Cardiac Dysrhythmias, Cardiomyopathy and Muscular Dystrophy in Patients with Emery-Dreifuss Muscular Dystrophy and Limb-Girdle Muscular Dystrophy Type 1B
- Affiliations
-
- 1Department of Internal Medicine, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea. dkkim@smc.samsung.co.kr
- 2Department of Clinical Pathology, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea.
- 3Department of Diagnostic Pathology, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea.
- 4Department of Neurology, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea.
- 5Department of Internal Medicine, Han-il General Hospital, Seoul, Korea.
- KMID: 1095205
- DOI: http://doi.org/10.3346/jkms.2005.20.2.283
Abstract
- Emery-Dreifuss muscular dystrophy (EDMD) and limb-girdle muscular dystrophy type 1B (LGMD1B) are characterized by cardiac dysrhythmias, late-onset cardiomyopathy, slowly progressive skeletal myopathy and contractures of the neck, elbows and ankles. The causative mutation is either in the emerin gene (X-linked recessive EDMD) or lamin A/C gene (autosomal dominant EDMD2 or LGMD1B). We report three cases of EDMD, EDMD2 and LGMD1B. A 14-yr-old boy showed limitation of cervical flexion and contractures of both elbows and ankles. Sinus arrest with junctional escape beats was noted. He was diagnosed as X-linked recessive EDMD (MIM 310300). A 28-yr-old female showed severe wasting and weakness of humeroperoneal muscles. Marked limitation of cervical flexion and contractures of both elbows and ankles were noted. Varying degrees of AV block were noted. She was diagnosed as autosomal dominant EDMD2 (MIM 181350). A 41-yr-old female had contractures of both ankles and limb-girdle type muscular dystrophy. ECG revealed atrial tachycardia with high grade AV block. She was diagnosed as autosomal