Comparison of Delayed-Onset Glaucoma and Early-Onset Glaucoma after Infantile Cataract Surgery
- Affiliations
-
- 1Department of Ophthalmology, St. Mary's Hospital, College of Medicine, The Catholic University of Korea, Seoul, Korea.
- 2Our Lady of Mercy Hospital, College of Medicine, The Catholic University of Korea, Seoul, Korea. yimhb@catholic.ac.kr
- 3Department of Ophthalmology, University of Pittsburgh School of Medicine, Pittsburgh, USA.
- KMID: 1099071
- DOI: http://doi.org/10.3341/kjo.2006.20.1.41
Abstract
- PURPOSE: To investigate the causes and characteristics of glaucoma in children following cataract surgery. METHODS: Twenty-four patients (37 eyes) with uncomplicated congenital cataracts who developed glaucoma after cataract surgery were studied retrospectively. Variables included cataract morphology, surgical techniques, post-operative complications, time to the onset of glaucoma, gonioscopic findings, presence of microcornea and the histopathologic characteristics of the filtration angle (in one case). RESULTS: There was a bimodal onset of glaucoma after cataract surgery. Early-onset glaucoma occurred at a mean age of 6 months in 15 eyes and delayed-onset glaucoma at a mean age of 12 years in 22 eyes. Early-onset glaucoma was significantly (p=0.018) more likely to be due to angle closure than delayed-onset glaucoma. With delayed-onset glaucoma, the filtration angle was open in 86% of eyes and significantly (p=0.006) more eyes in the delayed-onset group had microcornea. Medical treatment was sufficient to control intraocular pressure in the delayed-onset group while the early-onset group required surgical treatment (P<0.001). CONCLUSIONS: The onset of glaucoma after cataract surgery during infancy follows a bimodal pattern that is correlated with the configuration of the filtration angle. The early-onset glaucoma group had high incidence of angle closure requiring surgical treatment, while in the delayed-onset group non-surgical treatment was sufficient to control intraocular pressure. Prophylactic iridectomy in eyes at risk for pupillary block is recommended. Eyes with delayed-onset glaucoma have open filtration angles yet also have findings of incomplete development of filtration structures. Microcornea is a risk factor for delayed-onset glaucoma.
Keyword
MeSH Terms
-
Time Factors
Risk Factors
Retrospective Studies
Postoperative Complications
Male
Intraocular Pressure
Infant
Humans
Gonioscopy
Glaucoma, Open-Angle/diagnosis/*etiology/physiopathology
Glaucoma, Angle-Closure/diagnosis/*etiology/physiopathology
Follow-Up Studies
Female
Child, Preschool
Child
Cataract Extraction/*adverse effects
Cataract/congenital
Age Factors
Adult
Adolescent
Figure
-
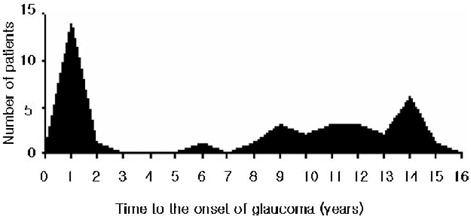
Fig. 1 Time (years) to the onset of glaucoma following removal of cataracts diagnosed before one year of age and removed before five years of age.
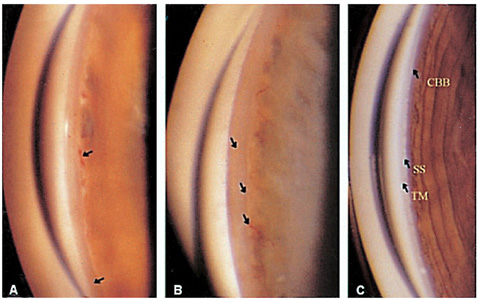
Fig. 2 (A and B) Gonioscopic appearance of two eyes with microcornea and delayed-onset aphakic glaucoma. Note the high iris insertion, lack of angle recess, lack of iris surface undulation, visible iris vessels, and pigmented membranous tissue covering the angle (black arrows in A and B). The scleral spur (SS) is indiscriminate. (C) Gonioscopic appearance of an age-matched normal eye with congenital nuclear cataract and microcornea. Note the normal appearance of the iris, ciliary body band (CBB), SS, and trabecular meshwork (TM).
