Reversible Lansoprazole-Induced Interstitial Lung Disease Showing Improvement after Drug Cessation
- Affiliations
-
- 1Department of Radiology, College of Medicine, Korea University, Guro Hospital, Seoul, Korea. wokhee@unitel.co.kr
- 2Department of Pathology, College of Medicine, Korea University, Guro Hospital, Seoul, Korea.
- 3Department of Internal Medicine, College of Medicine, Korea University, Guro Hospital, Seoul, Korea.
- KMID: 1098197
- DOI: http://doi.org/10.3348/kjr.2008.9.2.175
Abstract
- Lansoprazole is an acid proton-pump inhibiting drug that is used for the treatment of duodenal or gastric ulcers, H. pylori infection, gastroesophageal reflux disease or Zollinger-Ellison syndrome. Although lansoprazole is well known for its gastrointestinal and dermatologic adverse effects, mild pulmonary symptoms are also known to develop from taking this drug. There have been no reports about lansoprazole-induced interstitial lung disease. We report here a case of lansoprazole-induced interstitial lung disease that developed in a 66-year-old man.
MeSH Terms
Figure
-
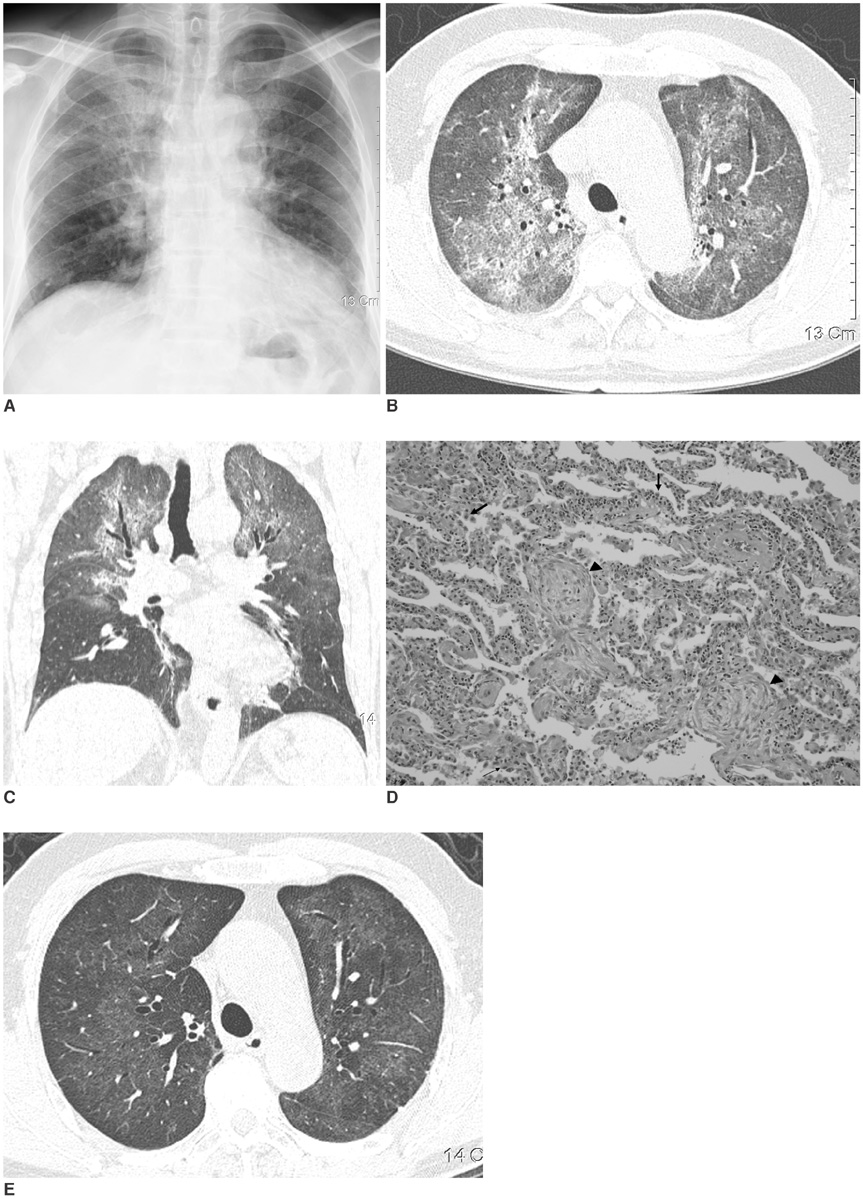
Fig. 1 Lansoprazole-induced interstitial lung disease. A. Posteroanterior chest radiograph shows diffuse ground-glass opacities in both lungs, which are predominant in upper lung zones. B, C. Axial (B) and coronal (C) reconstruction high-resolution CT images show areas of diffuse ground-glass opacity in both lungs with upper lung predominance, similar to those seen in chest radiograph (A). D. Histopathological specimen shows mixed interstitial infiltration of lymphocytes and plasma cells, suggestive of nonspecific interstitial pneumonia pattern. Note active hyperplasia of type II pneumocytes (arrows) and Massons' body (arrowheads). E. Follow-up high resolution CT image shows markedly improved opacities in both lungs. Faint areas of ground-glass opacity still remain.
Reference
-
1. Pietra GG. Pathologic mechanism of drug-induced lung disorders. J Thorac Imaging. 1991. 6(1):1–7.2. Kohno S, Yamaguchi K, Yasuoka A, Koga H, Hayashi T, Komori K, et al. Clinical evaluation of 12 cases of antimicrobial drug-induced pneumonitis. Jpn J Med. 1990. 29:248–254.3. Akira M, Ishikawa H, Yamamoto S. Drug-induced pneumonitis: thin-section CT findings in 60 patients. Radiology. 2002. 224:852–860.4. Rossi SE, Erasmus JJ, McAdams HP, Sporn TA, Goodman PC. Pulmonary drug toxicity: radiologic and pathologic manifestation. Radiographics. 2000. 20:1245–1259.5. Cleverley JR, Screaton NJ, Hiorns MP, Flint JD, Muller NL. Drug-induced lung disease: high-resolution CT and histologic findings. Clin Radiol. 2002. 57:292–299.6. Fraser RS, Muller NL, Colman N, Pare PD. Fraser & Pare: Diagnosis of disease of the chest. 1999. 4th ed. Philadelphia: Saunders;2537–2540.
