Techniques, Clinical Applications and Limitations of 3D Reconstruction in CT of the Abdomen
- Affiliations
-
- 1Division of Abdominal Imaging and Intervention, Department of Radiology, Massachusetts General Hospital and Harvard Medical School. mmaher@partners.org
- KMID: 1066246
- DOI: http://doi.org/10.3348/kjr.2004.5.1.55
Abstract
- Enhanced z-axis coverage with thin overlapping slices in breath-hold acquisitions with multidetector CT (MDCT) has considerably enhanced the quality of multiplanar 3D reconstruction. This pictorial essay describes the improvements in 3D reconstruction and technical aspects of 3D reconstruction and rendering techniques available for abdominal imaging. Clinical applications of 3D imaging in abdomen including liver, pancreaticobiliary system, urinary and gastrointestinal tracts and imaging before and after transplantation are discussed. In addition, this article briefly discusses the disadvantages of thin-slice acquisitions including increasing numbers of transverse images, which must be reviewed by the radiologist.
Keyword
MeSH Terms
-
Adult
Aged
Biliary Tract/radiography
Female
Gastrointestinal Tract/radiography
Human
Image Processing, Computer-Assisted/*methods
Imaging, Three-Dimensional
Liver/radiography
Liver Transplantation/radiography
Male
Middle Aged
Pancreas/radiography
Radiography, Abdominal/*methods
Tomography, X-Ray Computed/*methods
Urography/methods
Figure
-

Fig. 1 Liver donor evaluation in a 50-year-old man with CT angiography. Maximum intensity projection image (A) demonstrates hepatic arterial anatomy with left hepatic (LH) artery originating from celiac trunk (arrow) and right hepatic (RH) artery arising from superior mesenteric (SM) artery. 3D surface rendering in the same patient depicts entire hepatic lobe volume (B) and left lobe volume (C) to determine liver volume in living-related liver donor.

Fig. 2 Unexpected finding in a 35-year-old woman who underwent CT evaluation prior to liver donor surgery. Axial (A), multiplanar volume rendering (B) and maximum intensity projection (C) images show dissection of hepatic artery (arrow) with tortuous, dilated and featureless false lumen (arrowheads) without branching, which was not appreciated on conventional angiogram (D). The false lumen of common hepatic artery dissection is seen only on CT angiography. Distal communication of true and false lumens maintains the patency and perfusion of right and left hepatic arteries.

Fig. 3 3D reconstruction of axial source data of 42-year-old man, status post-liver transplant. Doppler examination did not definitively demonstrate hepatic arterial flow. Multiplanar reconstruction image shows patent donor (white arrowhead) and recipient hepatic artery (black arrowhead) and demonstrates the position of transjugular intrahepatic portrsystemic shunt (arrow).

Fig. 4 Contrast enhanced CT image (A) of a 72-year-old woman with large cystic mass (white arrow) in the pancreatic head. Coronal multiplanar volume rendering (B) shows relationship of the mass with the "C" loop of duodenum (black arrows).
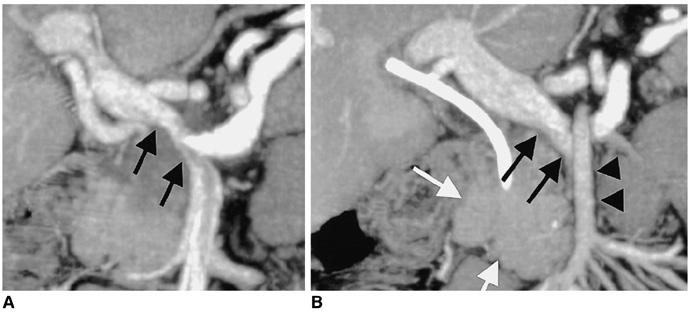
Fig. 5 Multiplanar volume rendering image (A) of axial source data of a 60-year-old man with pancreatic adenocarcinoma (white arrows) encasing the portal vein and distal superior mesenteric vein (black arrows). Intraluminal filling defect suggestive of a thrombus is seen in the superior mesenteric vein. Note the exquisite display of 3D vascular anatomy of superior mesenteric artery (black arrowheads) in relation with the tumor (B).

