Radiological and Clinical Characteristics of a Military Outbreak of Pandemic H1N1 2009 Influenza Virus Infection
- Affiliations
-
- 1Department of Radiology, Armed Force Byukjae Hospital, Gyeonggi-do 412-510, Korea.
- 2Department of Radiology, Seoul National University College of Medicine, and Institute of Radiation Medicine, Seoul National University Medical Research Center, Seoul 110-744, Korea. cmpark@radiol.snu.ac.kr
- 3Department of Family Medicine, Armed Force Byukjae Hospital, Gyeonggi-do 412-510, Korea.
- 4Department of Family Medicine, Gangneung Asan Hospital, Ulsan University College of Medicine, Gangwon-do 210-711, Korea.
- 5Department of Internal Medicine, Armed Force Byukjae Hospital, Gyeonggi-do 412-510, Korea.
- 6Division of Pulmonary and Critical Care Medicine, Department of Internal Medicine and Lung Institute, Seoul National University College of Medicine, Seoul 110-744, Korea.
- 7Department of Family Medicine, Chungnam National University School of Medicine, Daejeon 301-721, Korea.
- KMID: 984895
- DOI: http://doi.org/10.3348/kjr.2010.11.4.417
Abstract
OBJECTIVE
To describe detailed clinical and radiological features of the pandemic H1N1 2009 influenza viral infection among healthy young males in a semi-closed institutionalized setting.
MATERIALS AND METHODS
A total of 18 patients confirmed with the pandemic H1N1 2009 influenza virus infection from July 18 to July 30, 2009 were enrolled in this study. Each patient underwent an evaluation to determine detailed clinical and radiological features.
RESULTS
All patients presented with high fever (> 38.0degrees C), with accompanying symptoms of cough, rhinorrhea, sore throat, myalgia and diarrhea, and increased C-reactive protein (CRP) values with no leukocytosis nor elevated erythrocyte sedimentation rate (ESR). All patients, including one patient who progressed into acute respiratory distress syndrome, were treated with oseltamivir phosphate and quickly recovered from their symptoms. Chest radiographs showed abnormalities of small nodules and lobar consolidation in only two out of 18 patients. However, six of 12 patients who underwent thin-section CT examinations showed abnormal findings for small ground-glass opacities (GGOs) in addition to poorly-defined nodules with upper lobe predominance.
