Fibroblastic Type Osteosarcoma of the Ulna: a Case Report of a Tumor in a Rare Location with Atypical Imaging Findings
- Affiliations
-
- 1Department of Radiology and Institute of Radiation Medicine, Seoul National University College of Medicine, Seoul, Korea. jacrad@radiol.snu.ac.kr
- 2Department of Radiology, Seoul National University Bundang Hospital, Seong Nam, Gyeongi-do, Korea.
- 3Department of Pathology, Seoul National University Bundang Hospital, Seong Nam, Gyeongi-do, Korea.
- 4Department of Orthopedic Surgery, Seoul National University Bundang Hospital, Seong Nam, Gyeongi-do, Korea.
- KMID: 1088683
- DOI: http://doi.org/10.3348/kjr.2009.10.1.85
Abstract
- The ulna is a rare site of origin for osteosarcoma, and purely osteolytic osteosarcomas are uncommonly noted on conventional radiographs. We present a patient with a lytic lesion of the distal ulna for which imaging findings suggested an aneurysmal bone cyst. The lesion was histologically confirmed to be a fibroblastic osteosarcoma.
MeSH Terms
Figure
-
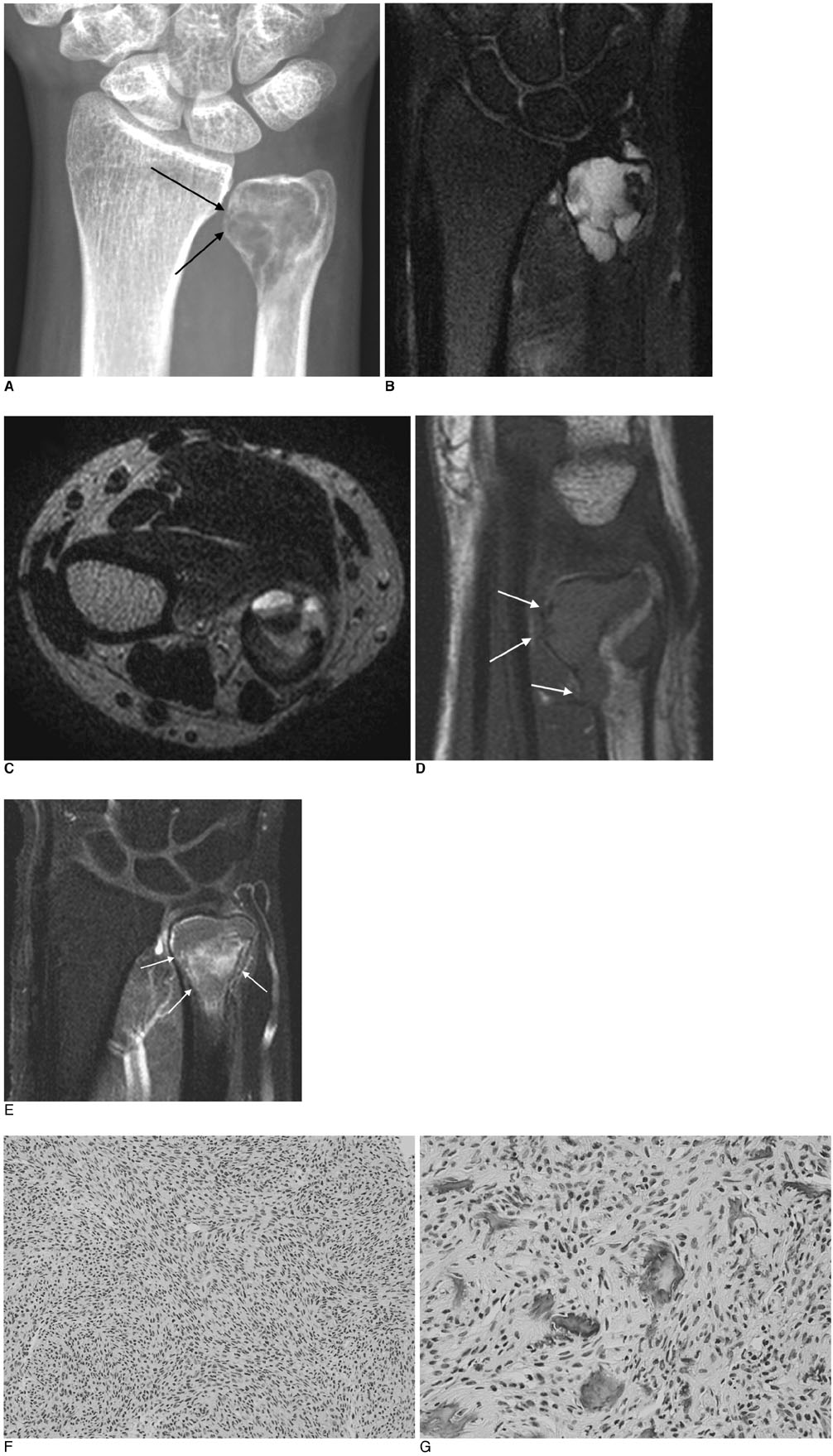
Fig. 1 Imaging findings of fibroblastic osteosarcoma in distal ulna of 37-year-old woman. A. PA view of right wrist reveals well-marginated osteolytic lesion of slightly expansile nature with suspicious focal cortical disruptions (arrows) in distal ulna metaphysis and epiphysis. B. Coronal T2-weighted (TR/TE = 2925/54), fat-suppressed MR imaging shows multi-loculated, high signal intensity lesion in distal ulna. C. Axial T2-weighted (TR/TE = 4319/100) MR imaging shows fluid-fluid levels within cystic lesion. D. Sagittal T1-weighted (400/18.46) MR imaging reveals cortical disruptions (white arrows). E. On gadolinium-enhanced, fat-suppressed, T1-weighted (517.9/20) MR imaging, focal enhancement of lesion (white arrows) is noted along with largely non-enhancing portions. F. Large part of tumor is composed of spindle cells, often in "herringbone" pattern (Hematoxylin & Eosin staining, ×200). G. Focal osteoid production by neoplastic stromal cells (Hematoxylin & Eosin staining, ×400).
