Comparison of CT-Guided Sclerotherapy with Using 95% Ethanol and 20% Hypertonic Saline for Managing Simple Renal Cyst
- Affiliations
-
- 1Department of Radiology, Cumhuriyet University School of Medicine,Sivas, Turkey. hegilmez@cumhuriyet.edu.tr
- 2Department of Obstetrics and Gynecology, Cumhuriyet University School of Medicine,Sivas, Turkey.
- 3Department of Urology, Cumhuriyet University School of Medicine, Sivas, Turkey.
- KMID: 1089439
- DOI: http://doi.org/10.3348/kjr.2007.8.6.512
Abstract
- OBJECTIVE: We wanted to compare the efficacies of 95% ethanol and 20% hypertonic saline (HS) sclerotherapies that were performed in a single session under CT guidance for the management of simple renal cysts. MATERIALS AND METHODS: A prospective series of 74 consecutive patients (average age: 57.6 +/- 8.1 years) with simple renal cysts were enrolled in this study. They were randomized into two groups and 95% ethanol or 20% HS, respectively, corresponding to 25% of the aspiration volume, was injected. Treatment success was determined six months later with follow-up clinical evaluation and performing ultrasonography. RESULTS: The sclerotherapy was accepted as technically successful without major complications in all except two patients who were excluded because of a communication between the simple renal cyst and the pelvicalyceal collecting system. Thirty-six patients in the ethanol group received sclerotherapy with 95% ethanol and 36 patients in the HS group underwent sclerotherapy with 20% HS. The complete regression ratio of the ethanol group was significantly higher (94% versus 72%, respectively) than that of the HS group. There was one patient with partial regression in each group. The failure ratio of the ethanol group was significantly lower (3% versus 25%, respectively) than that of the HS group. CONCLUSION: Ethanol sclerotherapy under CT guidance is a successful and safe procedure and it can be used for the treatment of simple renal cysts. Sclerotherapy with 95% ethanol is more effective than 20% HS sclerotherapy. Sclerotherapy with HS may be an option for patients preferring to undergo a less painful treatment procedure.