CONCLUSION
In a population of healthy young adults, elevated CRP with normal ESR and white blood cell levels combined with GGOs and nodules on thin-section CT scans may indicate early signs of infection by the pandemic H1N1 2009 influenza virus.
MeSH Terms
Figure
-
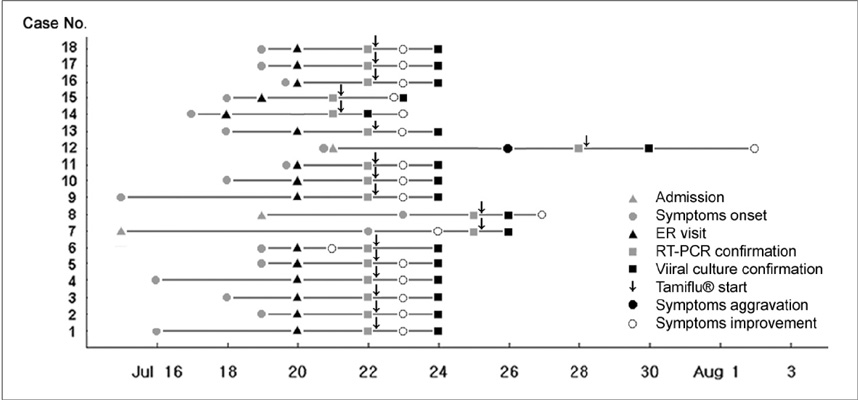
Fig. 1 Clinical course and outcome of all 18 patients. Figure shows brief clinical course and outcome in 18 patients. One patient (case No. 12) progressed into acute respiratory distress syndrome and was placed on mechanical ventilation. Eventually, patient was taken off mechanical ventilation five days after administration of antiviral agent therapy (oseltamivir phosphate, Tamiflu®). In two patients (case No. 6 and 7), symptoms started to improve before administration of antiviral agent therapy for treatment of pandemic H1N1 2009 influenza virus. RT-PCR = reverse-transcriptase-polymerase-chain-reaction
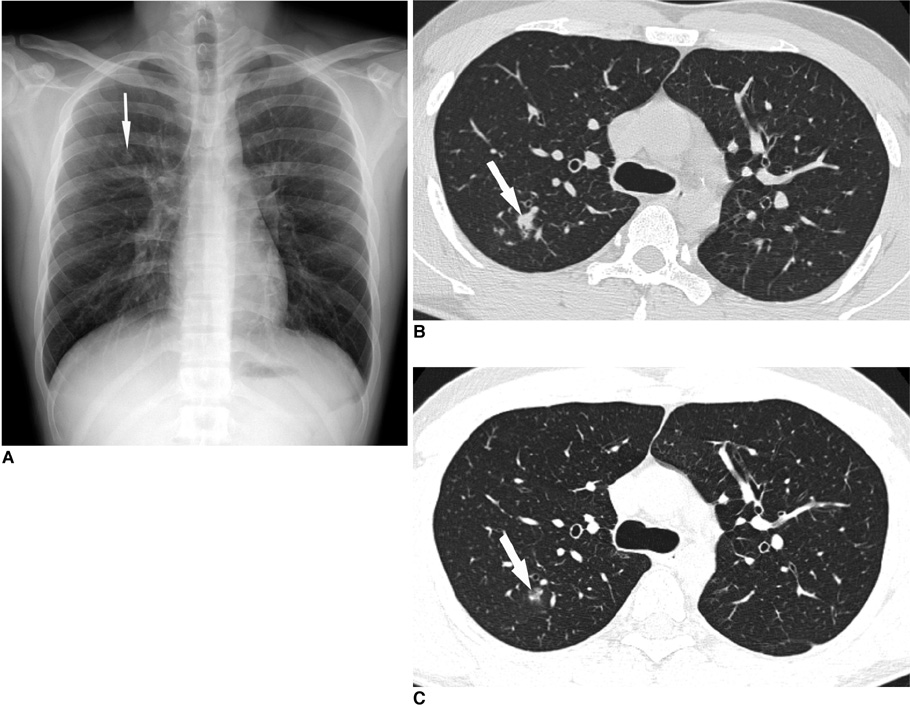
Fig. 2 Small nodules in 20-year-old man with pandemic H1N1 2009 influenza virus infection. A. Plain chest radiograph shows small nodular opacity in right upper lung (arrow). B. Thin-section chest CT shows 10 mm nodule (arrow) in right upper lobe of lung. Several tiny nodules are also shown around nodule. C. Follow-up thin-section CT obtained one week later indicated that this small nodule decreased in size and opacity (arrow). Several tiny nodules that were present in (B) disappeared.
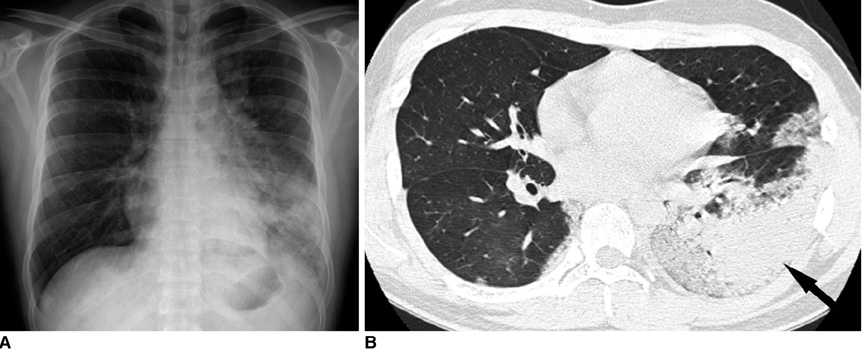
Fig. 3 Consolidations in 22-year-old man with pandemic H1N1 2009 influenza virus infection. A. Plain chest radiograph shows consolidations in left middle and lower lung. Consolidations are also suspected in right lower lung. B. Thin-section chest CT image at level of left atrial appendage shows consolidation in left lower lobe (arrow) accompanied by ground-glass opacities in left upper lobe and both lower lobes of lung.