dominant LGMD1B (MIM 159001). Cardiac dysrhythmias in EDMD and LGMD1B include AV block, bradycardia, atrial tachycardia, atrial fibrillation, and atrial standstill, causing sudden death necessitating pacemaker implantation. Cardiologists should know about these unusual genetic diseases with conduction defects, especially in young adults.
MeSH Terms
Figure
-
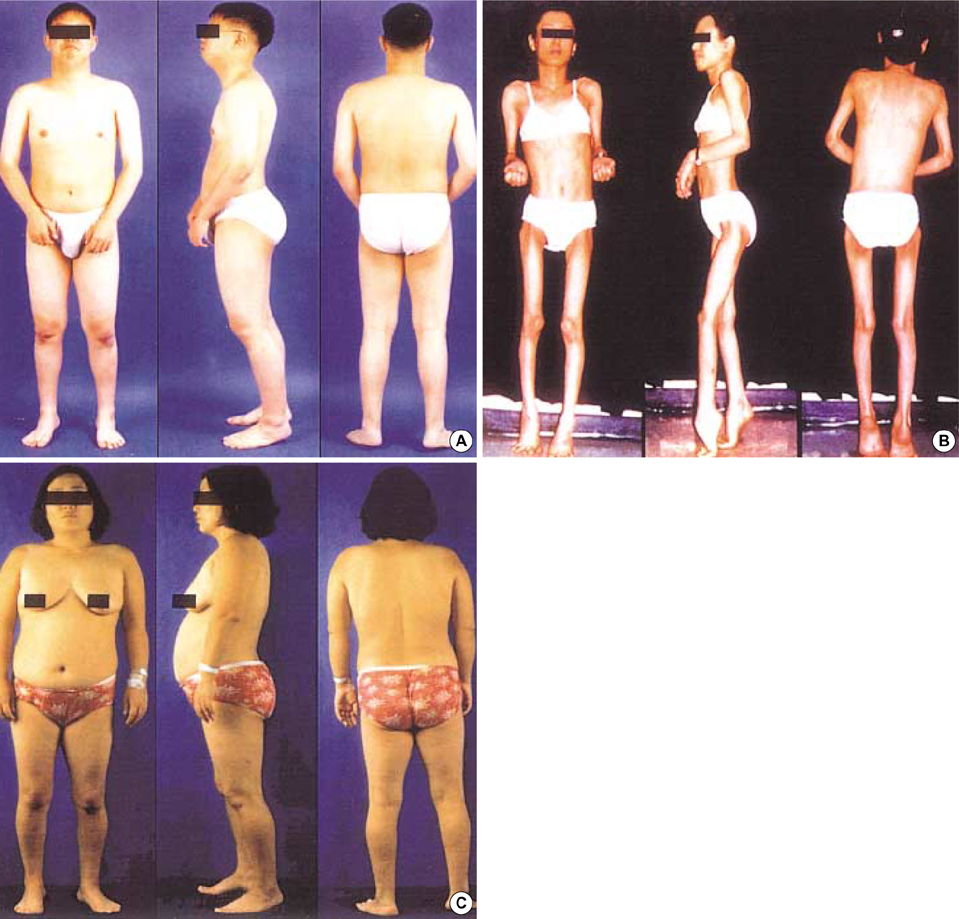
Fig. 1 Photographs of each patient. (A) XR EDMD patient (case 1) showing flexion contractures of both elbows and Achilles tendons. (B) AD EDMD2 patient (case 2) showing marked muscular atrophy of upper and lower extremities with flexion contractures of both elbows and Achilles tendons. The patient keeps her heel off the floor with equinus deformities of the feet. (C) LGMD1B patient (case 3) shows peroneal dystrophy with Achilles tendon contractures. Equinus deformity of the right foot is more severe than the left one.
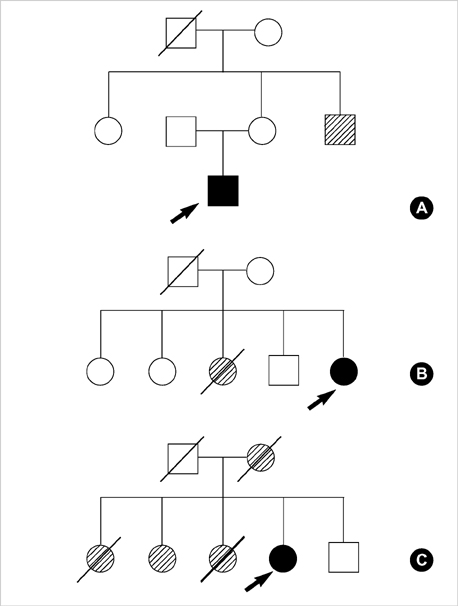
Fig. 2 Pedigrees of the families with XR EDMD (A), AD EDMD2 (B) and LGMD1B (C). Squares indicate male family members, circles female family members and symbols with a slash mark deceased family members. Open symbols indicate unaffected family members, filled symbols indicate the presence of neuromuscular and cardiac symptoms, and shaded symbols indicate family members who are or were probably affected. Arrows represent proband. B and C from reference 8.
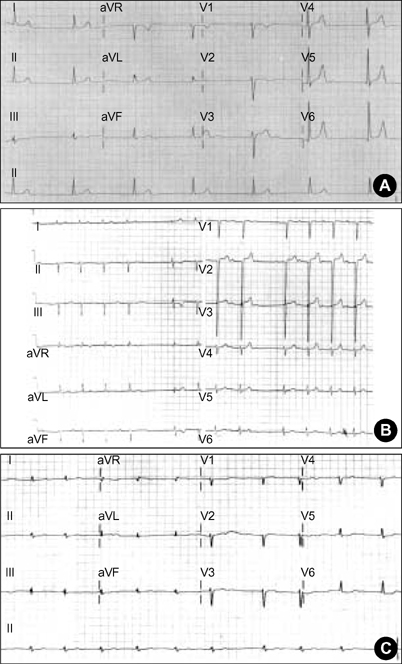
Fig. 3 12-lead ECG of EDMD (A), AD EDMD2 (B) and LGMD1B (C). (A) The ECG shows sinus arrest with junctional escape rhythm at a heart rate of 40 beats per minute. (B) The ECG shows left axis deviation, left anterior hemiblock, first-degree atrioventricular block, and sinus pause. (C) The ECG shows atrial fibrillation with ST-T changes.
