Korean J Radiol.
2009 Oct;10(5):481-489. 10.3348/kjr.2009.10.5.481.
Prediction of Mortality after Emergent Transjugular Intrahepatic Portosystemic Shunt Placement: Use of APACHE II, Child-Pugh and MELD Scores in Asian Patients with Refractory Variceal Hemorrhage
- Affiliations
-
- 1Department of Radiology, Chi-Mei Foundation Medical Center, Tainan, Taiwan. 520006@mail.chimei.org.tw
- 2Section of Gastroenterology, Chi-Mei Foundation Medical Center, Tainan, Taiwan.
- 3Section of Hepatology, Chi-Mei Foundation Medical Center, Tainan, Taiwan.
- 4Department of Radiological Technology, Central Taiwan University of Science and Technology, Taichung, Taiwan.
- 5Department of Radiology, Tri-Service General Hospital, National Defense Medical Center, Neihu, Taipei City, Taiwan.
- 6Hospital and Health Care Administration, Chia Nan University of Pharmacy and Science, Tainan, Taiwan.
- KMID: 1093963
- DOI: http://doi.org/10.3348/kjr.2009.10.5.481
Abstract
OBJECTIVE
This study was designed to determine if existing methods of grading liver function that have been developed in non-Asian patients with cirrhosis can be used to predict mortality in Asian patients treated for refractory variceal hemorrhage by the use of the transjugular intrahepatic portosystemic shunt (TIPS) procedure. MATERIALS AND METHODS: Data for 107 consecutive patients who underwent an emergency TIPS procedure were retrospectively analyzed. Acute physiology and chronic health evaluation (APACHE II), Child-Pugh and model for end-stage liver disease (MELD) scores were calculated. Survival analyses were performed to evaluate the ability of the various models to predict 30-day, 60-day and 360-day mortality. The ability of stratified APACHE II, Child-Pugh, and MELD scores to predict survival was assessed by the use of Kaplan-Meier analysis with the log-rank test. RESULTS: No patient died during the TIPS procedure, but 82 patients died during the follow-up period. Thirty patients died within 30 days after the TIPS procedure; 37 patients died within 60 days and 53 patients died within 360 days. Univariate analysis indicated that hepatorenal syndrome, use of inotropic agents and mechanical ventilation were associated with elevated 30-day mortality (p < 0.05). Multivariate analysis showed that a Child-Pugh score > 11 or an MELD score > 20 predicted increased risk of death at 30, 60 and 360 days (p < 0.05). APACHE II scores could only predict mortality at 360 days (p < 0.05). CONCLUSION: A Child-Pugh score > 11 or an MELD score > 20 are predictive of mortality in Asian patients with refractory variceal hemorrhage treated with the TIPS procedure. An APACHE II score is not predictive of early mortality in this patient population.
Keyword
MeSH Terms
Figure
-
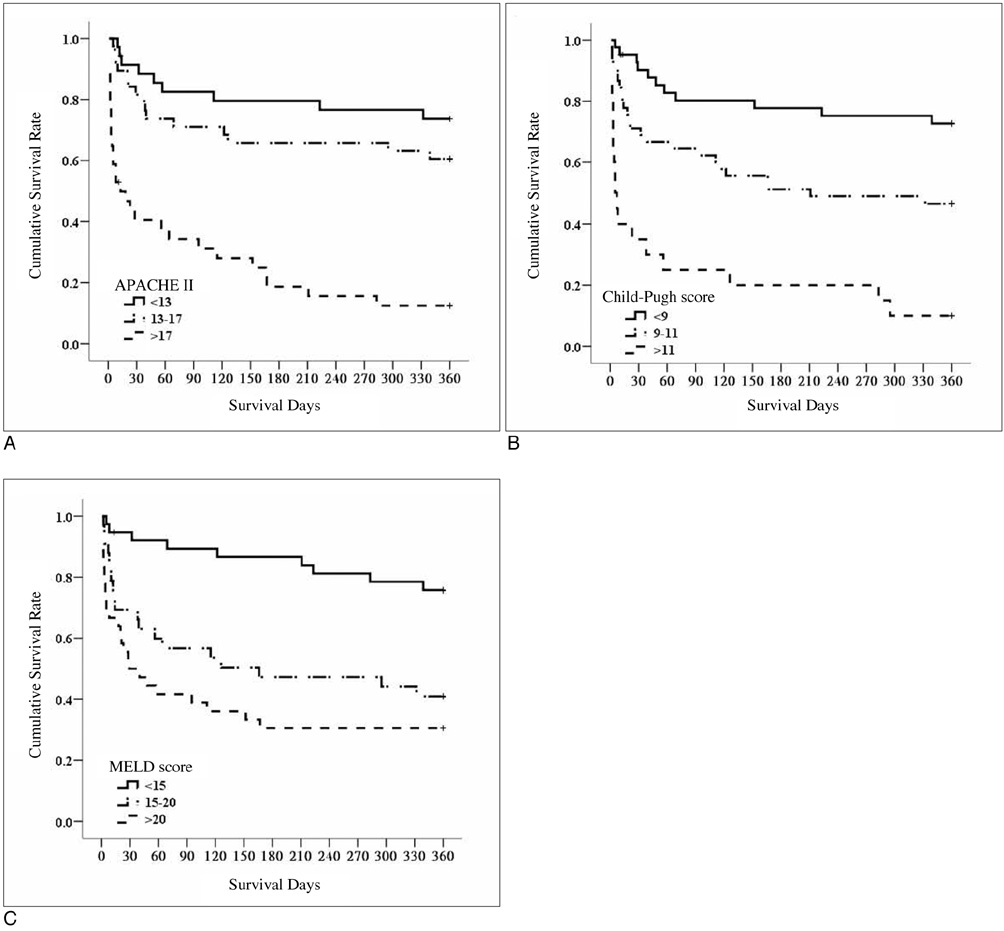
Fig. 1 Kaplan-Meier 360-day survival curves based on (A) acute physiology and chronic health evaluation scores, (B) Child-Pugh scores and (C) model for end-stage liver disease scores. Tertile difference for 30-day, 60-day and 360-day survival was significant (log-rank test, all p < 0.01).
