Sequential Magnetic Resonance Imaging Finding of Intramedullary Spinal Cord Abscess including Diffusion Weighted Image: a Case Report
- Affiliations
-
- 1Department of Radiology, Chungbuk National University College of Medicine, Chungbuk 361-711, Korea. lsyrad@chungbuk.ac.kr
- KMID: 1088570
- DOI: http://doi.org/10.3348/kjr.2011.12.2.241
Abstract
- Intramedullary spinal cord abscess (ISCA) is a rare infection of the central nervous system. We describe the magnetic resonance imaging (MRI) findings, including the diffusion-weighted imaging (DWI) findings, of ISCA in a 78-year-old man. The initial conventional MRI of the thoracic spine demonstrated a subtle enhancing nodule accompanied by significant edema. On the follow-up MRI after seven days, the nodule appeared as a ring-enhancing nodule. The non-enhancing central portion of the nodule appeared hyperintense on DWI with a decreased apparent diffusion coefficient (ADC) value on the ADC map. We performed myelotomy and surgical drainage, and thick, yellowish pus was drained.
MeSH Terms
Figure
-
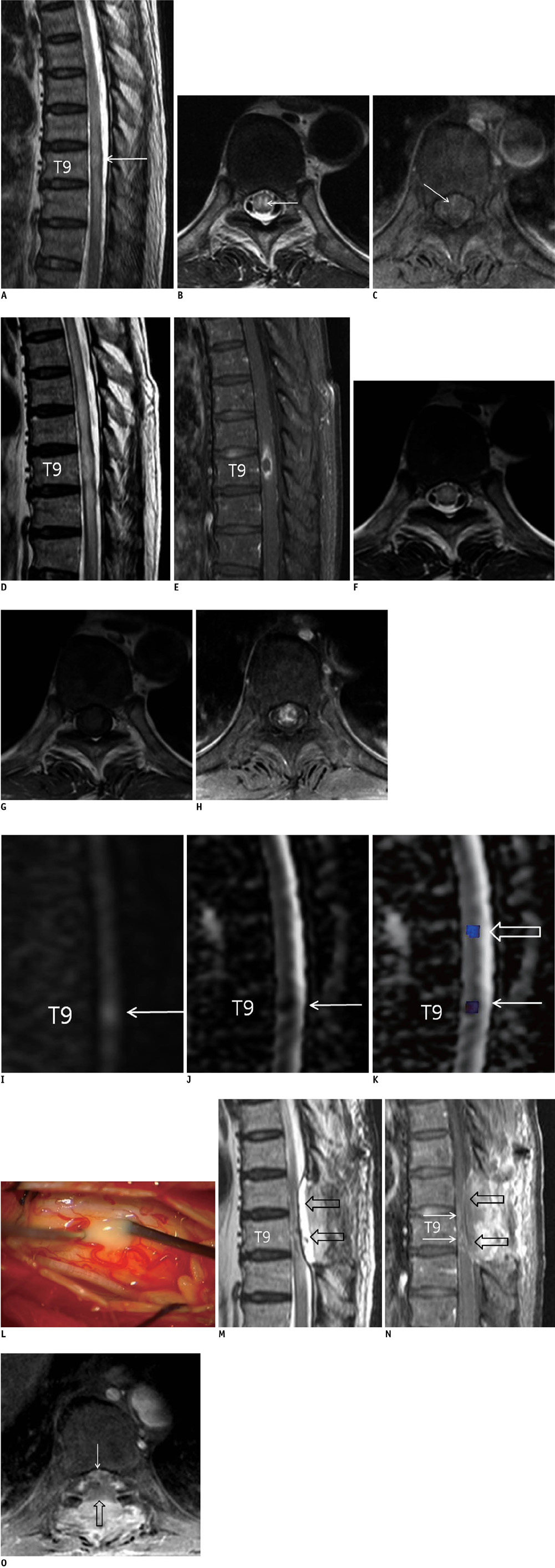
Fig. 1 Intramedullary spinal cord abscess in 78-year-old man. A-C. Initial MRI of thoracic spine shows focal hyperintense nodular lesion involving gray matter at level of T9 (arrows) and diffuse intramedullary high signal intensity extending from T7 to T11 on sagittal (A) and axial (B) T2-weighted images. Axial fat-saturated T1-weighted image with gadolinium (C) at level of T9 shows focal spotty intramedullary enhancement (arrow in C). D-H. Follow-up MRI of thoracic spine that was performed 10 days after initial presentation shows more prominent focal hyperintense lesion at T9 level and increased extent of intramedullary hypersignal intensity, and this all suggested edema from T5 to T11 on sagittal (D) and axial (F) T2-weighted images. Fat-saturated sagittal T1-weighted image after gadolinium injection (E) shows intramedullary ring-enhancing lesion at T9 level. Precontrast (G) and postcontrast (H) axial T1-weighted MRI at T9 level show striking intramedullary enhancement. I. Sagittal diffusion-weighted imaging shows intramedullary hyperintensity at T9 level (arrow). J. Sagittal apparent diffusion coefficient map shows restricted apparent diffusion coefficient map at T9 level (arrow). K. Apparent diffusion coefficient map with region of interest shows each apparent diffusion coefficient value in abscess cavity, surrounding edema and normal spinal cord. Apparent diffusion coefficient within region of interest measured 0.610 × 10-3 mm2/s in abscess cavity (arrow), 1.306 × 10-3 mm2/s in surrounding edema (open arrow) and 1.112 × 10-3 mm2/s in normal-appearing spinal cord (not shown). L. Intraoperative photograph shows yellowish pus after myelotomy at T8-9 level. M-O. Follow-up MRI of