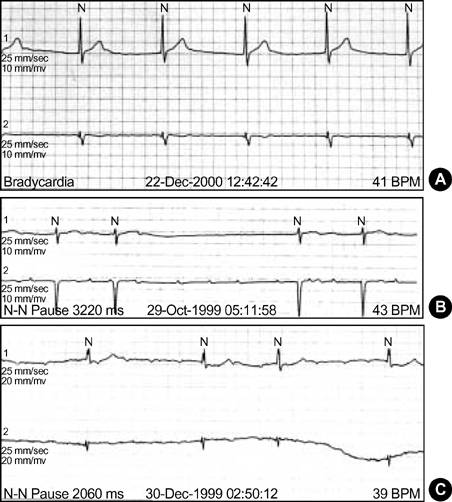
Fig. 4 Findings of ambulatory ECG monitorings of EDMD (A), AD EDMD2 (B) and LGMD1B (C). (A) Atrial fibrillation with complete AV block and junctional escape rhythm. (B) Slow nonsustained atrial tachycardia at a rate of 120 beats per minute with high grade AV block. (C) Atrial tachycardia and high grade (3:1, 4:1) AV block with the longest R-R interval of 2.06 sec.
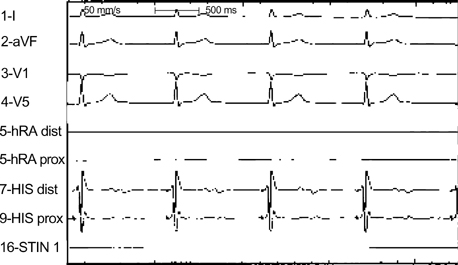
Fig. 5 Findings of electrophysiologic study in a patient with XR EDMD (case 1). Electrophysiologic study shows no electrical signal in the right upper atrium. Junctional escape beats are noted.
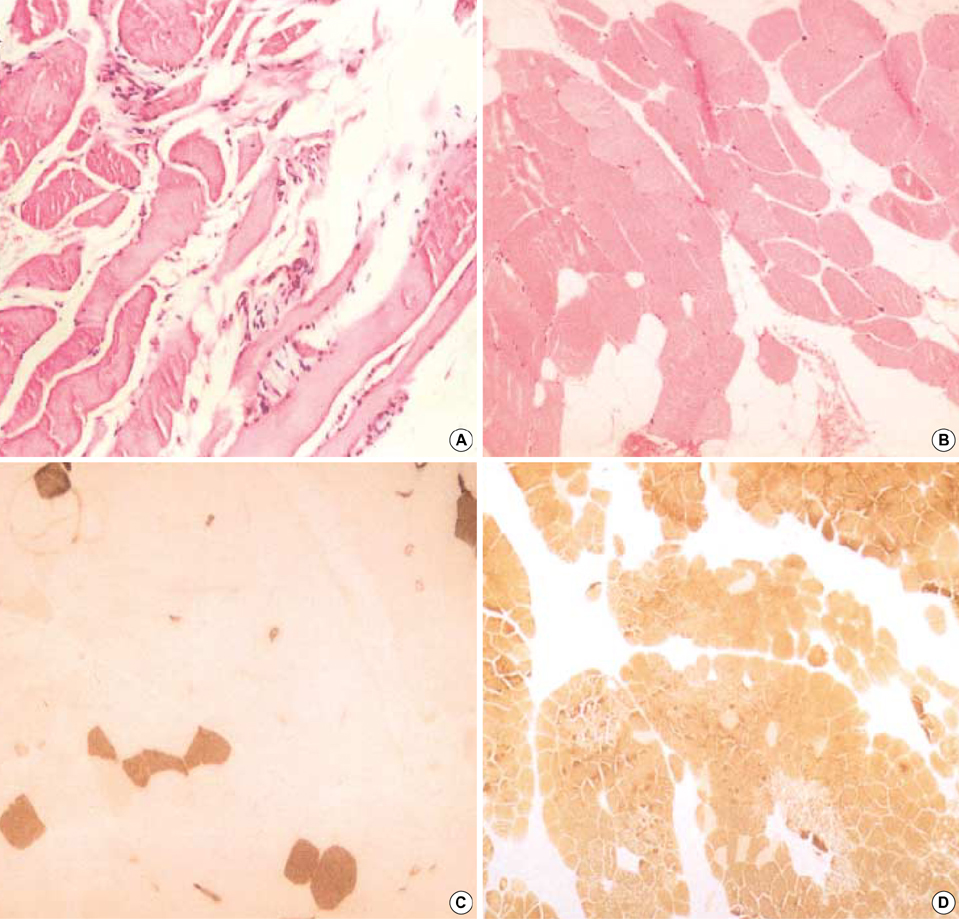
Fig. 6 The histopathologic findings of skeletal muscle biopsy specimen in AD EDMD2 (A) and LGMD1B (B-D) patient. (A) Myofibers are reduced in number and replaced by fibroadipose tissues. There are atrophic or hypertrophic myofibers, internalization of sarcolemmal nuclei and fiber splitting (hematoxylin and eosin stain, ×200). (B) Variation in myofiber size, frequent internal nuclei and fatty ingrowth are noted in hematoxylin and eosin stain (×200). (C) ATPase pH 4.6 stain reveals atrophy of type 1 fibers (dark brown stain, ×200). (D) ATPase pH 9.4 stain reveals a predominance of type 2 fibers (brown stain, ×100).
Reference
-
1. Bione S, Maestrini E, Rivella S, Mancini M, Regis S, Romeo G, Toniolo D. Identification of a novel X-linked gene responsible for Emery-Dreifuss muscular dystrophy. Nat Genet. 1994. 8:323–327.
