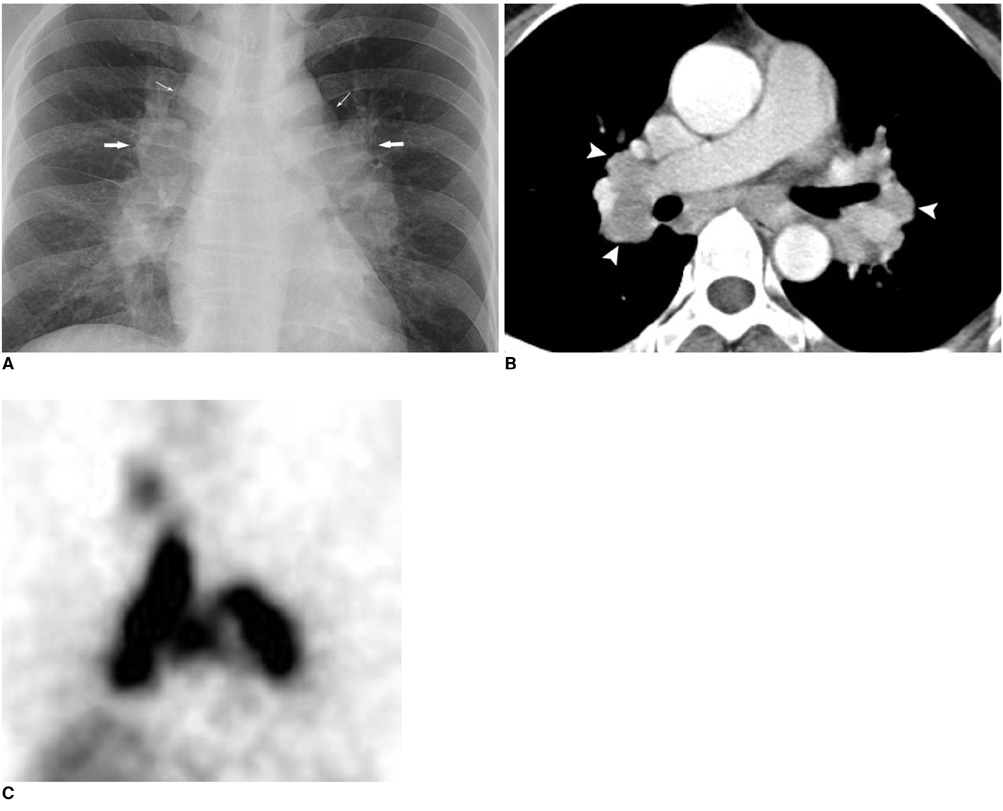
Fig. 1 Imaging findings for bilateral, symmetrical hilar lymphadenopathy in 35-year-old man with sarcoidosis are shown. A. Chest PA shows bilateral symmetric hilar enlargement (arrows) and right lower paratracheal and subaortic lymphadenopathy (thin arrows). B. Axial CT scan shows bilateral hilar and subcarinal lymphadenopathy (arrowheads). C. Gallium scan reveals 'lambda sign' with bilateral hilar and mediastinal lymphadenopathy.

Fig. 2 Node calcification in sarcoidosis is shown. Axial CT scan shows typical eggshell calcification in both hilar and peribronchial nodes (arrows). Presence of node calcification suggests chronic condition.
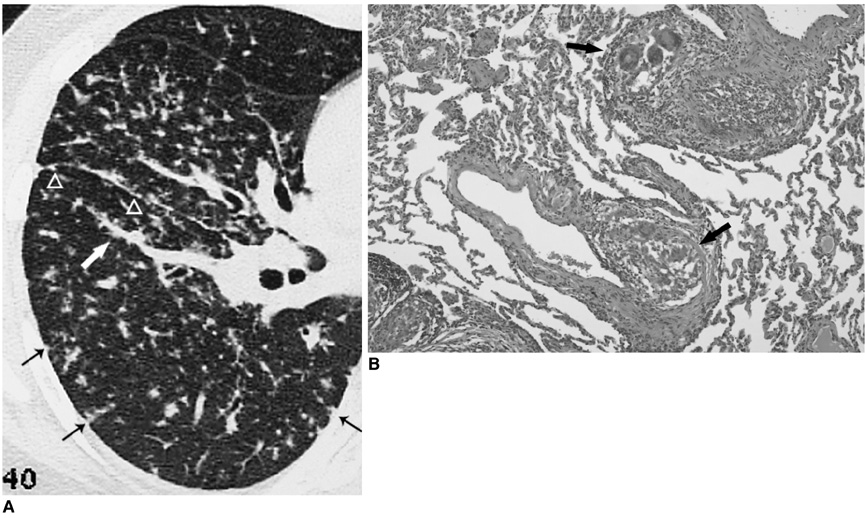
Fig. 3 Imaging findings for sarcoid granulomas with perilymphatic distribution are shown. A. High-resolution CT scan shows multiple small nodules in peribronchovascular interstitium (arrow), interlobar fissure (arrowheads) and subpleural region (thin arrows). B. Microscopic image (Hematoxylin & Eosin staining, ×40) reveals non-caseating granulomas with giant cells and proliferating epithelioid cells in bronchovascular interstitium (arrows).

