Imaging Features of Adult Choledochal Cysts: a Pictorial Review
- Affiliations
-
- 1Department of Radiology, College of Medicine, Soonchunhyang University Bucheon Hospital, Gyunggi-do, Korea. hklee@schbc.ac.kr
- 2Department of Gastroenterology, College of Medicine, Soonchunhyang University Bucheon Hospital, Gyunggi-do, Korea.
- 3Department of Radiology, College of Medicine, Soonchunhyang University Seoul Hospital, Seoul, Korea.
- KMID: 1088681
- DOI: http://doi.org/10.3348/kjr.2009.10.1.71
Abstract
- Choledochal cysts are rare congenital anomalies which are principally diagnosed by disproportional dilatation of the extrahepatic bile ducts. In addition, choledochal cysts are believed to arise from the anomalous union of the common bile duct and pancreatic duct outside the duodenal wall which is also proximal to the sphincter of the Oddi mechanism. The various types of choledochal cysts have been classified on the basis of these anomalous unions (Komi classification) and their anatomical locations (Todani classification). The multidetector computed tomography with reformatted imaging, magnetic resonance cholangiopancreatography, and an endoscopic retrograde cholangiography represent the important techniques providing the anatomical resolution and detail required to properly diagnose and classify choledochal cysts and their associated abnormal features of the biliary tree, as well as their pancreaticobile duct union. This study describes the various imaging features of a choledochal cyst in adults according to the various types of anomalous unions of the pancreaticobile duct according to Komi's classification and anatomic location according to Todani's classification. Lastly, we also review and discuss the associated abnormal findings developed in biliary systems.
Keyword
MeSH Terms
Figure
-
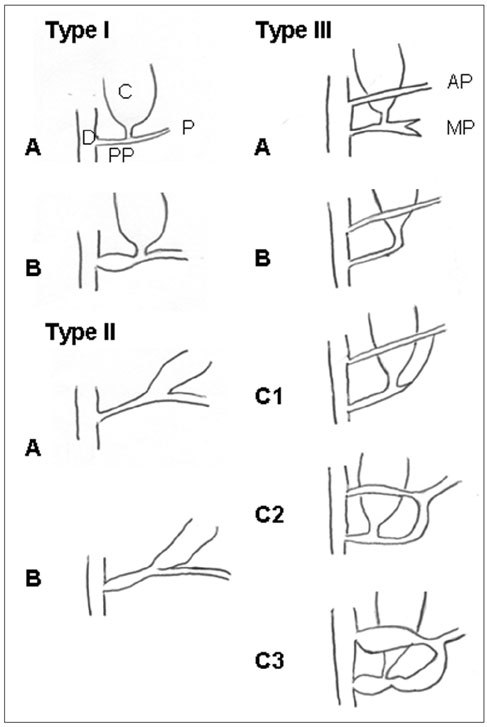
Fig. 1 Classification of anomalous union of pancreaticobile duct as per Komi et al. (11). AP = accessory pancreatic duct, C = choledochal cyst, CC = common channel, D = duodenum, MP = main pancreatic duct, P = pancreatic duct
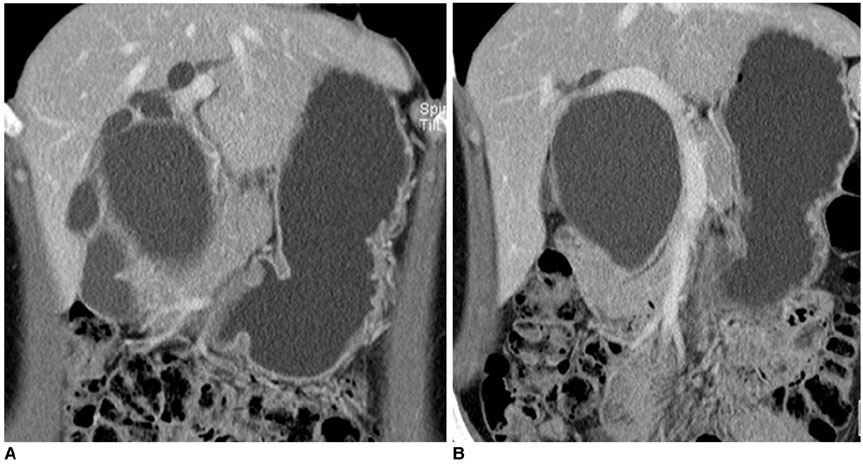
Fig. 2 Choledochal cyst with anomalous union of pancreaticobile duct (Komi IA, Todani IVA). A, B. Coronal reformatted CT scans show cystic dilatation of common bile duct with segmental dilatation of proximal intrahepatic duct and abrupt narrowing at distal end. Distal common bile duct joined with pancreatic duct at right angle.