Article2. Nagano A, Koga R, Ogawa M, Kurano Y, Kawada J, Okada R, Hayashi YK, Tsukahara T, Arahata K. Emerin deficiency at the nuclear membrane in patients with Emery-Dreifuss muscular dystrophy. Nat Genet. 1996. 12:254–259.3. Bonne G, Di Barletta MR, Varnous S, Becane HM, Hammouda EH, Merlini L, Muntoni F, Greenberg CR, Gary F, Urtizberea JA, Duboc D, Fardeau M, Toniolo D, Schwartz K. Mutation in the gene encoding lamin A/C cause autosomal dominant Emery-Dreifuss muscular dystrophy. Nat Genet. 1999. 21:285–288.4. Muchir A, Bonne G, van der Kooi AJ, van Meegen M, Baas F, Bolhuis PA, de Visser M, Schwartz K. Identification of mutations in the gene encoding lamins A/C in autosomal dominant limb girdle muscular dystrophy with atrioventricular conduction disturbances (LGMD1B). Hum Mol Genet. 2000. 9:1453–1459.
Article5. Fatkin D, MacRae C, Sasaki T, Wolff MR, Porcu M, Frenneaux M, Atherton J, Vidaillet HJ Jr, Spudich S, de Girolami U, Seidman JG, Seidman C, Muntoni F, Muehle G, Johnson W, McDonough B. Missense mutations in the rod domain of the lamin A/C gene as causes of dilated cardiomyopathy and conduction-system disease. N Engl J Med. 1999. 341:1715–1724.
Article6. Shackleton S, Lloyd D, Jackson SN, Evans R, Niermeijer MF, Singh BM, Schmidt H, Brabant G, Kumar S, Durrington PN, Gregory S, O'Rahilly S, Trembath RC. LMNA, encoding lamin A/C, is mutated in partial lipodystrophy. Nat Genet. 2000. 24:153–156.
Article7. Bonne G, Mercuri E, Muchir A, Urtizberea A, Becane HM, Recan D, Merlini L, Wehnert M, Boor R, Reuner U, Vorgerd M, Wicklein EM, Eymard B, Duboc D, Penisson-Besnier I, Cuisset JM, Ferrer X, Desguerre I, Lacombe D, Bushby K, Pollitt C, Toniolo D, Fardeau M, Schwartz K, Muntoni F. Clinical and molecular genetic spectrum of autosomal dominant Emery-Dreifuss muscular dystrophy due to mutations of the lamin A/C gene. Ann Neurol. 2000. 48:170–180.