Reference
-
1. Influenza A (H1N1) - update 68. World Health Organization. Accessed October 8, 2009. at http://www.who.int/csr/don/2009_10_02/en/index.html.2. World now at the start of 2009 influenza pandemic. World Health Organization. Accessed October 8, 2009. at http://www.who.int/mediacentre/news/statements/2009/h1n1_pandemic_phase6_20090611/en/index.html.3. Perez-Padilla R, de la Rosa-Zamboni D, Ponce de Leon S, Hernandez M, Quiñones-Falconi F, Bautista E, et al. Pneumonia and respiratory failure from swine-origin influenza A (H1N1) in Mexico. N Engl J Med. 2009. 361:680–689.4. Chowell G, Bertozzi SM, Colchero MA, Lopez-Gatell H, Alpuche-Aranda C, Hernandez M, et al. Severe respiratory disease concurrent with the circulation of H1N1 influenza. N Engl J Med. 2009. 361:674–679.5. Novel Swine-Origin Influenza A (H1N1) Virus Investigation Team. Dawood FS, Jain S, Finelli L, Shaw MW, Lindstrom S, et al. Emergence of a novel swine-origin influenza A (H1N1) virus in humans. N Engl J Med. 2009. 360:2605–2615.6. Shinde V, Bridges CB, Uyeki TM, Shu B, Balish A, Xu X, et al. Triple-reassortant swine influenza A (H1) in humans in the United States, 2005-2009. N Engl J Med. 2009. 360:2616–2625.7. Belshe RB. Implications of the emergence of a novel H1 influenza virus. N Engl J Med. 2009. 360:2667–2668.8. Interim WHO guidance for the surveillance of human infection with swine influenza A (H1N1) virus. United States Centers for Disease Control and Prevention. 2009. 04. 27. Accessed October 8, 2009. at http://www.wpro.who.int/NR/rdonlyres/0057E73B-E9DE-470D-8B21-B5E7AFE570D0/0/WHO_guidanceforsurveillanceofswineflu27Apr2009.pdf.9. Hospitalized patients with novel influenza A (H1N1) virus infection - California, April-May, 2009. MMWR Morb Mortal Wkly Rep. 2009. 58:536.10. World Health Organization. Human infection with new influenza A (H1N1) virus: clinical observations from Mexico and other affected countries, May 2009. Weekly Epidemiological Record. 2009. 84:185.11. Lee CW, Seo JB, Song JW, Lee HJ, Lee JS, Kim MY, et al. Pulmonary complication of novel influenza A (H1N1) infection: imaging features in two patients. Korean J Radiol. 2009. 10:531–534.12. Agarwal PP, Cinti S, Kazerooni EA. Chest radiographic and CT findings in novel swine-origin influenza A (H1N1) virus (S-OIV) infection. AJR Am J Roentgenol. 2009. 193:1488–1493.13. Ajlan AM, Quiney B, Nicolaou S, Müller NL. Swine-origin influenza A (H1N1) viral infection: radiographic and CT findings. AJR Am J Roentgenol. 2009. 193:1494–1499.14. Dolin R. Fauci AS, Braunwald E, Isselbacher KJ, editors. Infections due to DNA and RNA respiratory viruses. Harrison's principles of internal medicine. 2008. 17th ed. New York, USA: McGraw-Hill;1127–1132.15. Grinblat L, Shulman H, Glickman A, Matukas L, Paul N. Severe acute respiratory syndrome: radiographic review of 40 probable cases in Toronto, Canada. Radiology. 2003. 228:802–809.16. Hansell DM, Bankier AA, MacMahon H, McLoud TC, Müller NL, Remy J. Fleischner Society: glossary of terms for thoracic imaging. Radiology. 2008. 246:697–722.17. Wong KT, Antonio GE, Hui DS, Lee N, Yuen EH, Wu A, et al. Thin-section CT of severe acute respiratory syndrome: evaluation of 73 patients exposed to or with the disease. Radiology. 2003. 228:395–400.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Influenza Associated Pneumonia
- The 2009 H1N1 Pandemic Influenza in Korea
- Epidemiology, clinical manifestations, and management of pandemic novel Influenza A (H1N1)
- Three Reinfection Cases of the Pandemic Influenza (H1N1 2009)
- Effective Containment of Pandemic Influenza (H1N1 2009) Virus Outbreak in an International Residence Hall of a University by Recommended Infection Control Guidance