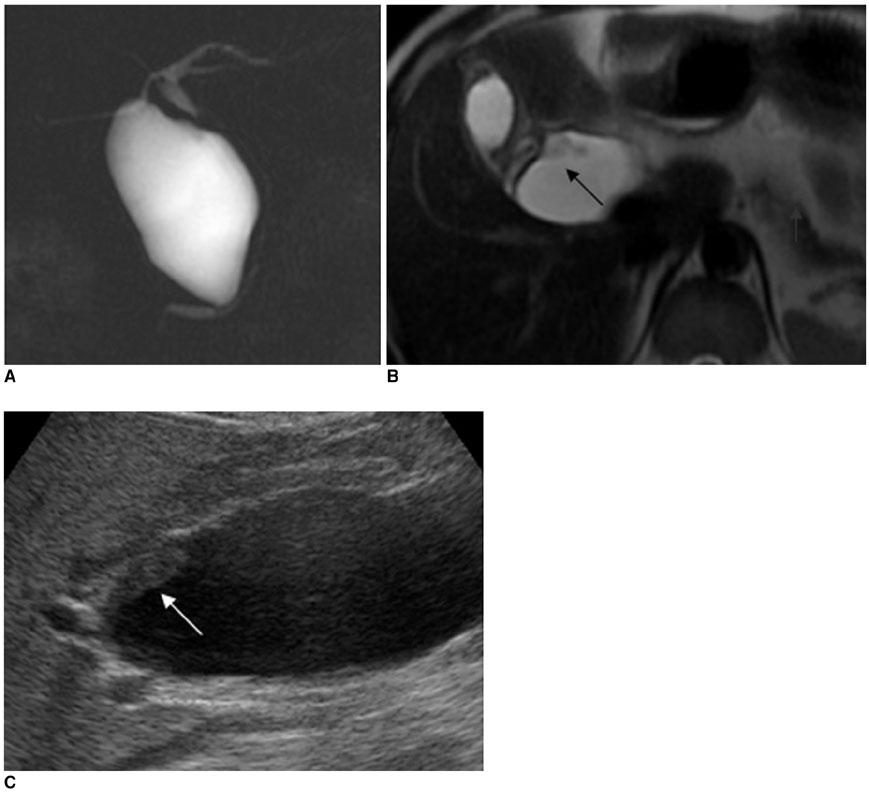
Fig. 3 Choledochal cyst with anomalous union of pancreaticobile duct (Komi IA, Todani IA) combined cholangiocarcinoma. A-C. MR cholangiopancreatography (A) images show cystic dilatation of common bile duct, with abrupt narrowing at distal end which joined with pancreatic duct at right angle. T2W transverse image of MR cholangiopancreatography (B) and ultrasonography (C) images show polypoid mass (arrows) at proximal region of cyst, which was confirmed pathologically as cholangiocarcinoma after operation.
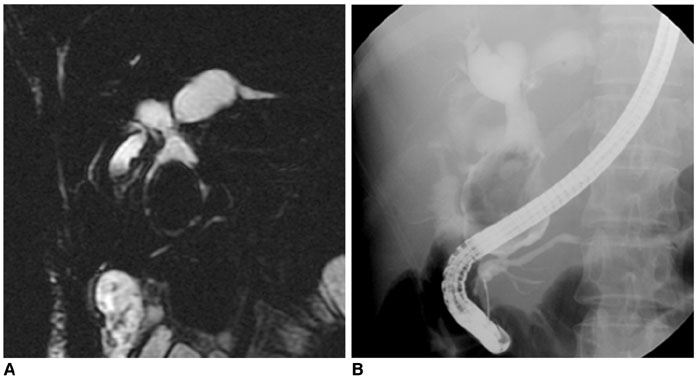
Fig. 4 Choledochal cyst with anomalous union of pancreaticobile duct (Komi IB, Todani IVA) combined stone. A, B. MR cholangiopancreatography (A) and endoscopic retrograde cholangiopancreatography (B) images show saccular dilatation of intrahepatic duct and common bile duct, which joined with pancreatic duct at right angle. Cyst also showed large filling defect in common bile duct. Common channel is dilated on endoscopic retrograde cholangiopancreatography (B) image.