Fig. 4 Imaging findings for interstitial thickening in sarcoidosis are presented. High-resolution CT image shows nodular thickening of interlobular septae, peribronchovascular interstitium and interlobar fissure (arrows).
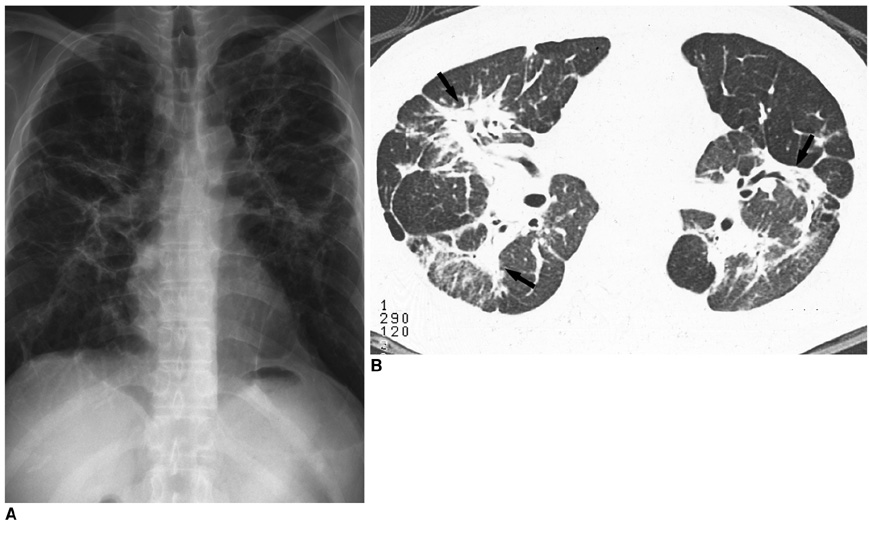
Fig. 5 Imaging findings for fibrosis in sarcoidosis are shown. A. Plain radiograph shows multiple linear and band like opacities in both lungs. Confluent irregular opacities are visible in both parahilar zones. Shadowing is maximal in middle and upper zones. Hilar regions are elevated and overexpanded lower zones are transradiant. B. High-resolution CT scan shows fibrotic masses with associated traction bronchiectasis at central lung region (arrows).
Fig. 6 Imaging findings for fibrosis with honeycombing in sarcoidosis are shown. High-resolution CT image shows interlobular septal thickening, reticular opacities and traction bronchiectasis. Associated subpleural honeycombing is also seen.

