Discrepant Immunophenotypic Characteristics between the Lymph Node and Bone Marrow in Two Mixed-Phenotype Acute Leukemia Patients
- Affiliations
-
- 1Department of Laboratory Medicine & Genetics, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea. sunnyhk@skku.edu
- 2Department of Diagnostic Pathology, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea.
- KMID: 1077414
- DOI: http://doi.org/10.3343/kjlm.2009.29.5.396
Abstract
- The immunophenotypic profile of hematological malignancies is usually consistent among different sites of involvement; this consistency allows reliable diagnosis from peripheral blood, bone marrow, or lymph node, especially in cases of acute leukemia. Although in a minority of lymphoma patients, two or more different populations with discordant immunophenotypes have been described, either at the same or distinct sites. Here, we report two Korean patients with acute leukemia where the results of immunophenotypic analysis of the bone marrow specimen were different from those of immunohistochemical studies of a biopsy sample of a cervical lymph node, particularly with respect to myeloperoxidase and CD3. The clinical significance of the immunophenotypic disparity found in the patients still remains unknown; however, discrepancies between the different anatomic sites that are simultaneously involved can occur in a subset of leukemia patients. Therefore, integration of all the relevant results, including those of the bone marrow studies, may be helpful for accurate diagnosis and selecting appropriate treatment modalities.
MeSH Terms
Figure
-
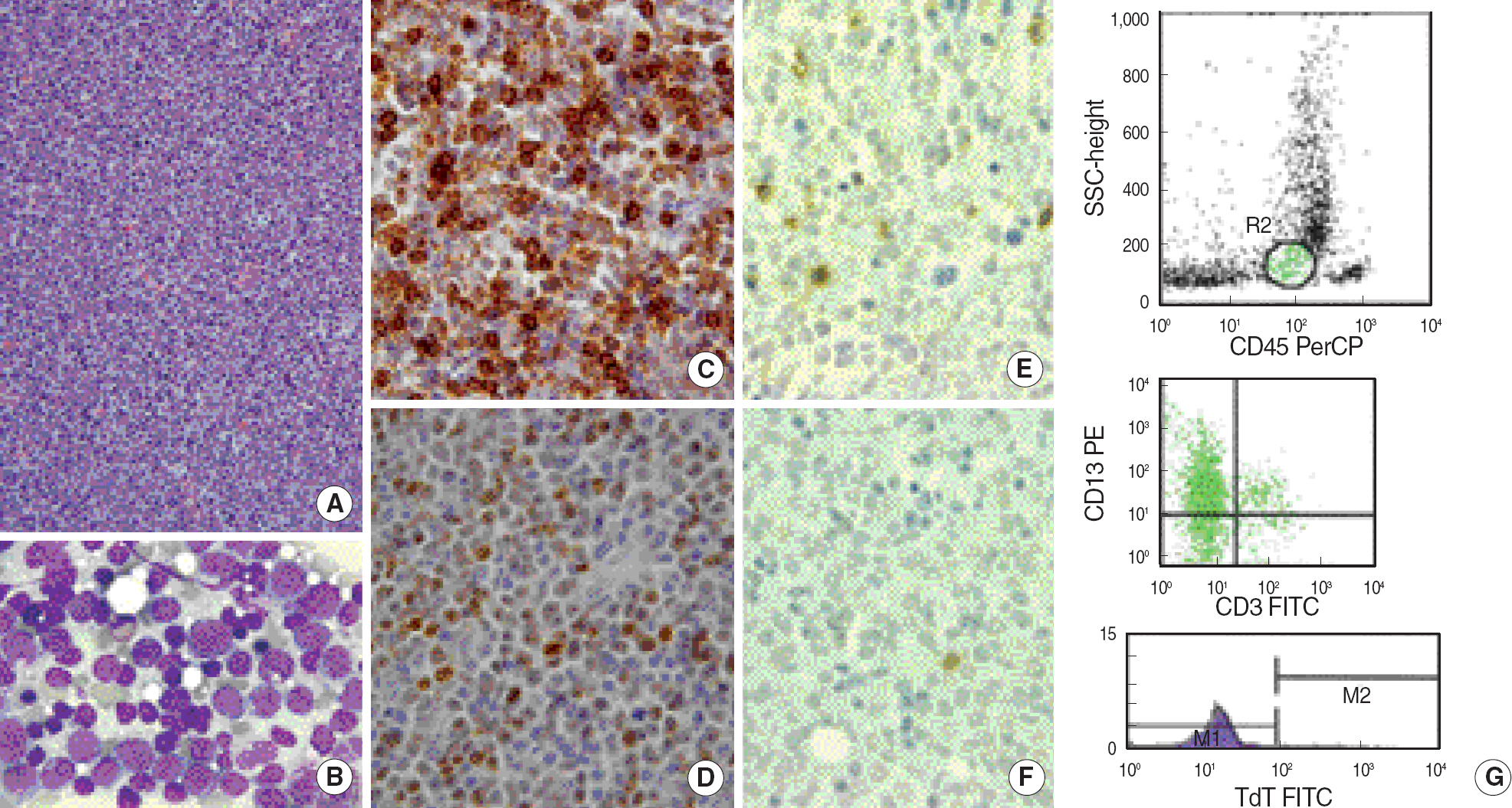
Fig. 1. Patient 1. (A) Cervical lymph node biopsy showing almost complete replacement by malignant cells (H&E stain, ×400). (B) Bone marrow aspirate smear showing blast cells with rather abundant cytoplasm with granules (Wright-Giemsa stain, ×1,000). (C, D) Immunohistochemical stains on lymph node biopsy. The majority of neoplastic cells are strongly positive for CD3 (C) and TdT (D) (×1,000). (E, F) Immunohistochemical stains on bone marrow biopsy. The majority of neoplastic cells are negative for CD3 (E) and TdT (F) (×1,000). (G) Flow cytometric immunophenotyping of the marrow blasts showing negative expression of CD3 and TdT. Abbreviation: Tdt, terminal deoxynucleotidyl transferase.