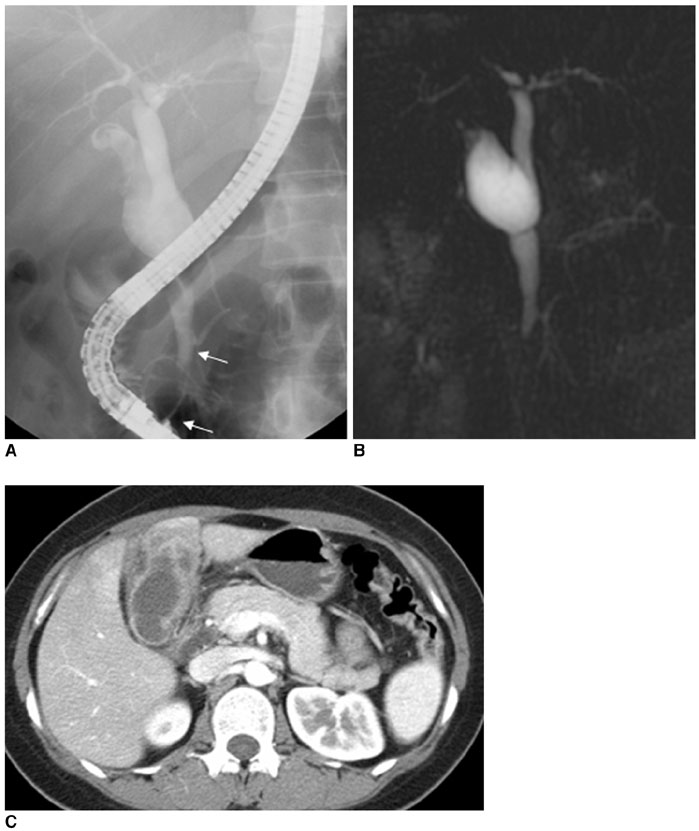
Fig. 5 Choledochal cyst with anomalous union of pancreaticobile duct (Komi IIA, Todani IB) combined small cell cancer of gallbladder. A-C. Endoscopic retrograde cholangiopancreatography (A) and MR cholangiopancreatography (B) images show fusiform dilatation of common bile duct, joined with pancreatic duct at acute angle, along with long common channel (arrows, 24 mm) and low lying cystic duct insertion with dilatation in proximal region. Irregular filling defect is noted in contrast filled gallbladder on endoscopic retrograde cholangiopancreatography image. CT image (C) shows irregular enhancing wall thickening of gallbladder. Pathologic diagnosis was confirmed to be small cell carcinoma.