MeSH Terms
-
Adult
Aged
Ethanol/administration & dosage/*therapeutic use
Female
Follow-Up Studies
Humans
Kidney/drug effects/radiography/ultrasonography
Kidney Diseases, Cystic/*drug therapy
Male
Middle Aged
Prospective Studies
Saline Solution, Hypertonic/administration & dosage
Sclerosing Solutions/administration & dosage/*therapeutic use
Sclerotherapy/adverse effects/*methods
Tomography, X-Ray Computed/*methods
Treatment Outcome
Figure
-
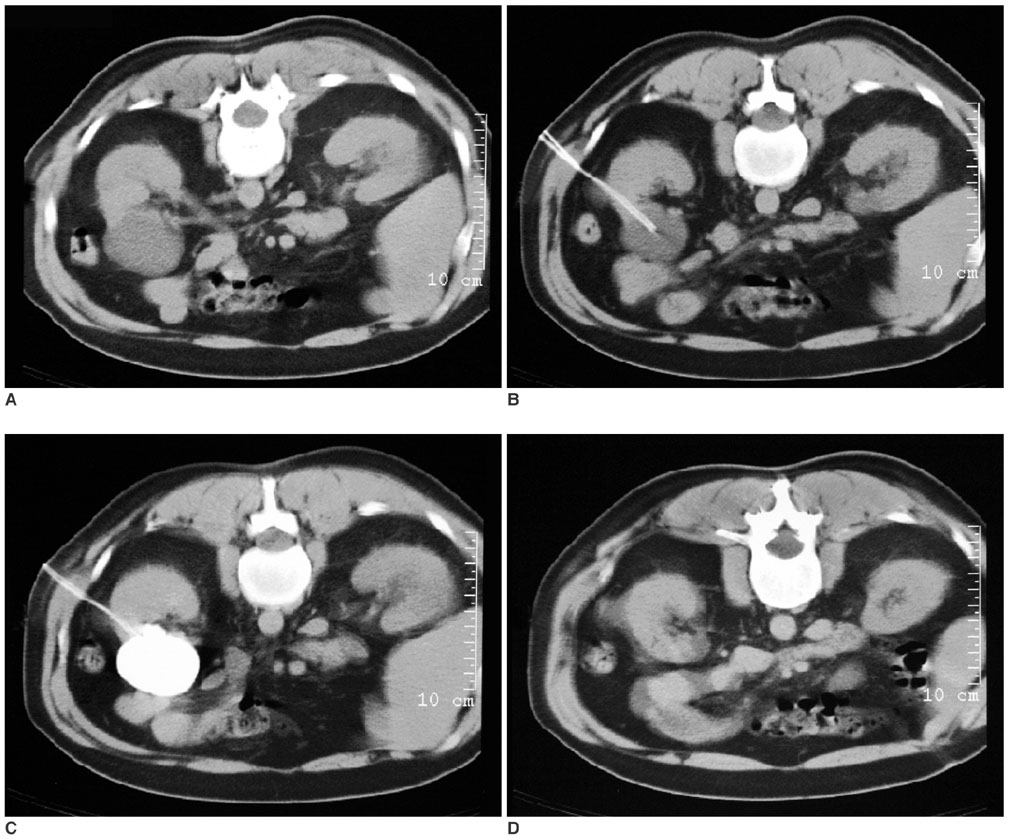
Fig. 1 Representative CT images of a 53-year-old male patient with a simple renal cyst. A. The simple renal cyst before aspiration. B. A 5.4-Fr pigtail catheter was inserted into the cyst. C. Contrast medium is instilled into the cyst to ensure that there was no communication with the pelvicalyceal collecting system, to exclude any leakage from the puncture site into the retroperitoneal cavity and to determine the presence of extravasation. D. The cyst disappeared after successful ethanol sclerotherapy.
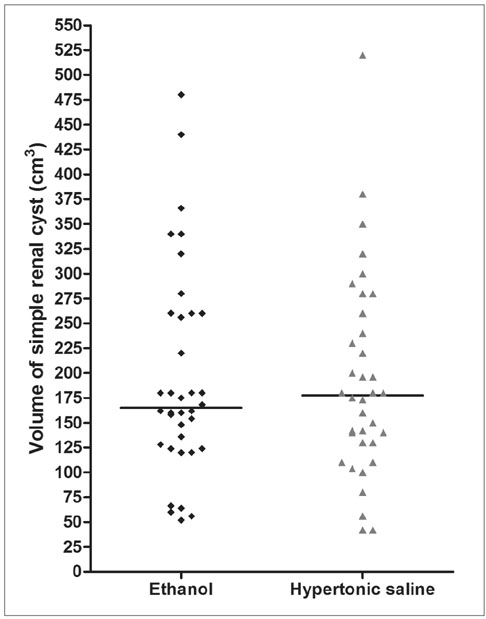
Fig. 2 Scatter dot plot with median line graphics of the volume of the simple renal cysts in the ethanol and hypertonic saline groups. There was no significant difference of the cyst volume between the study groups (p = 0.995).

Fig. 3 The number of patients, with complete and partial regression and failure at six months follow-up after sclerotherapy, in the ethanol and hypertonic saline groups. Their percentages are also presented. aP = 0.024 vs. the complete regression ratio of the hypertonic saline group with using Fisher's exact test. bP = 0.014 vs. the failure ratio of the hypertonic saline group with using Fisher's exact test.
Cited by 1 articles
-
Predictors of the Frequency of Ethanol Injections for Renal Cyst Ablation: A Preliminary Study
Yong Hun Kim, Bum Sang Cho
J Korean Soc Radiol. 2018;78(3):193-199. doi: 10.3348/jksr.2018.78.3.193.