Article8. Ki CS, Hong JS, Jeong GY, Ahn KJ, Choi KM, Kim DK, Kim JW. Identification of lamin A/C (LMNA) gene mutations in Korean patients with autosomal dominant Emery-Dreifuss muscular dystrophy and limb-girdle muscular dystrophy 1B. J Hum Genet. 2002. 47:225–228.
Article9. Hong JS, Kang JH, Lee GS, Lee CS, Choi HJ, Lee BD, Kim JS, Suh YL, Kim DK, Chi JG, Ahn KJ. A case of high degree AV block treated by implantation of permanent pacemaker in Emery-Dreifuss muscular dystrophy. Korean Circ J. 2000. 30:1316–1322.
Article10. Kim SE, Hong JS, Ahn KJ, Kim JS, Kim DK. A case of Emery-Dreifuss muscular dystrophy by emerin gene mutation. Korean Circ J. 2003. 33:143–149.
Article11. Cartegni L, di Barletta MR, Barresi R, Squarzoni S, Sabatelli P, Maraldi N, Mora M, Di Blasi C, Cornelio F, Merlini L, Villa A, Cobianchi F, Toniolo D. Heart-specific localization of emerin: new insights into Emery-Dreifuss muscular dystrophy. Hum Mol Genet. 1997. 6:2257–2264.
Article12. Hutchison CJ, Alvarez-Reyes M, Vaughan OA. Lamins in disease: why do ubiquitously expressed nuclear envelope proteins give rise to tissue-specific disease phenotypes? J Cell Sci. 2001. 114:9–19.
Article13. Arbustini E, Pilotto A, Repetto A, Grasso M, Negri A, Diegoli M, Campana C, Scelsi L, Baldini E, Gavazzi A, Tavazzi L. Autosomal dominant dilated cardiomyopathy with atrioventricular block: A lamin A/C defect-related disease. J Am Coll Cardiol. 2002. 39:981–990.
Article14. Emery AE. Emery-Dreifuss muscular dystrophy - a 40 year retrospective. Neuromuscul Disord. 2000. 10:228–232.
Article15. van der Kooi AJ, Ledderhof TM, de Voogt WG, Res CJ, Bouwsma G, Troost D, Busch HF, Becker AE, de Visser M. A newly recognized autosomal dominant limb girdle muscular dystrophy with cardiac involvement. Ann Neurol. 1996. 39:636–642.
Article16. Marshall TM, Huckell VF. Atrial paralysis in a patient with Emery-Dreifuss muscular dystrophy. Pacing Clin Electrophysiol. 1992. 15:135–140.
Article17. Fishbein MC, Siegel RJ, Thompson CE, Hopkins LC. Sudden death of a carrier of X-linked Emery-Dreifuss muscular dystrophy. Ann Intern Med. 1993. 119:900–905.
Article18. Zacharias AS, Wagener ME, Warren ST, Hopkins LC. Emery-Dreifuss muscular dystrophy. Semin Neurol. 1999. 19:67–79.
Article19. Merlini L, Granata C, Dominici P, Bonfiglioli S. Emery-Dreifuss muscular dystrophy: report of five cases in a family and review of the literature. Muscle Nerve. 1986. 9:481–485.
Article20. Vohanka S, Vytopil M, Bednarik J, Lukas Z, Kadanka Z, Schildberger J, Ricotti R, Bione S, Toniolo D. A mutation in the X-linked Emery-Dreifuss muscular dystrophy gene in a patient affected with conduction cardiomyopathy. Neuromuscul Disord. 2001. 11:411–413.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Early-Onset LMNA-Associated Muscular Dystrophy with Later Involvement of Contracture
- Emery-Dreifuss Muscular Dystrophy with Cardiac Involvement
- A Case of High Degree AV Block Treated by Implantation of Permanent Pacemaker in Emery-Dreifuss Muscular Dystrophy
- Two Cases of Oculopharyngeal Muscular Dystrophy in One Family
- Emery Dreifuss muscular Dystrophy: A case report