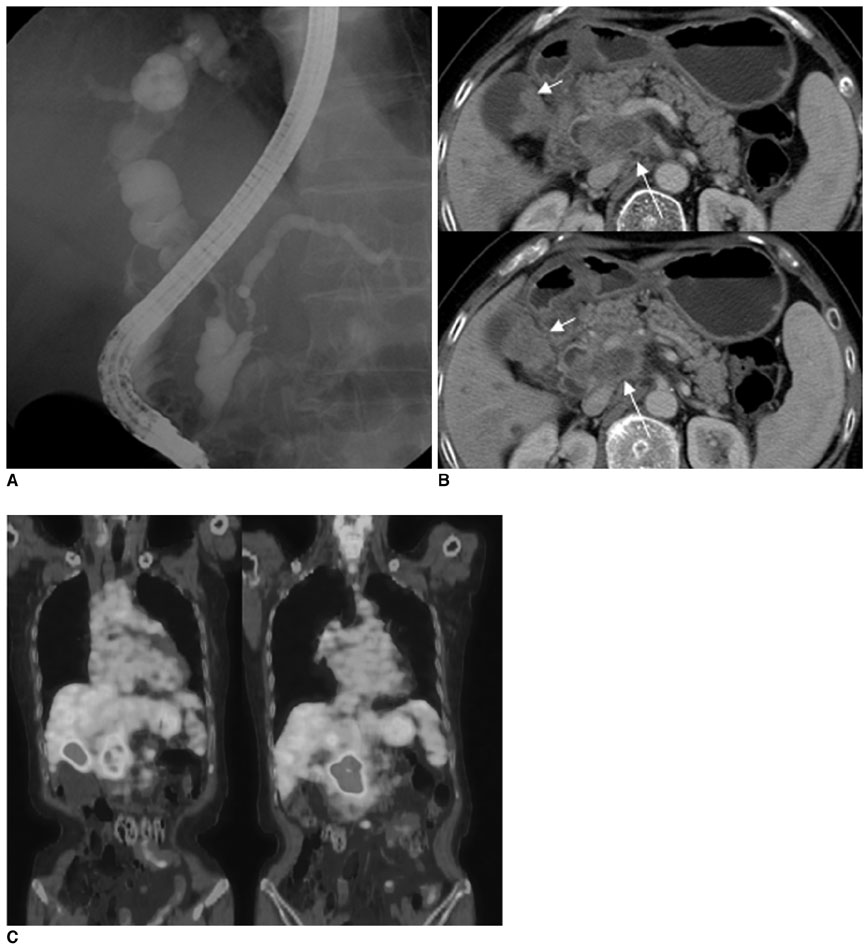
Fig. 6 Choledochal cyst with anomalous union of pancreaticobile duct (Komi IIB, Todani IVA) combined gallbladder and common bile duct cancer. A-C. Endoscopic retrograde cholangiopancreatography (A) image shows irregularly dilated common bile duct, common hepatic duct and intrahepatic duct. Common bile duct is joined with pancreatic duct at acute angle. In addition, long common channel is dilated. CT (B) image shows irregular enhancing mass in gallbladder (short arrows) and common bile duct (long arrows). PET CT (C) show focal increased FDG uptake as seen in gallbladder and common bile duct region.
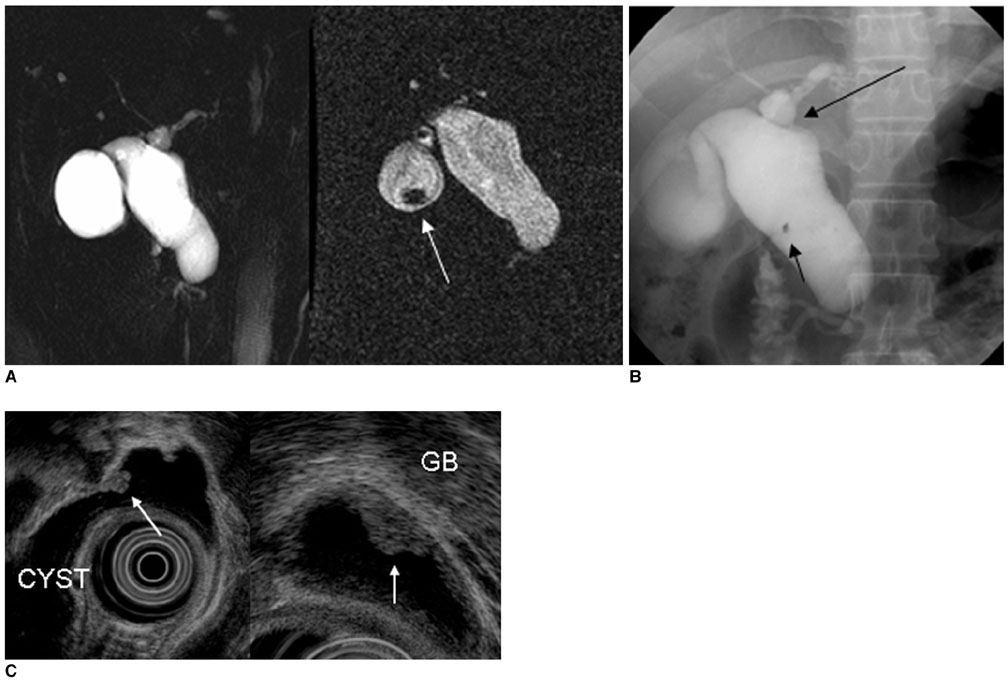
Fig. 7 Choledochal cyst and anomalous union of pancreaticobile duct (Komi IIIC2, Todani IC) combined with gallbladder cancer. A-C. MR cholangiopancreatography (A) and endoscopic retrograde cholangiopancreatography (B) images show saccular dilatation of common hepatic duct, common bile duct, left intrahepatic duct and cystic duct. Stricture is noted at hilum (black long arrows) on endoscopic retrograde cholangiopancreatography image. There is mass in gallbladder (white arrow) and small filling defect in cyst (short black arrow). Anomalous union of pancreaticobile duct with patent accessory duct is noted and common channel with same caliber of main and accessory duct. On endoscopic US (C), small polypoid mass in choledochal cyst and broad based villous isoechogenic mass in gallbladder. After operation, gallbladder cancer is confirmed, but there is no evidence of mass in choledochal cyst.