Reference
-
1. Clayman RV, Surya V, Miller RP, Reinke DB, Fraley EE. Pursuit of the renal mass. Is ultrasound enough? Am J Med. 1984. 77:218–223.2. Caglioti A, Esposito C, Fuiano G, Buzio C, Postorino M, Rampino T, et al. Prevalence of symptoms in patients with simple renal cysts. BMJ. 1993. 306:430–431.3. Ravine D, Gibson RN, Donlan J, Sheffield LJ. An ultrasound renal cyst prevalence survey: specificity data for inherited renal cystic diseases. Am J Kidney Dis. 1993. 22:803–807.4. Marumo K, Horiguchi Y, Nakagawa K, Oya M, Ohigashi T, Asakura H, et al. Incidence and growth pattern of simple cysts of the kidney in patients with asymptomatic microscopic hematuria. Int J Urol. 2003. 10:63–67.5. Rockson SG, Stone RA, Gunnells JC Jr. Solitary renal cyst with segmental ischemia and hypertension. J Urol. 1974. 112:550–552.6. Okeke AA, Mitchelmore AE, Keeley FX, Timoney AG. A comparison of aspiration and sclerotherapy with laparoscopic de-roofing in the management of symptomatic simple renal cysts. BJU Int. 2003. 92:610–613.7. el-Diasty TA, Shokeir AA, Tawfeek HA, Mahmoud NA, Nabeeh A, Ghoneim MA. Ethanol sclerotherapy for symptomatic simple renal cysts. J Endourol. 1995. 9:273–276.8. Chung BH, Kim JH, Hong CH, Yang SC, Lee MS. Comparison of single and multiple sessions of percutaneous sclerotherapy for simple renal cyst. BJU Int. 2000. 85:626–627.9. Fontana D, Porpiglia F, Morra I, Destefanis P. Treatment of simple renal cysts by percutaneous drainage with 3 repeated alcohol injection. Urology. 1999. 53:904–907.10. Kim JH, Lee JT, Kim EK, Won JY, Kim MJ, Lee JD, et al. Percutaneous sclerotherapy of renal cysts with a beta-emitting radionuclide, holmium-166-chitosan complex. Korean J Radiol. 2004. 5:128–133.11. Roberts WW, Bluebond-Langner R, Boyle KE, Jarrett TW, Kavoussi LR. Laparoscopic ablation of symptomatic parenchymal and peripelvic renal cysts. Urology. 2001. 58:165–169.12. Falci-Junior R, Lucon AM, Cerri LM, Danilovic A, Da Rocha PC, Arap S. Treatment of simple renal cysts with single-session percutaneous ethanol sclerotherapy without drainage of the sclerosing agent. J Endourol. 2005. 19:834–838.13. Yoder BM, Wolf JS Jr. Long-term outcome of laparoscopic decortication of peripheral and peripelvic renal and adrenal cysts. J Urol. 2004. 171(2 Pt 1):583–587.14. Akinci D, Akhan O, Ozmen M, Gumus B, Ozkan O, Karcaaltincaba M, et al. Long-term results of single-session percutaneous drainage and ethanol sclerotherapy in simple renal cysts. Eur J Radiol. 2005. 54:298–302.15. Lee YR, Lee KB. Ablation of symptomatic cysts using absolute ethanol in 11 patients with autosomal-dominant polycystic kidney disease. Korean J Radiol. 2003. 4:239–242.16. Gasparini D, Sponza M, Valotto C, Marzio A, Luciani LG, Zattoni F. Renal cysts: can percutaneous ehtanol injections be considered an alternative to surgery? Urol Int. 2003. 71:197–200.17. Akhan O, Ozmen MN, Dincer A, Sayek I, Göcmen A. Liver hydatid disease: long-term results of percutaneous treatment. Radiology. 1996. 198:259–264.18. Khuroo MS, Zargar SA, Mahajan R. Echinococcus granulosus cysts in the liver: management with percutaneous drainage. Radiology. 1991. 