Fluoroscopically Guided Balloon Dilation for Benign Anastomotic Stricture in the Upper Gastrointestinal Tract
- Affiliations
-
- 1Department of Radiology and Research Institute of Radiology, University of Ulsan College of Medicine, Asan Medical Center, Seoul, Korea. jhshin@amc.seoul.kr
- KMID: 1076463
- DOI: http://doi.org/10.3348/kjr.2008.9.4.364
Abstract
- A benign anastomotic stricture is a common complication of upper gastrointestinal (UGI) surgery and is difficult to manage conservatively. Fluoroscopically guided balloon dilation has a number of advantages and is a safe and effective procedure for the treatment of various benign anastomotic strictures in the UGI tract.
Keyword
MeSH Terms
Figure
-
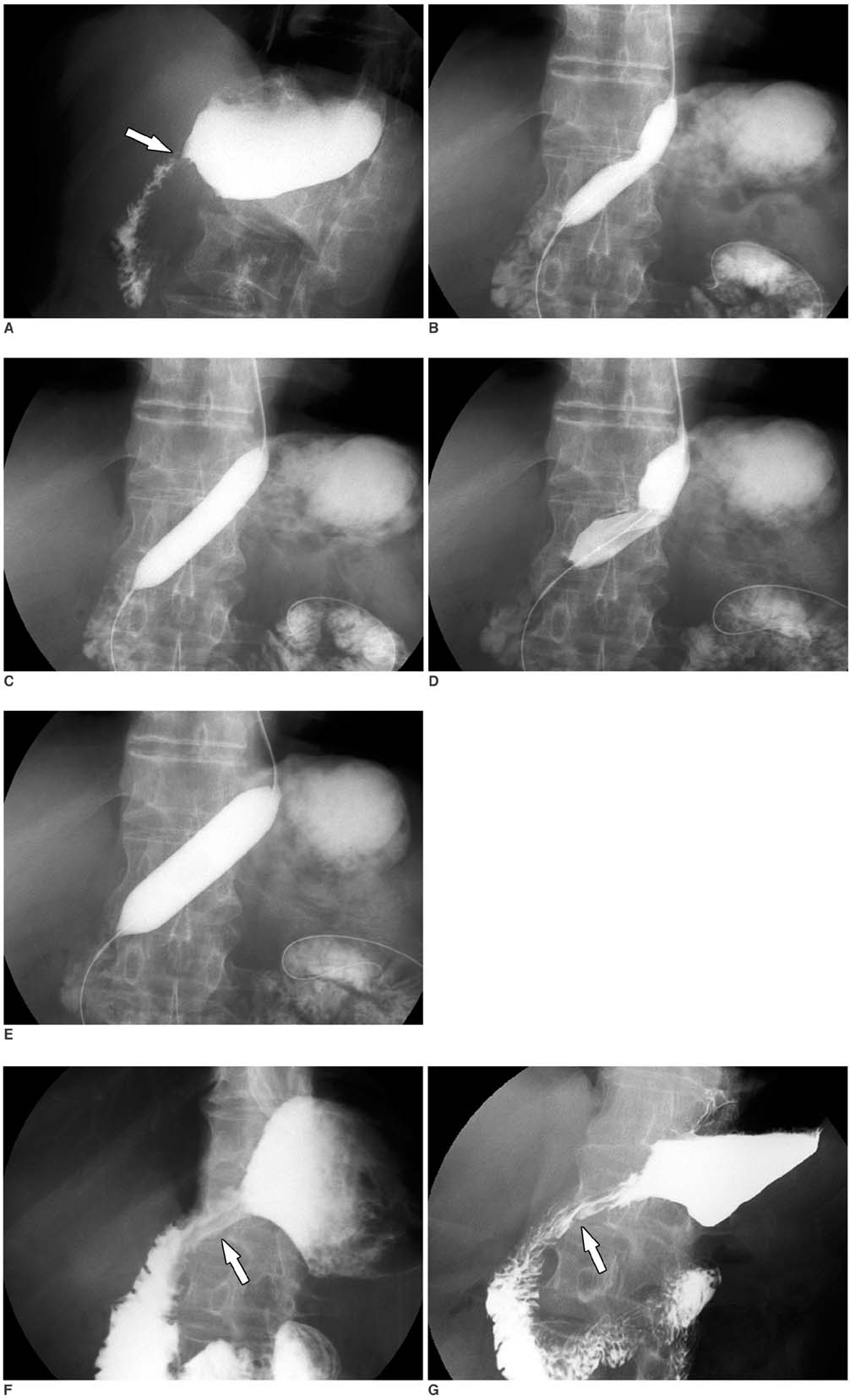