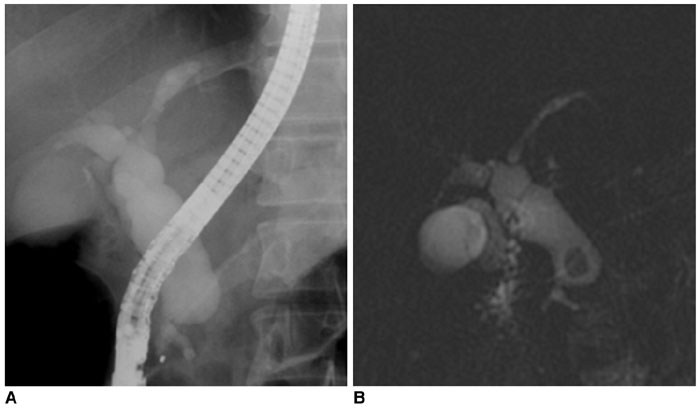
Fig. 8 Choledochal cyst with anomalous union of pancreaticobile duct (Komi IIIC3, Todani IA) combined stone. A, B. Endoscopic retrograde cholangiopancreatography (A) and MR cholangiopancreatography (B) images show fusiform dilatation of common bile duct, common hepatic duct, and both intrahepatic ducts. Accessory pancreatic duct is united with main pancreatic duct and common channel is dilated. Round filling defect is noted in distal common bile duct.
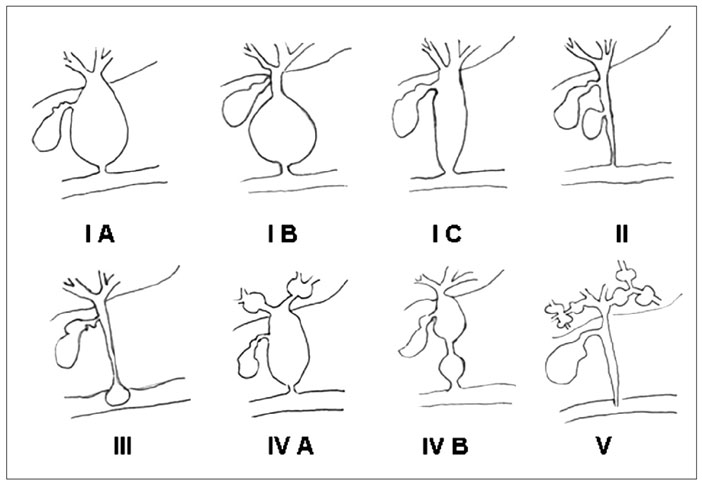
Fig. 9 Choledochal cyst was described according to Todani's classification system (12).