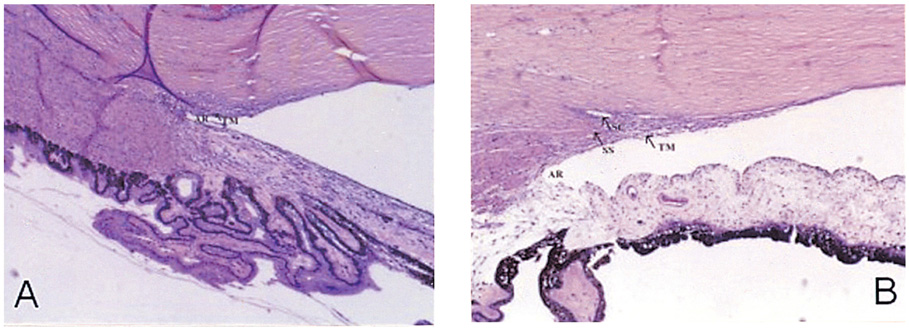
Fig. 3 (A) Histopathologic view of an angle with delayed-onset aphakic glaucoma. There is no identifiable Schlemm's canal (SC), the scleral spur (SS) is indistinct, and the trabecular meshwork (TM) is compact. The angle recess (AR) is poorly developed (H&E, magnification, ×12). (B) An age-matched normal filtration angle of a 15-year-old female who received enucleation due to retinoblastoma (H&E, magnification, ×12).
Cited by 1 articles
-
Risk Factors of Secondary Glaucoma after Congenital Cataract Surgery in Korean Patients
Ga-In Lee, Jong Chul Han, Si Bum Kim, Eun Jung Lee, Chang Won Kee
J Korean Ophthalmol Soc. 2018;59(6):569-576. doi: 10.3341/jkos.2018.59.6.569.
Reference
-
1. Chandler PA. Surgery for congenital cataract. Am J Ophthalmol. 1968. 65:663–673.2. Phelps CD, Arafat NI. Open-angle glaucoma following surgery for congenital cataracts. Arch Ophthalmol. 1977. 95:1985–1987.3. Chrousos GA, Parks MM, O'Neill JF. Incidence of chronic glaucoma, retinal detachment and secondary surgery in pediatric aphakic patients. Ophthalmology. 1984. 91:1238–1241.4. Keech RV, Tongue AC, Scott WE. Complications after surgery for congenital and infantile cataracts. Am J Ophthalmol. 1989. 108:136–141.5. Simon JW, Mehta N, Simmons ST, et al. Glaucoma after pediatric lensectomy / vitrectomy. Ophthalmology. 1991. 98:670–674.6. Parks MM, Johnson DA, Reed GW. Long-term visual results and complications in children with aphakia: A function of cataract type. Ophthalmology. 1993. 100:826–841.7. Mills MD, Robb RM. Glaucoma following childhood cataract surgery. J Pediatr Ophthalmol Strabismus. 1994. 31:355–360.8. Walton DS. Pediatric aphakic glaucoma: A study of 65 patients. Trans Am Ophthalmol Soc. 1995. 93:403–420.9. Asrani SG, Wilensky JT. Glaucoma after congenital cataract surgery. Ophthalmology. 1995. 102:863–867.10. Magnusson G, Abrahamsson M, Sjostrand J. Glaucoma following cataract surgery: An 18-year longitudinal follow-up. Acta Ophthalmol Scand. 2000. 78:65–70.11. Chen TC, Walton DS, Bhatia LS. Aphakic glaucoma after congenital cataract surgery. Arch Ophthalmol. 2004. 122:1819–1825.12. Vishwanath M, Cheong-Leen R, Taylor D, et al. Is early surgery for congenital cataract a risk factor for glaucoma? Br J Opthalmol. 2004. 88:905–910.13. Rabiah P. Frequency and predictors of glaucoma after pediatric cataract surgery. Am J Ophthalmol. 2004. 137:30–37.14. Eustis SH, Walton RC, Ball SF. Pupillary block glaucoma following pediatric cataract extraction. Ophthalmic Surg. 1990. 21:413–415.15. Pressman SH, Crouch ER. Pediatric aphakic glaucoma. Ann Ophthalmol. 1983. 