Fig. 6 CT cholangiogram of dilated biliary ductal system in a 47-year-old woman with cholangiocarcinoma at porta hepatis (arrow). Axial CT image (A) shows dilated intrahepatic biliary system with hypodense mass at the porta hepatis. Minimum intensity projection (B) rendering provides a "cholangiographic" view of the dilated intrahepatic ductal system with mass in the porta hepatis region.
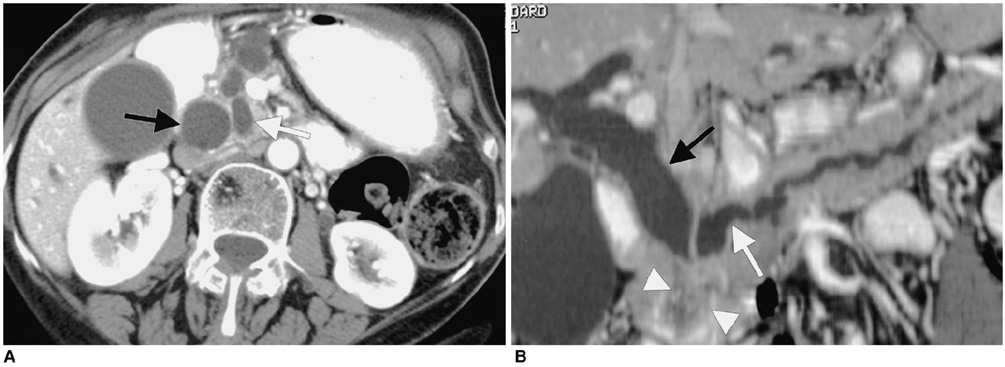
Fig. 7 Double duct sign on 3D CT in a 65-year-old man with biopsy proven ampullary carcinoma (white arrowheads). Axial CT image (A) shows dilated common bile duct (black arrow) and pancreatic duct (white arrow). Curved multiplanar reconstruction (B) images show smooth dilatation of pancreatic duct (white arrow) and common bile duct (black arrow).
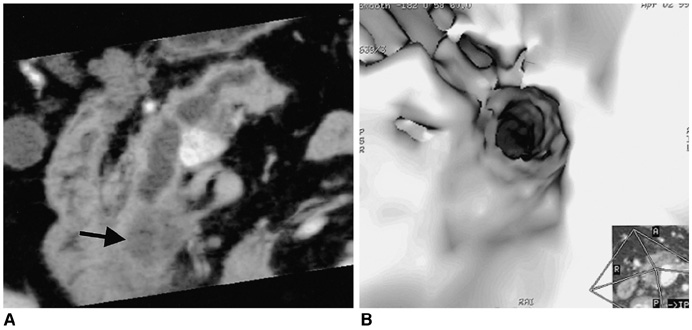
Fig. 8 Virtual endoscopy of pancreatic duct in a 62-year-old woman. Curved multiplanar reconstruction image shows a small hypodense mass in the pancreatic head (arrow) with dilated pancreatic duct (A). Virtual endoscopy (B) of pancreatic duct shows the attenuated lumen of the pancreatic duct due to extrinsic compression from periampullary carcinoma.
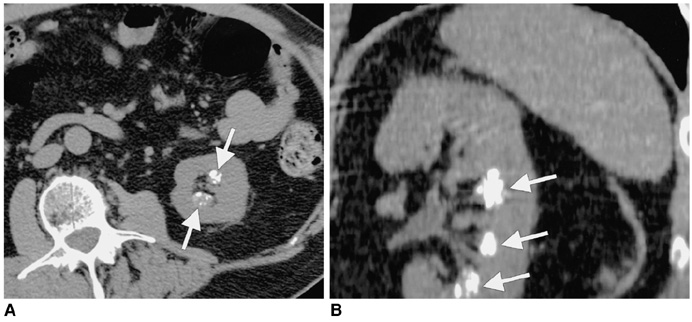
Fig. 9 Coronal reformats aid with characterization of caliceal abnormalities. Axial CT image (A) of a 31-year-old woman shows calcification in the renal papillae (arrows). Coronal multiplanar reconstruction (B) shows typical radiographic features of medullary nephrocalcinosis (arrows).

Fig. 10 Axial CT image (A) of a 68-year-old man with diabetes mellitus and papillary necrosis shows a filling defect (sloughed papilla) in the renal calyces (black arrow). Maximum intensity projection image (B) shows fraying and blunting of the right renal calyces (white arrows), a classical radiographic feature of papillary necrosis first described with excretory urography.

Fig. 11 Axial CT image (A) of a 32-year-old man with a hydronephrotic upper pole moiety (arrow) of a duplicated renal collecting system. Coronal multiplanar reconstruction (B) confirms hydronephrosis of upper pole moiety (arrow) and normal lower pole moiety.