thoracic spine performed two weeks after surgical treatment shows markedly improved intramedullary signal change and spinal cord swelling on sagittal (M) T2-weighted images and at-saturated postcontrast sagittal (N) and axial (O) T1-weighted images. But there was residual increased intramedullary signal intensity and contrast enhancement (arrows) at T9-10 level. Postoperative epidural fluid collection (open arrows) and ill-defined enhancement at posterior paraspinal area from T8 to T10 level were also noted.
Reference
-
1. Dörflinger-Hejlek E, Kirsch EC, Reiter H, Opravil M, Kaim AH. Diffusion-weighted MR imaging of intramedullary spinal cord abscess. AJNR Am J Neuroradiol. 2009. 31:1651–1652.2. Hart J. Case of encysted abscess in the center of the spinal cord. Dublin Hospital Report. 1830. 5:522–524.3. Kurita N, Sakurai Y, Taniguchi M, Terao T, Takahashi H, Mannen T. Intramedullary spinal cord abscess treated with antibiotic therapy-case report and review. Neurol Med Chir (Tokyo). 2009. 49:262–268.4. Chan CT, Gold WL. Intramedullary abscess of the spinal cord in the antibiotic era: clinical features, microbial etiologies, trends in pathogenesis, and outcomes. Clin Infect Dis. 1998. 27:619–626.5. Al Barbarawi M, Khriesat W, Qudsieh S, Qudsieh H, Loai AA. Management of intramedullary spinal cord abscess: experience with four cases, pathophysiology and outcomes. Eur Spine J. 2009. 18:710–717.6. Hung PC, Wang HS, Wu CT, Lui TN, Wong AM. Spinal intramedullary abscess with an epidermoid secondary to a dermal sinus. Pediatr Neurol. 2007. 37:144–147.7. Clauss HE, Lorber B. Central nervous system infection with Listeria monocytogenes. Curr Infect Dis Rep. 2008. 10:300–306.8. Reiche W, Schuchardt V, Hagen T, Il'yasov KA, Billmann P, Weber J. Differential diagnosis of intracranial ring enhancing cystic mass lesions--role of diffusion-weighted imaging (DWI) and diffusion-tensor imaging (DTI). Clin Neurol Neurosurg. 2010. 112:218–225.9. Marcel C, Kremer S, Jeantroux J, Blanc F, Dietemann JL, De Sèze J. Diffusion-weighted imaging in noncompressive myelopathies: a 33-patient prospective study. J Neurol. 2010. 257:1438–1445.10. Cartes-Zumelzu FW, Stavrou I, Castillo M, Eisenhuber E, Knosp E, Thurnher MM. Diffusion-weighted imaging in the assessment of brain abscesses therapy. AJNR Am J Neuroradiol. 2004. 25:1310–1317.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Spinal Cord Infarction Associated with Coronavirus Disease 2019: A Case Report with Magnetic Resonance Imaging Insights
- MR Imaging of Anoperineal Tuberculous Abscess: A Case Report
- Intramedullary Spinal Cord Metastasis
- Acute Spinal Cord Infarction: Diffusion-Weighted MR Imaging: Case Report
- Diffusion Tensor Imaging in Inflammatory and Neoplastic Intramedullary Spinal Cord Lesions: Focusing on Fiber Tracking