Fig. 7 Imaging findings for unilateral hilar lymphadenopathy in sarcoidosis are presented. A. Plain radiograph shows well-circumscribed oval mass in right infrahilar area (arrow). B. Contrast enhanced CT scan reveals presence of enlarged node (arrow) in right interlobar nodal station. Excision biopsy demonstrated presence of sarcoidosis.
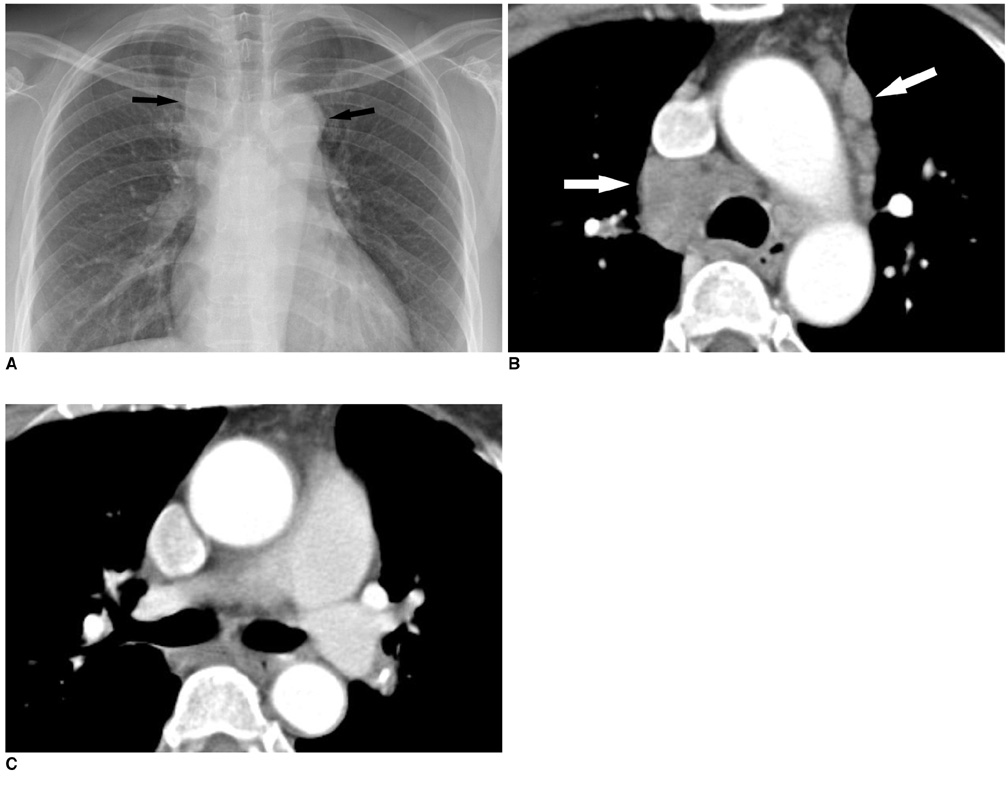
Fig. 8 Imaging findings for mediastinal lymphadenopathy without hilar nodes are presented. A. Plain radiograph shows lymphadenopathy in right paratracheal region and para-aortic area (arrows). Both hilar shadows appear to be normal. B, C. Contrast enhanced CT scans show multiple enlarged nodes with homogeneous attenuation in mediastinum (arrows). However, both hilar zones are preserved.

Fig. 9 Imaging findings for isolated subaortic lymphadenopathy in sarcoidosis are shown. A, B. Contrast enhanced CT scans show presence of enlarged subaortic node (arrow) without hilar and paratracheal lymphadenopathy.

Fig. 10 Imaging findings for necrosis in sarcoidosis are shown. Axial CT scan with lung window setting shows ill-defined irregular consolidation with two small cavities at subpleural region of right middle lobe.

Fig. 11 Imaging findings for alveolar sarcoidosis are shown. Axial CT scan with lung window setting shows ill-defined round consolidation with air bronchogram in right upper lobe.

Fig. 12 Galaxy sign in alveolar sarcoidosis is demonstrated. High-resolution CT scan shows ill-defined nodular opacity resulting from confluence of interstitial granulomas (arrow). Another ill-defined large area with ground glass attenuation is seen with similar appearance as nodular lesion, also suggestive of alveolar sarcoidosis.
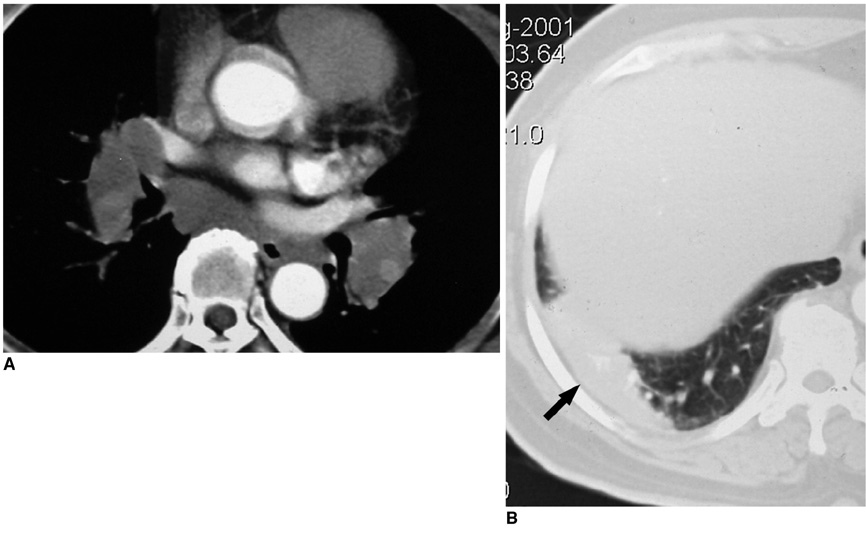
Fig. 13 Imaging findings for subpleural consolidation in sarcoidosis are presented. A. Axial CT scan shows bilateral symmetric hilar lymphadenopathy. B. Axial CT scan with lung window setting shows well-defined, elongated consolidation adjacent to pleura (arrow). Percutaneous CT guided biopsy revealed presence of sarcoidosis.