Fig. 12 Coronal reformat accurately displays urinary anatomy. Maximum intensity projection shows a duplex non-dilated pelvicaliceal system on the left side.
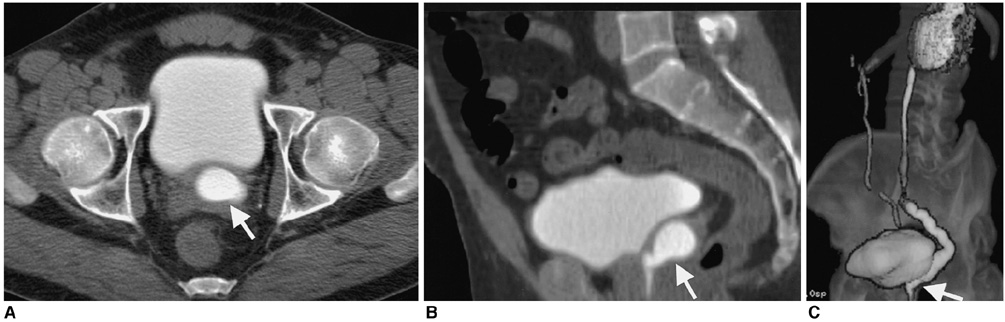
Fig. 13 3D CT can combine advantages of intravenous urography and voiding cystourethrogram and retrograde urethrogrogram. Axial CT image (A) in 47-year-old man with recurrent urinary tract infection shows a dilated, ectopic left ureter (arrow) within the prostate. Sagittal multiplanar reconstruction (B) shows a dilated, ectopic ureter (arrow) opening into the posterior urethra. 3D surface rendering (C) demonstrates anatomic relationship of the ectopic ureter to the regional anatomy.
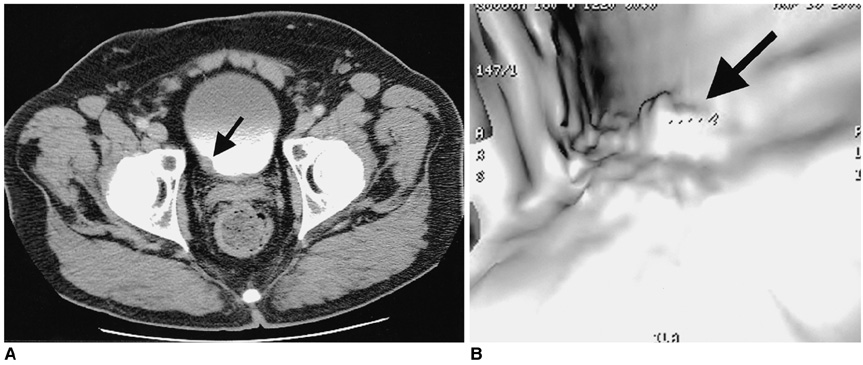
Fig. 14 Virtual cystoscopy is useful in evaluation of bladder tumors. Axial (A) and virtual cystoscopy (B) images in a 67-year-old man demonstrate bladder wall thickening and irregularity (arrow). Virtual cystoscopy depicts the surface of the bladder mucosa and shows the size and site of the bladder neoplasm (arrow).
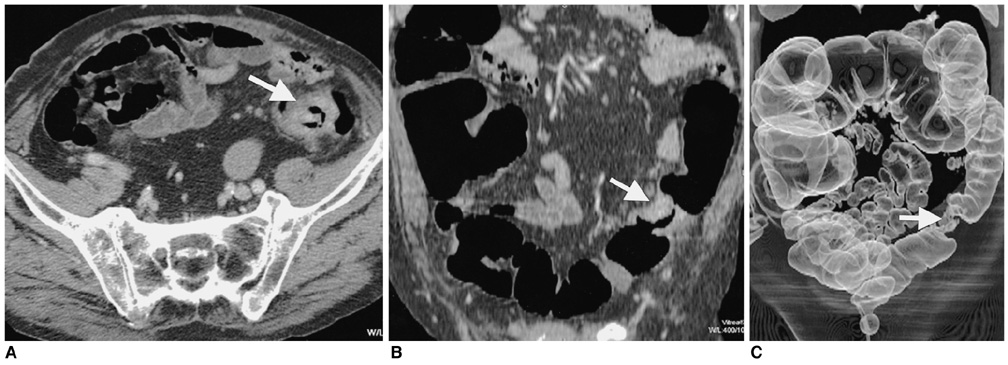