15:568–573.16. Wallace DK, Plager DA. Corneal diameter in childhood aphakic glaucoma. J Pediatr Ophthalmol Strabismus. 1996. 33:230–234.17. Egbert JE, Wright MM, Dahlhauser KF, et al. A prospective study of ocular hypertension and glaucoma after pediatric cataract surgery. Ophthalmology. 1995. 102:1098–1101.18. Johnson CP, Keech RV. Prevalence of glaucoma after surgery for PHPV and infantile cataracts. J Pediatr Ophthalmol Strabismus. 1996. 33:14–17.19. Cheng KP, Hiles DA, Biglan AW, et al. Visual results after early surgical treatment of unilateral congenital cataracts. Ophthalmology. 1991. 98:903–910.20. Hosal BM, Biglan AW, Elhan AH. High levels of binocular function are achievable after removal of monocular cataracts in children before 8 years of age. Ophthalmology. 2000. 107:1647–1655.21. Mori M, Keech RV, Scott WE. Glaucoma and ocular hypertension in pediatric patients with cataracts. J AAPOS. 1997. 1:98–101.22. Brady KM, Atkinson CS, Kilty LA, et al. Glaucoma after cataract extraction and posterior chamber lens implantation in children. J Cataract Refract Surg. 1997. 23:669–674.23. Vajpayee RB, Angra SK, Titiyal JS, et al. Pseudophakic pupillary-block glaucoma in children. Am J Ophthalmol. 1991. 111:715–718.24. Tawara A, Inomata H, Tsukamoto S. Ciliary body band width as an indicator of goniodysgenesis. Am J Ophthalmol. 1996. 122:790–800.25. Shields MB. Brown CL, Vaughn VM, Knighten DL, editors. Primary congenital glaucoma. Textbook of Glaucoma. 1992. 3rd ed. Baltimore: Williams&Wilkins;chap. 11.26. Kaufman PL. Hart W, editor. Accommodation. Adler's Physiology of the Eye; Clinical Application. 1992. 9th ed. St. Louis: Mosby;chap. 11.27. Armaly MF. Studies on intraocular effects of the orbital parasympathetic pathway. I. Technique and effects on morphology. II. Effect on intraocular pressure. III. Effect on steady-state dynamics. Arch Ophthalmol. 1959. 61:14–29.28. Allen L, Burian HM. The valve action of the trabecular meshwork. Am J Ophthalmol. 1965. 59:382–389.29. Coleman DJ. Unified model for accommodative mechanism. Am J Ophthalmol. 1970. 69:1063–1079.30. Coleman DJ, Fish SK. Presbyopia, accommodation, and the mature cataracts. Ophthalmology. 2001. 108:1544–1551.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case of Ocular Siderosis with Cataract and Delayed-Onset Secondary Glaucoma
- Clinical Result of Trabeculotomy(ab externo)
- Clinical Factors that Influence Intraocular Pressure Change after Cataract Surgery in Primary Open-Angle Glaucoma and Angle-Closure Glaucoma
- Spontaneous Anterior Lens Capsular Dehiscence Causing Lens Particle Glaucoma
- Evaluation of Combined Cataract and Glaucoma Operation