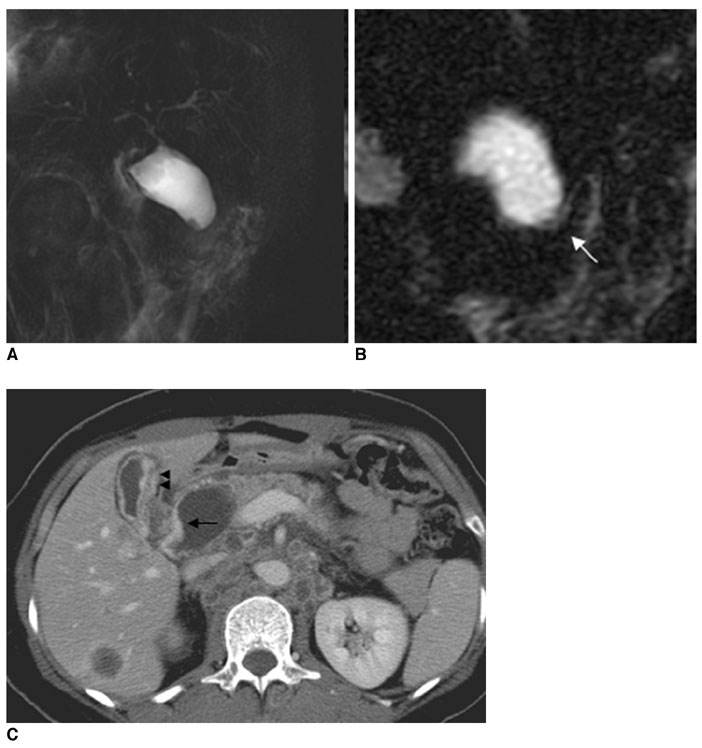
Fig. 10 Choledochal cyst with anomalous union of pancreaticobile duct (Komi IA, Todani IC) combined cholangiocarcinoma and gallbladder cancer with liver metastasis. A-C. MR cholangiopancreatography images (A, B) show cystic dilatation of common bile duct, however, proximal common hepatic duct and intrahepatic duct show normal caliber. Additionally, common bile duct joined with pancreatic duct at right angle (arrow). CT image (C) shows saccular dilatation of common bile duct with enhancing wall thickening in proximal region of choledochal cyst (arrow) and gallbladder (arrowheads). In addition, metastatic lesions are present in liver and conglomerated lymph nodes at aortocaval and left paraaortic regions.
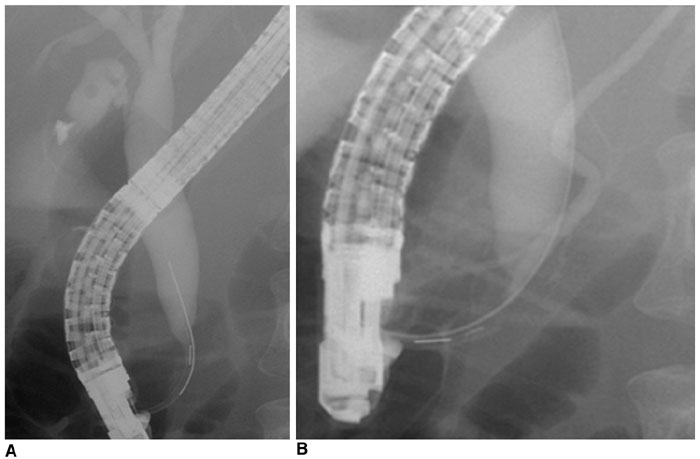
Fig. 11 Choledochal cyst without anomalous union of pancreaticobile duct. A, B. Endoscopic retrograde cholangiopancreatography images (A, B) show fusiform dilatation of common bile duct. There is normal union of common bile duct and pancreatic duct with less than 12 mm of common channel.