Fig. 15 3D CT of malignant colonic stricture in a 73-year-old man. Axial CT (A) and coronal multiplanar reconstruction (B) images show circumferential short segment thickening of the sigmoid colon (arrow) suggestive of colon cancer. 3D CT colonography (C) as a "double-contrast barium enema" simulating image, reveals short segment "apple-core" lesion (arrow) in the sigmoid colon.
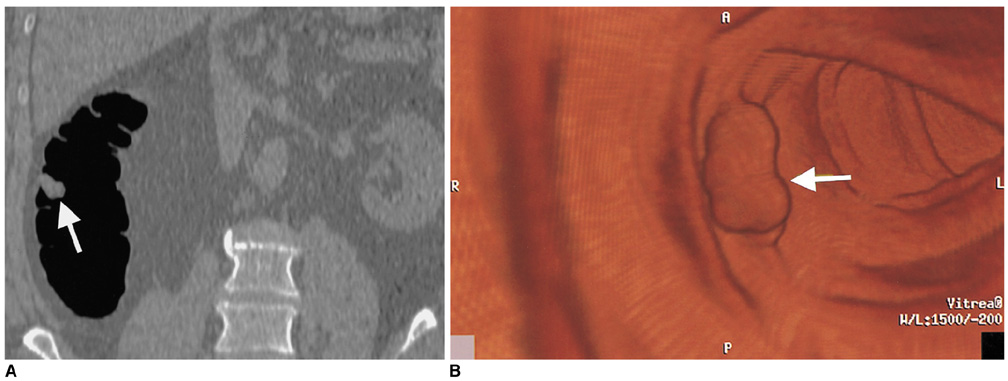
Fig. 16 Screening CT colonoscopy was performed in a 55-year-old man. Coronal reformat (A) and virtual colonoscopy (B) images demonstrate a polyp (arrow) in the ascending colon. 3D reconstruction in CT colonoscopy also helps in differentiating normal mucosal folds from intraluminal masses.
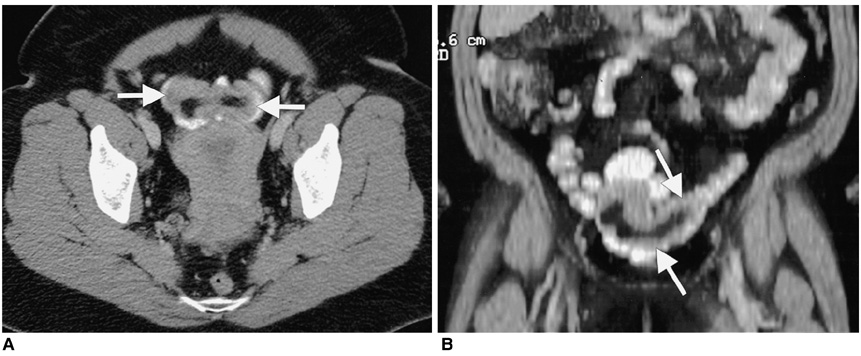
Fig. 17 Axial image (A) shows a fat containing intraluminal mass (arrows) in a loop of ileum in a 49-year-old woman with intussuscepted Meckel's diverticulum. Coronal multiplanar reconstruction image (B) shows a tubular fat containing filling defect (arrows) in the ileal lumen that was contiguous with the mesenteric fat.
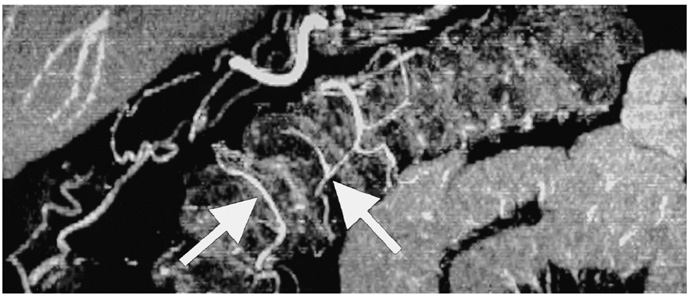
Fig. 18 Multiplanar volume rendering image of a 50-year-old man displays small vessels of the arterial plexus (arrows) of the large intestine. Depiction of vasa recti is showing promise in increasing the scope of CT evaluation of patients with bowel ischemia and assessment of disease activity in patients with inflammatory bowel disease.