Fig. 1 Fluoroscopically guided balloon dilation for anastomotic stricture at gastroduodenostomy. A. UGI series before balloon dilation shows anastomotic stricture (arrow) at gastroduodenostomy. B-E. Anastomotic stricture is initially dilated using 15-mm-diameter balloon. As dilation is easily accomplished, caliber of balloon catheter is increased to 20 mm. F, G. UGI series immediately (F) and one month after (G) balloon dilation showed improvement of luminal diameter (arrows).
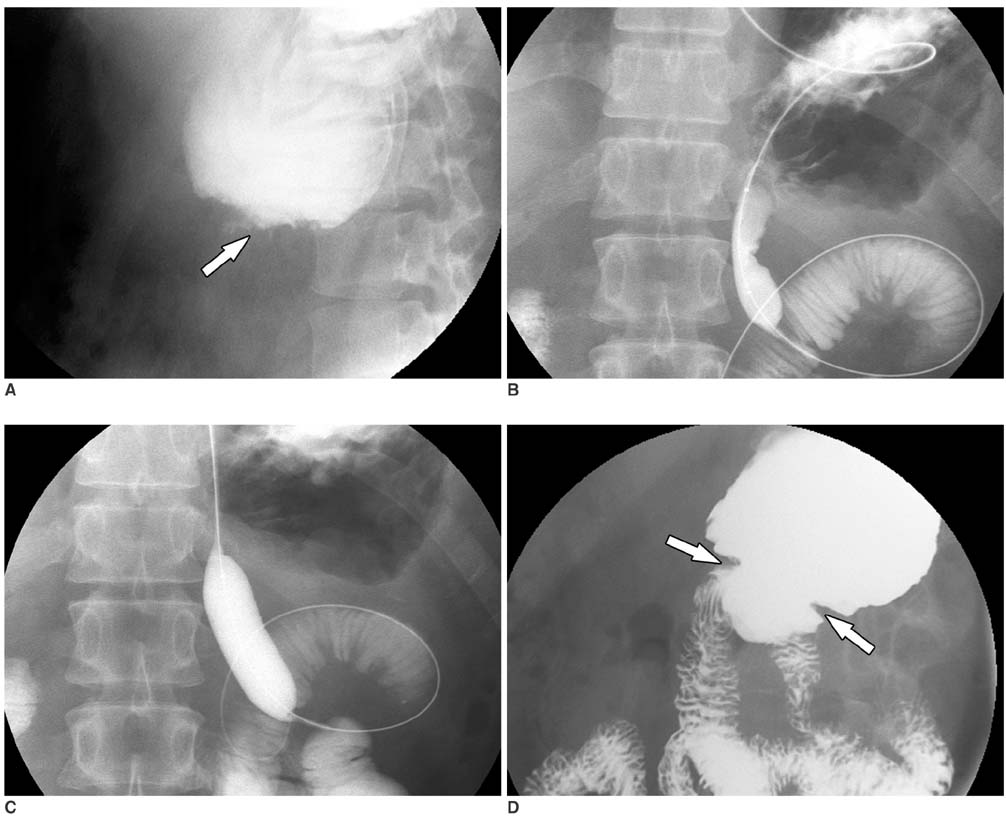
Fig. 2 Fluoroscopically guided balloon dilation for anastomotic stricture at gastrojejunostomy. A. UGI series before balloon dilation shows severe anastomotic stricture (arrow) at gastrojejunostomy with no passage of contrast medium. B, C. 20-mm-diameter balloon is placed and is inflated until waist forms by stricture disappeared. D. One month after balloon dilation, anastomotic stricture is greatly improved (arrows).