Fig. 14 Ground glass opacity in sarcoidosis is demonstrated. Axial CT scan with lung window setting shows localized area of ground glass opacity at posterior segment of right upper lobe. Note nodular thickening of peribronchial interstitium (arrow).

Fig. 15 Imaging findings for bronchial narrowing in sarcoidosis are presented. Axial CT scan with lung window setting shows focal narrowing of lateral segmental bronchus of right middle lobe, caused by enlarged peribronchial nodes (arrow). Associated ground glass opacity in right upper lobe is seen.
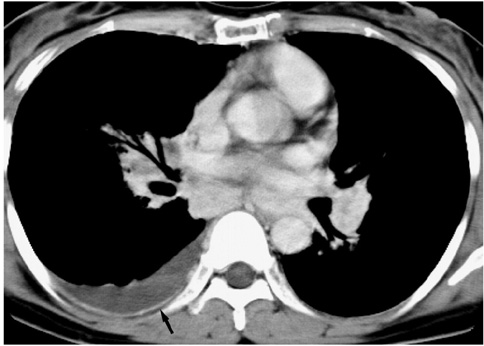
Fig. 16 Pleural involvement in sarcoidosis is demonstrated. Axial CT scan shows bilateral hilar and subcarinal lymphadenopathy, indicating sarcoidosis. Right pleural effusion is present. Note pleural thickening (arrow). Pleural biopsy revealed presence of sarcoidosis.
Reference
-
1. Colby TV, Carrington CB. Thurlbeck WM, editor. Infiltrative lung disease. Pathology of the lung. 1988. Stuttgart: Thieme Medical;425–517.2. Müller NL, Kullnig P, Miller RR. The CT findings of pulmonary sarcoidosis: analysis of 25 patients. AJR Am J Roentgenol. 1989. 152:1179–1182.3. Koyama T, Ueda H, Togashi K, Umeoka S, Kataoka M, Nagai S. Radiologic manifestations of sarcoidosis in various organs. Radiographics. 2004. 24:87–104.4. Hamper UM, Fishman EK, Khouri NF, Johns CJ, Wang KP, Siegelman SS. Typical and atypical CT manifestations of pulmonary sarcoidosis. J Comput Assist Tomogr. 1986. 10:928–936.5. Rockoff SD, Rohatgi PK. Unusual manifestations of thoracic sarcoidosis. AJR Am J Roentgenol. 1985. 144:513–528.6. Baughman RP, Teirstein AS, Judson MA, Rossman MD, Yeager H Jr, Bresnitz EA, et al. Clinical characteristics of patients in a case control study of sarcoidosis. Am J Respir Crit Care Med. 2001. 164:1885–1889.7. Sulavik SB, Spencer RP, Weed DA, Shapiro HR, Shiue ST, Castriotta RJ. Recognition of distinctive patterns of gallium-67 distribution in sarcoidosis. J Nucl Med. 1990. 31:1909–1914.8. Conant EF, Glickstein MF, Mahar P, Miller WT. Pulmonary sarcoidosis in the older patient: conventional radiographic features. Radiology. 1988. 169:315–319.9. Miller BH, Rosado-de-Christenson ML, McAdams HP, Fishback NF. Thoracic sarcoidosis: radiologic-pathologic correlation. Radiographics. 1995. 15:421–437.10. Nakatsu M, Hatabu H, Morikawa K, Uematsu H, Ohno Y, Nishimura K, et al. Large coalescent parenchymal nodules in pulmonary sarcoidosis: "sarcoid galaxy" sign. AJR Am J Roentgenol. 2002. 178:1389–1393.11. Rohatgi PK, Schwab LE. Primary acute pulmonary cavitation in sarcoidosis. AJR Am J Roentgenol. 1980. 134:1199–1203.12. Nishimura K, Itoh H, Kitaichi M, Nagai S, Izumi T. Pulmonary sarcoidosis: correlation of CT and histopathologic findings. Radiology. 1993. 189:105–109.13. Huggins JT, Doelken P, Sahn SA, King L, Judson MA. Pleural effusions in a series of 181 outpatients with sarcoidosis. Chest. 2006. 129:1599–1604.