Fig. 2. Patient 2. (A) Cervical lymph node biopsy showing diffuse infiltration by neoplastic cells (H&E stain, ×400). (B) Bone marrow aspirate smear showing blast cells (arrows) with high nucleus/cytoplasm ratio and prominent nucleoli (Wright-Giemsa stain, ×1,000). (C) Immunohistochemical stain on lymph node biopsy. The large neoplastic cells showed positivity to MPO (×1,000). (D) Immunohistochemical stain on bone marrow biopsy. The neoplastic cells showed negativity to MPO (×1,000). (E) Flow cytometric immunophenotyping of the marrow blasts showing negative expression of MPO. Abbreviation: MPO, myeloperoxidase.
Reference
-
1.Khalidi HS., Medeiros LJ., Chang KL., Brynes RK., Slovak ML., Arber DA. The immunophenotype of adult acute myeloid leukemia: high frequency of lymphoid antigen expression and comparison of immunophenotype, French-American-British classification, and karyotypic abnormalities. Am J Clin Pathol. 1998. 109:211–20.2.Swerdlow SH, Campo E, editors. WHO classification of tumours of haematopoietic and lymphoid tissues. 4th ed.Lyon: IARC Press;2008. p. 149–55.3.Brunning RD., Matutes E, et al. Acute leukaemias of ambiguous lineage. Vardiman JW, editor. Pathology and genetics of tumours of the haemopoietic and lymphoid tissues. Lyon, France: IARC Press;2001. p. 106–7.4.The value of c-kit in the diagnosis of biphenotypic acute leukemia. EGIL (European Group for the Immunological Classification of Leukaemias). Leukemia. 1998. 12:2038.5.Craig FE., Foon KA. Flow cytometric immunophenotyping for hematologic neoplasms. Blood. 2008. 111:3941–67.
Article6.Fisher DE., Jacobson JO., Ault KA., Harris NL. Diffuse large cell lymphoma with discordant bone marrow histology. Clinical features and biological implications. Cancer. 1989. 64:1879–87.
Article7.Kluin PM., van Krieken JH., Kleiverda K., Kluin-Nelemans HC. Discordant morphologic characteristics of B-cell lymphomas in bone marrow and lymph node biopsies. Am J Clin Pathol. 1990. 94:59–66.
Article8.Onciu M., Berrak SG., Medeiros LJ., Katz RL., Huh YO. Discrepancies in the immunophenotype of lymphoma cells in samples obtained simultaneously from different anatomic sites. Am J Clin Pathol. 2002. 117:644–50.
Article9.Inghirami G., Wieczorek R., Zhu BY., Silber R., Dalla-Favera R., Knowles DM. Differential expression of LFA-1 molecules in non-Hodgkin's lymphoma and lymphoid leukemia. Blood. 1988. 72:1431–4.
Article10.Pals ST., Horst E., Ossekoppele GJ., Figdor CG., Scheper RJ., Meijer CJ. Expression of lymphocyte homing receptor as a mechanism of dissemination in non-Hodgkin's lymphoma. Blood. 1989. 73:885–8.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Bone Marrow Necrosis in CD7 positive Acute Myeloid Leukemia
- A case of bone marrow necrosis in acute lymphoblastic leukemia
- Generation and Characterization of Alloenic Radiation Bone Marrow Chimera
- Mixed-phenotype acute leukemia treated with decitabine
- A Case of Bone Marrow Necrosis Following Induction Chemotherapy in Childhood Acute Lymphoblastic Leukemia