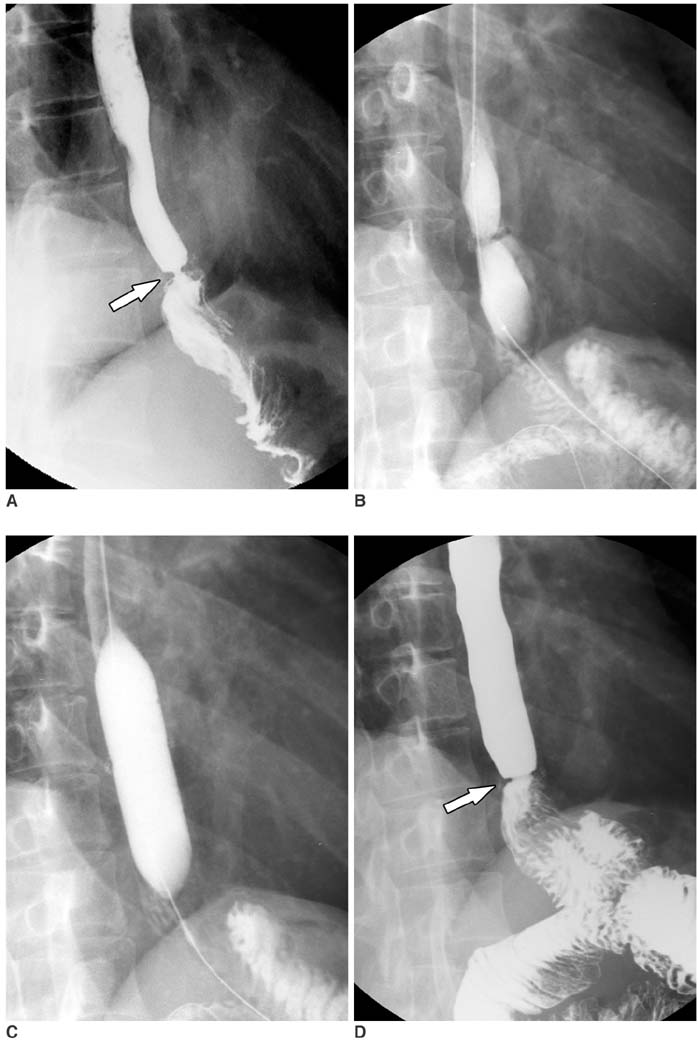
Fig. 3 Fluoroscopically guided balloon dilation for anastomotic stricture at esophagojejunostomy. A. UGI series before balloon dilation shows severe anastomotic stricture (arrow) at esophagojejunostomy. B, C. 20-mm-diameter balloon is placed and is inflated until waist forms by stricture disappeared. D. Immediately after balloon dilation, stricture is greatly improved (arrow).