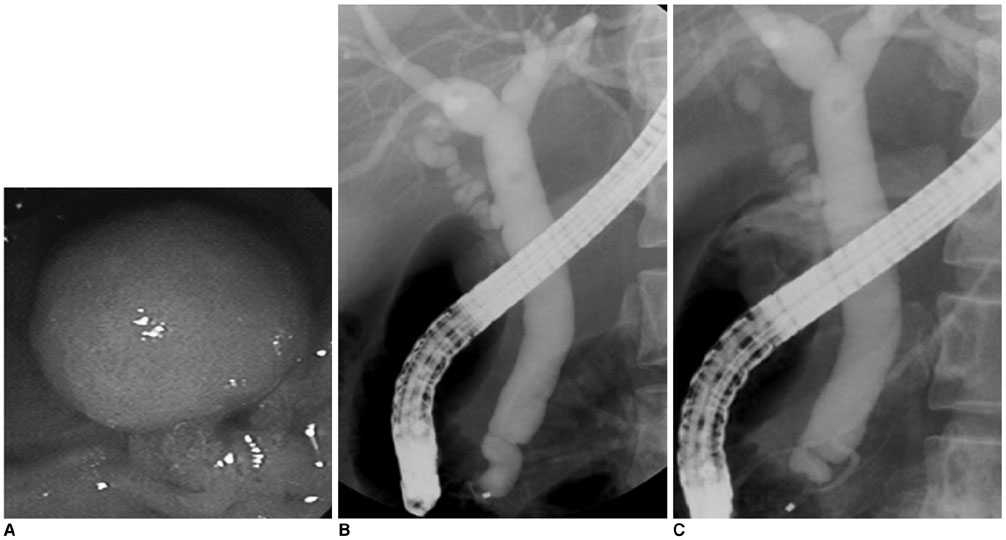
Fig. 12 Choledochocele (Todani III). A-C. Endoscopic retrograde cholangiopancreatography image revealed that duodenal papilla is bulging. Distal common bile duct shows saccular dilatation and collapsing during procedure.
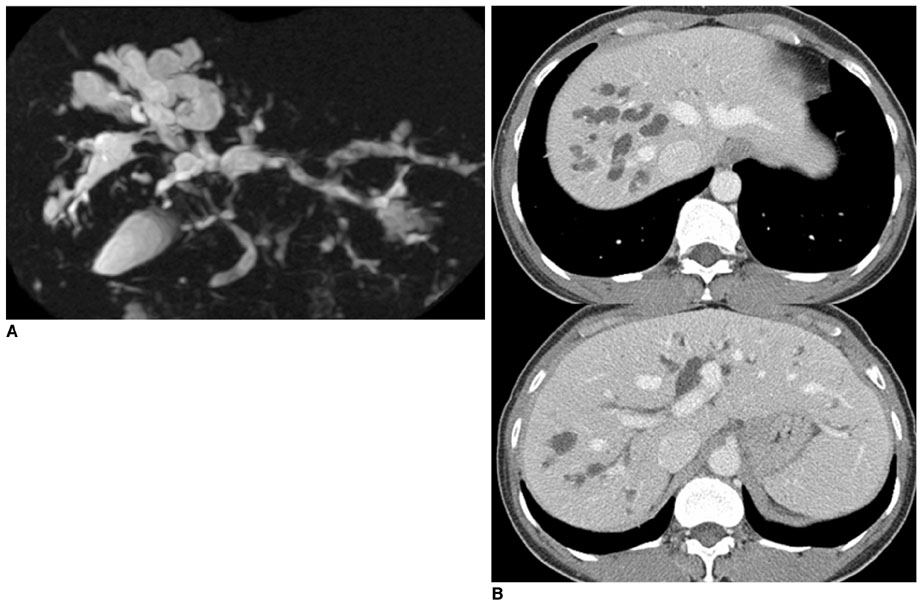
Fig. 13 Calori's disease (Todani V). A, B. MR cholangiopancreatography (A) image shows multifocal irregular dilatation of intrahepatic duct without common bile duct dilatation. CT (B) image revealed multiple cystic dilatation of intrahepatic duct in both lobes of liver, as well as dot-like enhancing foci representing portal radicles adjacent to dilated intrahepatic duct.
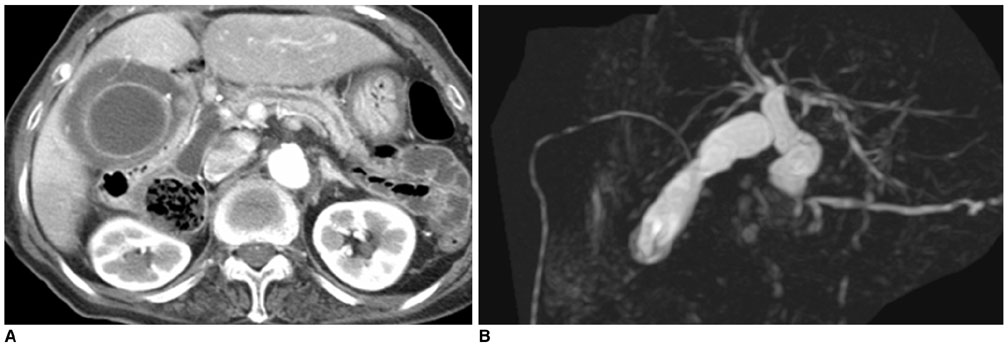
Fig. 14 Choledochal cyst with anomalous union of pancreaticobile duct (Komi IA, Todani IC) combined cholecystitis. A, B. Initial CT (A) image shows diffuse wall thickening with distension of gallbladder, suggesting acute cholecystitis. MR cholangiopancreatography (B) image shows fusiform dilatation of common bile duct, joined with pancreatic duct at right angle.