Cited by 1 articles
-
Lesions that Mimic Musculoskeletal Infection: A Pictorial Essay
Hye Jin Kang, Hee Young Choi, Ji Seon Park, So Young Park, Wook Jin, Kyung Nam Ryu
J Korean Soc Radiol. 2018;78(3):200-211. doi: 10.3348/jksr.2018.78.3.200.
Reference
-
1. Murphey MD, Robbin MR, McRae GA, Flemming DJ, Temple HT, Kransdorf MJ. The many faces of osteosarcoma. Radiographics. 1997. 17:1205–1231.2. Exner GU, von Hochstetter AR, Honegger H, Schreiber A. Osseous lesions of the distal ulna: atypical location-unusual diagnosis Report of three cases with similar imaging and different pathologic diagnoses. Arch Orthop Trauma Surg. 2000. 120:219–223.3. Sundaram M, Totty WG, Kyriakos M, McDonald DJ, Merkel K. Imaging findings in pseudocystic osteosarcoma. AJR Am J Roentgenol. 2001. 176:783–788.4. Mahnken AH, Nolte-Ernsting CC, Wildberger JE, Heussen N, Adam G, Wirtz DC, et al. Aneurysmal bone cyst: value of MR imaging and conventional radiography. Eur Radiol. 2003. 13:1118–1124.5. Resnick D, Kransdorf MJ. Bone and joint imaging. 2005. 3rd ed. Philadelphia: Saunders.6. Maccauro G, Tulli A, Prezioso V, Muratori F, Della Rocca C, Barone C. Parosteal osteosarcoma of the ulna: a rare low-grade malignant neoplasm. Case report and review of the literature. J Orthopaed Traumatol. 2006. 7:198–120.7. Arndt CA, Crist WM. Common musculoskeletal tumors of childhood and adolescence. N Engl J Med. 1999. 341:342–352.8. deSantos LA, Edeiken B. Purely lytic osteosarcoma. Skeletal Radiol. 1982. 9:1–7.9. Phatak SV, Ravi R, Kolwadkar PK, Rajderkar D. Diaphyseal osteosarcoma: - a case report. Indian J Radiol Imaging. 2006. 16:335–337.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Rosette-forming epithelioid osteosarcoma in the rib: a rare case of location and morphology
- Metachronous osteosarcoma
- Radiographic manifestations of fibroblastic osteosarcoma: A diagnostic challenge
- A Case of Pleomorphic Dermal Sarcoma Showing Characteristics of Myxoinflammatory Fibroblastic Sarcoma
- A small cell osteosarcoma on the calcaneus: a case report