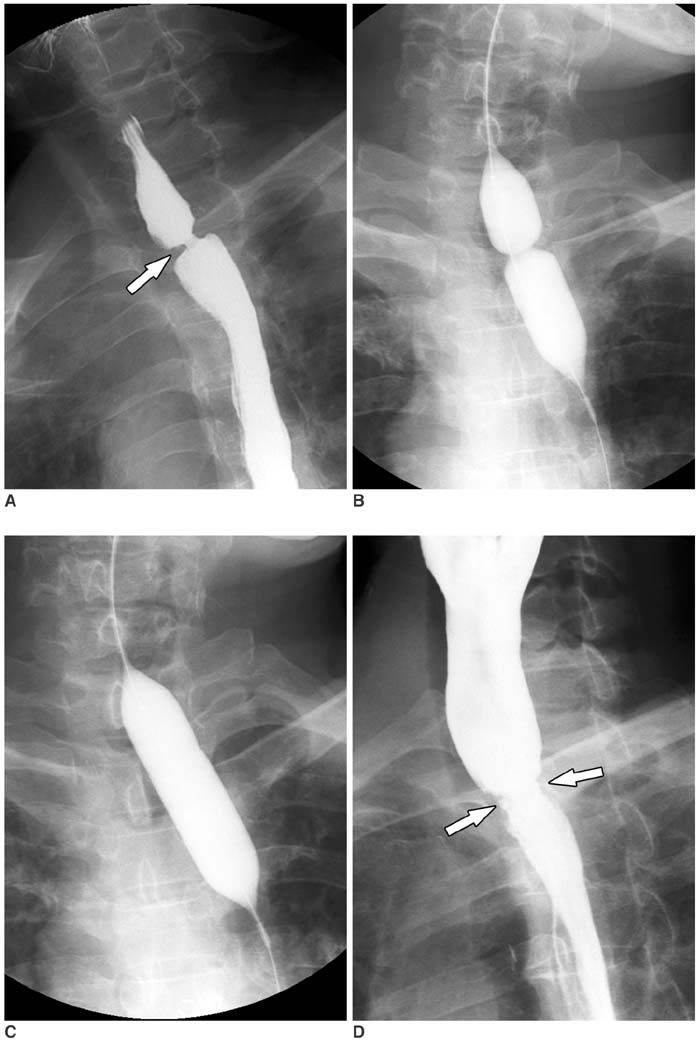
Fig. 4 Fluoroscopically guided balloon dilation for anastomotic stricture after Ivor-Lewis surgery. A. UGI series before balloon dilation shows anastomotic stricture (arrow) at esophagogastrostomy. B, C. 20-mm-diameter balloon is placed and is inflated until waist forms by stricture disappeared. D. Immediately after balloon dilation, stricture is greatly improved (arrow).
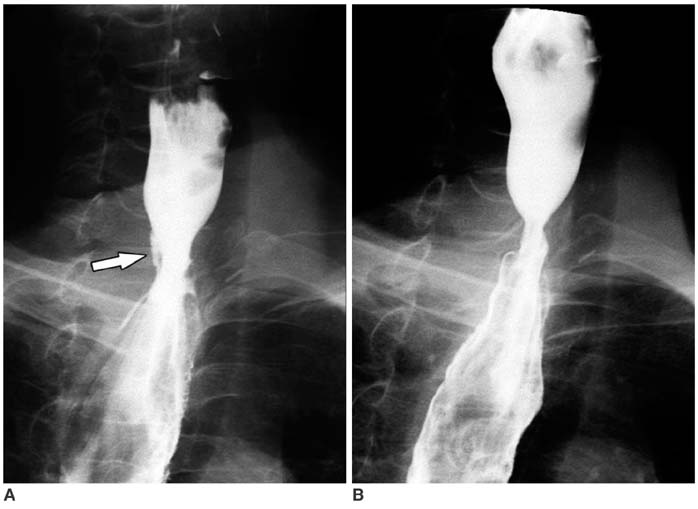
Fig. 5 Intramural rupture of anastomosis (type 1 rupture) after fluoroscopically guided balloon dilation for anastomotic stricture after Ivor-Lewis surgery. UGI series obtained immediately after balloon dilation (A) shows small amount of contrast leakage (arrow). One-month follow-up UGI series (B) shows healed intramural tear.