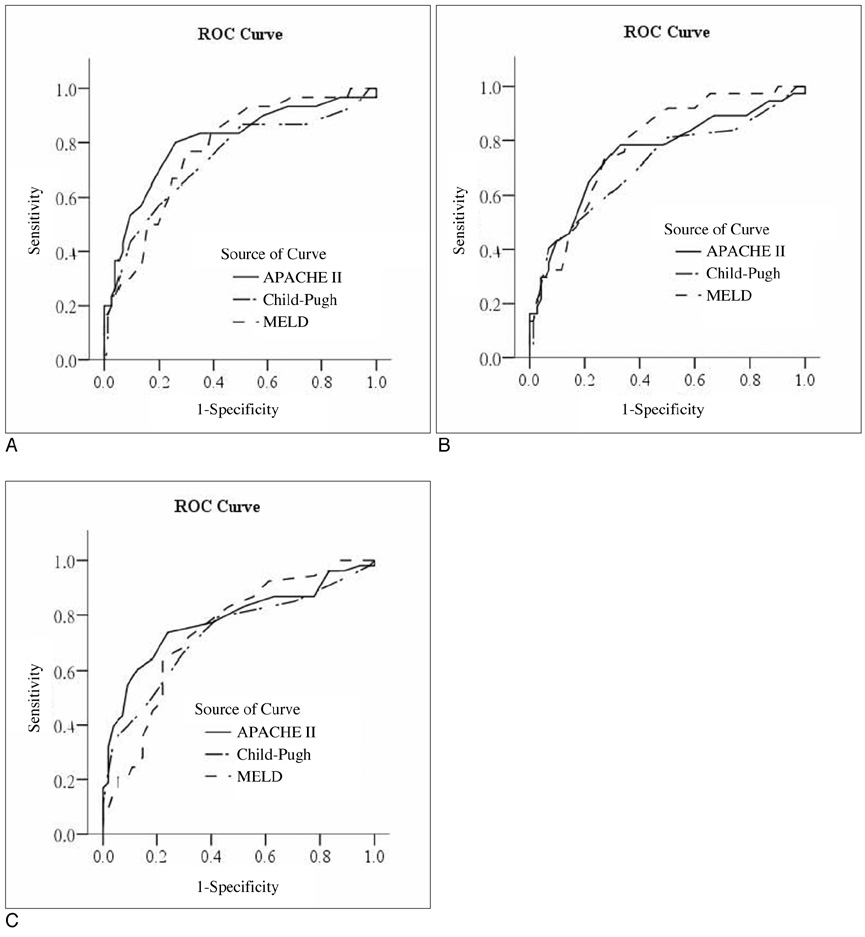
Fig. 2 Receiver operating characteristics curves for acute physiology and chronic health evaluation, Child-Pugh and model for end-stage liver disease for (A) 30-day, (B) 60-day, and (C) 360-day mortality.