Fig. 19 3D reconstruction with 16-slice CT scanner. Coronal multiplanar volume rendering (A) and minimum intensity projection (B) images reconstructed from sub-millimeter images (0.625 mm) of a 60-year-old woman show right renal mass. Note the exquisite demonstration of relation of the mass with right renal artery and an accessory renal artery (arrow) (General Medical Systems, Waukesha Wis, U.S.A.).
Cited by 1 articles
-
Three-dimensional CT angiography of the canine hepatic vasculature
Yucheol Jeong, Changyun Lim, Sunkyoung Oh, Joohyun Jung, Jinhwa Chang, Junghee Yoon, Mincheol Choi
J Vet Sci. 2008;9(4):407-413. doi: 10.4142/jvs.2008.9.4.407.
Reference
-
1. Hu H, He HD, Foley WD, Fox SH. Four multidetector-row helical CT: image quality and volume coverage speed. Radiology. 2000. 215:55–62.2. Wigmore SJ, Redhead DN, Yan XJ, et al. Virtual hepatic resection using three-dimensional reconstruction of helical computed tomography angioportograms. Ann Surg. 2001. 233:221–226.3. Kamel IR, Kruskal JB, Keogan MT, Goldberg SN, Warmbrand G, Raptopoulos V. Multidetector CT of potential right-lobe liver donors. AJR Am J Roentgenol. 2001. 177:645–651.4. Bogetti JD, Herts BR, Sands MJ, Carroll JF, Vogt DP, Henderson JM. Accuracy and utility of 3-dimensional computed tomography in evaluating donors for adult living related liver transplants. Liver Transpl. 2001. 7:687–692.5. Rubin GD, Beaulieu CF, Argiro V, et al. Perspective volume rendering of CT and MR images: applications for endoscopic imaging. Radiology. 1996. 199:321–323.6. Caoili EM, Cohan RH, Korobkin M, et al. Urinary tract abnormalities: initial experience with multi-detector row CT urography. Radiology. 2002. 222:353–360.7. Cody DD. AAPM/RSNA physics tutorial for residents: topics in CT. Image processing in CT. RadioGraphics. 2002. 22:1255–1268.8. O'Malley ME, Boland GW, Wood BJ, Fernandez-del Castillo C, Warshaw AL, Mueller PR. Adenocarcinoma of the head of the pancreas: determination of surgical unresectability with thin-section pancreatic-phase helical CT. AJR Am J Roentgenol. 1999. 173:1513–1518.9. Takeshita K, Furui S, Yamauchi T, et al. Minimum intensity projection image and curved reformation image of the main pancreatic duct obtained by helical CT in patients with main pancreatic duct dilation. Nippon Igaku Hoshasen Gakkai Zasshi. 1999. 59:146–148.10. Park SJ, Han JK, Kim TK, Choi BI. Three-dimensional spiral CT cholangiography with minimum intensity projection in patients with suspected obstructive biliary disease: comparison with percutaneous transhepatic cholangiography. Abdom Imaging. 2001. 26:281–286.11. Schreyer HH, Uggowitzer MM, Ruppert-Kohlmayr A. Helical CT of the urinary organs. Eur Radiol. 2002. 12:575–591.12. Marukawa K, Horiguchi J, Shigeta M, Nakamoto T, Usui T, Ito K. Three dimensional navigator for retroperitoneal laparoscopic nephrectomy using multidetector row computerized tomography. J Urol. 2002. 168:1933–1936.13. Song JH, Francis IR, Platt JF, et al. Bladder tumor detection at virtual cystoscopy. Radiology. 2001. 218:95–100.14. Kim JK, Ahn JH, Park T, Ahn HJ, Kim CS, Cho KS. Virtual cystoscopy of the contrast material-filled bladder in patients with gross hematuria. AJR Am J Roentgenol. 2002. 179:763–768.15. Horton KM, Fishman EK. Volume-rendered 3D CT of the mesenteric vasculature: normal anatomy, anatomic variants, and pathologic conditions. RadioGraphics. 2002. 22:161–172.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Surface Functionalization of Three-Dimensional Printed Scaffold for Biomedical Application
- Applications of Three-Dimensional Printing in Cardiovascular Surgery: A Case-Based Review
- Application of 3-dimensional printing implants for bone tumors
- Fabrication of 3D-Printed Implant for Two-Stage Ear Reconstruction Surgery and Its Clinical Application
- A Review of Current Clinical Applications of Three-Dimensional Printing in Spine Surgery