Reference
-
1. Cho YK, Shin JH, Kim BS, Yook JH, Song HY, Kim JH, et al. Fluoroscopically guided balloon dilation of anastomotic strictures after total gastrectomy: long-term results. AJR Am J Roentgenol. 2007. 188:647–651.2. Kim JH, Shin JH, Bae JI, Di ZH, Lim JO, Kim TH, et al. Gastric outlet obstruction caused by benign anastomotic stricture: treatment by fluoroscopically guided balloon dilation. J Vasc Interv Radiol. 2005. 16:699–704.3. Ko HK, Shin JH, Song HY, Kim YJ, Ko GY, Yoon HK, et al. Balloon dilation of anastomotic strictures secondary to surgical repair of esophageal atresia in a pediatric population: long-term results. J Vasc Interv Radiol. 2006. 17:1327–1333.4. Jha S, Levine MS, Rubesin SE, Dumon K, Kochman ML, Laufer I, et al. Detection of stricture on upper gastrointestinal tract radiographic examinations after laparoscopic Roux-en-Y gastric bypass surgery: importance of projection. AJR Am J Roentgenol. 2006. 186:1090–1093.5. Kim JH, Shin JH, Di ZH, Ko GY, Yoon HK, Sung KB, et al. Benign duodenal strictures: treatment by means of fluoroscopically guided balloon dilation. J Vasc Interv Radiol. 2005. 16:543–548.6. Vance PL, de Lange EE, Shaffer HA Jr, Schirmer B. Gastric outlet obstruction following surgery for morbid obesity: efficacy of fluoroscopically guided balloon dilation. Radiology. 2002. 222:70–72.7. Holt PD, de Lange EE, Shaffer HA Jr. Strictures after gastric surgery: treatment with fluoroscopically guided balloon dilatation. AJR Am J Roentgenol. 1995. 164:895–899.8. Kim HC, Shin JH, Song HY, Park SI, Ko GY, Yoon HK, et al. Fluoroscopically guided balloon dilation for benign anastomotic stricture after Ivor-Lewis esophagectomy: experience in 62 patients. J Vasc Interv Radiol. 2005. 16:1699–1704.9. de Lange EE, Shaffer HA Jr. Anastomotic strictures of the upper gastrointestinal tract: results of balloon dilation. Radiology. 1988. 167:45–50.10. McLean GK, Cooper GS, Hartz WH, Burke DR, Meranze SG. Radiologically guided balloon dilation of gastrointestinal strictures. Part I. Technique and factors influencing procedural success. Radiology. 1987. 165:35–40.11. McLean GK, Cooper GS, Hartz WH, Burke DR, Meranze SG. Radiologically guided balloon dilation of gastrointestinal strictures. Part II. Results of long-term follow-up. Radiology. 1987. 165:41–43.12. Weintraub JL, Eubig J. Balloon catheter dilatation of benign esophageal strictures in children. J Vasc Interv Radiol. 2006. 17:831–835.13. Kim JH, Song HY, Park SW, Yoon CJ, Shin JH, Yook JH, et al. Early symptomatic strictures after gastric surgery: palliation with balloon dilation and stent placement. J Vasc Interv Radiol. 2008. 19:565–570.14. Said M, Mekki M, Golli M, Memmi F, Hafsa C, Braham R, et al. Balloon dilatation of anastomotic strictures secondary to surgical repair of oesophageal atresia. Br J Radiol. 2003. 76:26–31.15. Ahmad J, Martin J, Ikramuddin S, Schauer P, Slivka A. Endoscopic balloon dilation of gastroenteric anastomotic stricture after laparoscopic gastric bypass. Endoscopy. 2003. 35:725–728.16. Bains MS. Ivor Lewis esophagectomy. Chest Surg Clin N Am. 1995. 5:515–526.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Use of a Cutting Balloon Dilation as a Rescue Therapy in Patients with Benign Bilioenteric Anastomotic Strictures Refractory to Conventional Balloon Dilation
- Balloon Dilatation and Bougienage of Post-operative Anastomotic Site Stricture of Upper G-I Tract
- Risk factors for recurrent stenosis after balloon dilation for benign hepaticojejunostomy anastomotic stricture
- Balloon dilatation for the treatment of stricture of gastrojejunostomy
- Fluoroscopically guided balloon dilation of esophageal stricture in Plummer–Vinson syndrome: A report of two cases