Reference
-
1. Wiseman K, Buczkowski AK, Chung SW, Francoeur J, Schaeffer D, Scudamore CH. Epidemiology, presentation, diagnosis, and outcomes of choledochal cysts in adults in an urban environment. Am J Surg. 2005. 189:527–531.2. Liu CL, Fan ST, Lo CM, Lam CM, Poon RT, Wang J. Choledochal cysts in adults. Arch Surg. 2002. 137:465–468.3. Visser BC, Suh I, Way LW, Kang SM. Congenital choledochal cysts in adults. Arch Surg. 2004. 139:855–862.4. Liu YB, Wang JW, Devkota KR, Ji ZL, Li JT, Wang XA, et al. Congenital choleochal cysts in adults: twenty-five-year experience. Chin Med J. 2007. 120:1404–1407.5. Park DH, Kim MH, Lee SK, Lee SS, Choi JS, Lee YS, et al. Can MRCP replace the diagnostic role of ERCP for patients with choledochal cysts? Gastrointest Endosc. 2005. 62:360–366.6. Sugiyama M, Haradome H, Takahara T, Abe N, Tokuhara M, Masaki T, et al. Anomalous pancreaticobiliary junction shown on multidetector CT. AJR Am J Roentgenol. 2003. 180:173–175.7. Sugiyama M, Atomi Y. Endoscopic ultrasonography for diagnosing anomalous pancreaticobiliary junction. Gastrointest Endosc. 1997. 45:261–267.8. Babbitt DP, Starshak RJ, Clemett AR. Choledochal cysts: a concept of etiology. Am J Roentgenol Radium Ther Nucl Med. 1973. 119:57–62.9. Iwai N, Yanagihara J, Tokiwa K, Shimotake T, Nakamura K. Congenital choledochal dilatation with emphasis on pathophysiology of the biliary tract. Ann Surg. 1992. 215:27–30.10. Metcalfe MS, Wemyss-Holden SA, Maddern GJ. Management dilemmas with choledochal cysts. Arch Surg. 2003. 138:333–339.11. Komi N, Takehara H, Kunitomo K, Miyoshi Y, Yagi T. Does the type of anomalous arrangement of pancreaticobiliary ducts influence the surgery and prognosis of choledochal cyst? J Pediat Surg. 1992. 27:728–731.12. Todani T, Watanabe Y, Narusue M, Tabuchi K, Okajima K. Congenital bile duct cysts: classification, operative procedures, and review of thirty-seven cases including cancer arising from choledochal cyst. Am J Surg. 1997. 134:263–269.13. Todani T, Watanabe Y, Toki A, Morotomi Y. Classification of congenital biliary cystic disease: special reference to type Ic and IVA cysts with primary ductal stricture. J Hepatobiliary Pancreat Surg. 2003. 10:340–344.14. Fieber SS, Nance FC. Choledochal cyst and neoplasm: a comprehensive review of 106 cases and presentation of two original cases. Am Surg. 1997. 63:982–987.15. Elnemr A, Ohta T, Kayahara M, Kitagawa H, Yoshimoto K, Tani T, et al. Anomalous pancreaticobiliary ductal junction without bile duct dilatation in gallbladder cancer. Hepatogastroenterology. 2001. 48:382–386.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Anomalous junction of pancreaticobiliary ductal system(AJPBDS) in adult choledochal cysts
- Choledochal Cyst Associated with Cystic Duct Dilatation: Report of Three Cases
- Infantile Type Choledochal Cyst with Biliary Atresia: Report of two cases
- A Case Report of Choledochal Cyst
- A Case of Rupture of Choledochal Cyst during Pregnancy