Reference
-
1. Coldwell DM, Ring EJ, Rees CR, Zemel G, Darcy MD, Haskal ZJ, et al. Multicenter investigation of the role of transjugular intrahepatic portosystemic shunt in management of portal hypertension. Radiology. 1995. 196:335–340.2. Luca A, D'Amico G, La Galla R, Midiri M, Morabito A, Pagliaro L. TIPS for prevention of recurrent bleeding in patients with cirrhosis: meta-analysis of randomized clinical trials. Radiology. 1999. 212:411–421.3. Rossle M, Haag K, Ochs A, Sellinger M, Noldge G, Perarnau JM, et al. The transjugular intrahepatic portosystemic stent-shunt procedure for variceal bleeding. N Engl J Med. 1994. 330:165–171.4. Shiffman ML, Jeffers L, Hoofnagle JH, Tralka TS. The role of transjugular intrahepatic portosystemic shunt for treatment of portal hypertension and its complications: a conference sponsored by the National Digestive Diseases Advisory Board. Hepatology. 1995. 22:1591–1597.5. Banares R, Casado M, Rodriguez-Laiz JM, Camunez F, Matilla A, Echenagusia A, et al. Urgent transjugular intrahepatic portosystemic shunt for control of acute variceal bleeding. Am J Gastroenterol. 1998. 93:75–79.6. Sanyal AJ, Freeman AM, Lutetic VA, Purdum PP, Shiffman ML, Tisnado J, et al. Transjugular intrahepatic portosystemic shunts for patients with active variceal hemorrhage unresponsive to sclerotherapy. Gastroenterology. 1996. 111:138–146.7. McCormick PA, Dick R, Panagou EB, Chin JK, Greenslade L, McIntyre N, et al. Emergency transjugular intrahepatic portasystemic stent shunting as salvage treatment for uncontrolled variceal bleeding. Br J Surg. 1994. 81:1324–1327.8. Chalasani N, Clark WS, Martin LG, Kamean J, Khan MA, Patel NH, et al. Determinants of mortality in patients with advances cirrhosis after transjugular intrahepatic portosystemic shunting. Gastroenterology. 2000. 118:138–144.9. Malinchoc M, Kamath PS, Gordon FD, Peine CJ, Rank J, ter Borg PC. A model to predict poor survival in patients undergoing transjugular intrahepatic portosystemic shunts. Hepatology. 2000. 31:864–871.10. Rubin RA, Haskal ZJ, O'Brien CB, Cope C, Brass CA. Transjugular intrahepatic portosystemic shunting: decreased survival for patients with high APACHE II scores. Am J Gastroenterol. 1995. 90:556–563.11. Patch D, Nikolopoulou V, McCormick A, Dick R, Armonis A, Wannamethee G, et al. Factors related to early mortality after transjugular intrahepatic portosystemic shunt for failed endoscopic therapy in acute variceal bleeding. J Hepatol. 1998. 28:454–460.12. Rajan DK, Haskal ZJ, Clark TW. Serum bilirubin and early mortality after transjugular intrahepatic portosystemic shunts: results of a multivariate analysis. J Vasc Interv Radiol. 2002. 13:155–161.13. Brensing KA, Raab P, Textor J, Gorich J, Schiedermaier P, Strunk H, et al. Prospective evaluation of a clinical score for 60-day mortality after transjugular intrahepatic portosystemic stent-shunt: Bonn TIPSS early mortality analysis. Eur J Gastroenterol Hepatol. 2002. 14:723–731.14. Montgomery A, Ferral H, Vasan R, Postoak DW. MELD score as a predictor of early death in patients undergoing elective transjugular intrahepatic portosystemic shunt (TIPS) procedures. Cardiovasc Intervent Radiol. 2005. 28:307–312.15. Yoon CJ, Chung JW, Park JH. Transjugular intrahepatic portosystemic shunt for acute variceal bleeding in patients with viral liver cirrhosis: predictors of early mortality. AJR Am J Roentgenol. 2005. 185:885–889.16. Schepke M, Roth F, Fimmers R, Brensing KA, Sudhop T, Schild HH, et al. Comparison of MELD, Child-Pugh, and Emory model for the prediction of survival in patients undergoing transjugular intrahepatic portosystemic shunting. Am J Gastroenterol. 2003. 98:1167–1174.17. Angermayr B, Cejna M, Karnel F, Gshwantler M, Koenig F, Pidlich J, et al. Child-Pugh versus MELD score in predicting survival in patients undergoing transjugular intrahepatic portosystemic shunt. Gut. 2003. 52:879–885.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Bleeding from an Ileal Conduit Stomal Varix: Diagnosis with Three-Dimmensional Volume Rendered Images by the use of Multidetector-Row CT (MDCT) and Management with a Transjugular Intrahepatic Portosystemic Shunt
- Gastric Variceal Rebleeding by Aberrant Left Gastric Vein after Transjugular Intrahepatic Portosystemic Shunt: A Case Report
- A Case of Successful Treatment of Stomal Variceal Bleeding with Transjugular Intrahepatic Portosystemic Shunt and Coil Embolization
- A Successful Endoscopic Therapy for Uncontrolled Duodenal Varix after Transjugular Intrahepatic Portosystemic Shunt
- Prognostic Factors of the Long-Term Survival after Transjugular Intrahepatic Portosystemic Shunt in the Treatment of Gastric and Esophageal Variceal Bleeding