180:141–145.19. Paksoy Y, Odev K, Sahin M, Arslan A, Koc O. Percutaneous treatment of liver hydatid cysts: comparison of direct injection of albendazole and hypertonic saline solution. AJR Am J Roentgenol. 2005. 185:727–734.20. Harisinghani MG, Gervais D, Hahn PF, Jhaveri K, Yoder I, Mueller PR. CT and MR of atypical cystic renal masses: Revisiting the Bosniak classification. Radiologist. 2001. 8:145–153.21. Warren KS, McFarlane J. The Bosniak classification of renal cystic masses. BJU Int. 2005. 95:939–942.22. Nahm AM, Ritz E. The simple renal cyst. Nephrol Dial Transplant. 2000. 15:1702–1704.23. Curry NS, Bissada NK. Radiologic evaluation of small and indeterminant renal masses. Urol Clin North Am. 1997. 24:493–505.24. Higgins JC, Fitzgerald JM. Evaluation of incidental renal and adrenal masses. Am Fam Physician. 2001. 63:288–294. 29925. Akinci D, Gumus B, Ozkan OS, Ozmen MN, Akhan O. Single-session percutaneous ethanol sclerotherapy in simple renal cysts in children: long-term follow-up. Pediatr Radiol. 2005. 35:155–158.26. Yasuda M, Masai M, Shimazaki J. A simple renal cyst. Nippon Hinyokika Gakkai Zasshi. 1993. 84:251–257.27. Dalton D, Neiman H, Grayhack JT. The natural history of simple renal cysts: a preliminary study. J Urol. 1986. 135:905–908.28. Wolf JS Jr. Evaluation and management of solid and cystic renal masses. J Urol. 1998. 159:1120–1133.29. Camacho MF, Bondhus MJ, Carrion HM, Lockhart JL, Politano VA. Ureteropelvic junction obstruction resulting from percutaneous cyst puncture and intracystic isophendylate injection: an unusual complications. J Urol. 1980. 124:713–714.30. Bean WJ, Rodan BA. Hepatic cysts: treatment with alcohol. AJR Am J Roentgenol. 1985. 144:237–241.31. Goktay AY, Secil M, Gulcu A, Hosgor M, Karaca I, Olguner M, et al. Percutaneous treatment of hydatid liver cysts in children as a primary treatment: long-term results. J Vasc Interv Radiol. 2005. 16:831–839.32. Kabaalioğlu A, Karaali K, Apaydin A, Melikoğlu M, Sindel T, Lüleci E. Ultrasound-guided percutaneous sclerotherapy of hydatid liver cysts in children. Pediatr Surg Int. 2000. 16:346–350.33. Kabaalioğlu A, Apaydin A, Ozkaynak C, Melikoğlu M, Sindel T, Lüleci E. Percutaneous sclerotherapy of a symptomatic simple renal cyst in a child: observation of membrane detachment sign. Eur Radiol. 1996. 6:872–874.34. Lin YH, Pan HB, Liang HL, Chung HM, Chen CY, Huang JS, et al. Single-session alcohol-retention sclerotherapy for simple renal cysts: comparison of 2- and 4-hr retention techniques. AJR Am J Roentgenol. 2005. 185:860–866.35. De Dominicis C, Ciccariello M, Peris F, Di Crosta G, Sciobica F, Zuccalà A, et al. Percutaneous sclerotization of simple renal cysts with 95% ethanol followed by 24-48 h drainage with nephrostomy tube. Urol Int. 2001. 66:18–21.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Aspiration and Sclerotherapy with 95% Ehtanol for Simple Renal Cyst
- Ultrasound-guided Aspiration and Instillation of 95% Ethanol for Simple Renal Cyst
- Effect of Percutaneous Aspiration and Repeated Sclerotherapy of the Simple Renal Cyst
- The Effect of Two-Injection Ethanol Sclerotherapy with 5-Minute Duration of Exposure Time in Simple Renal Cysts
- Long Term Follow-up Results of Percutaneous Aspiration with Sclerotherapy of the Simple Renal Cyst
