Type 2 Hepatorenal Syndrome in a Cirrhotic Patient Who Underwent Gastric Cancer Surgery
- Affiliations
-
- 1Department of Medicine, Seoul National University Bundang Hospital, Seongnam, Korea. kimjw@snubh.org
- KMID: 948774
- DOI: http://doi.org/10.4166/kjg.2010.56.3.125
Abstract
- No abstract available.
MeSH Terms
Figure
-
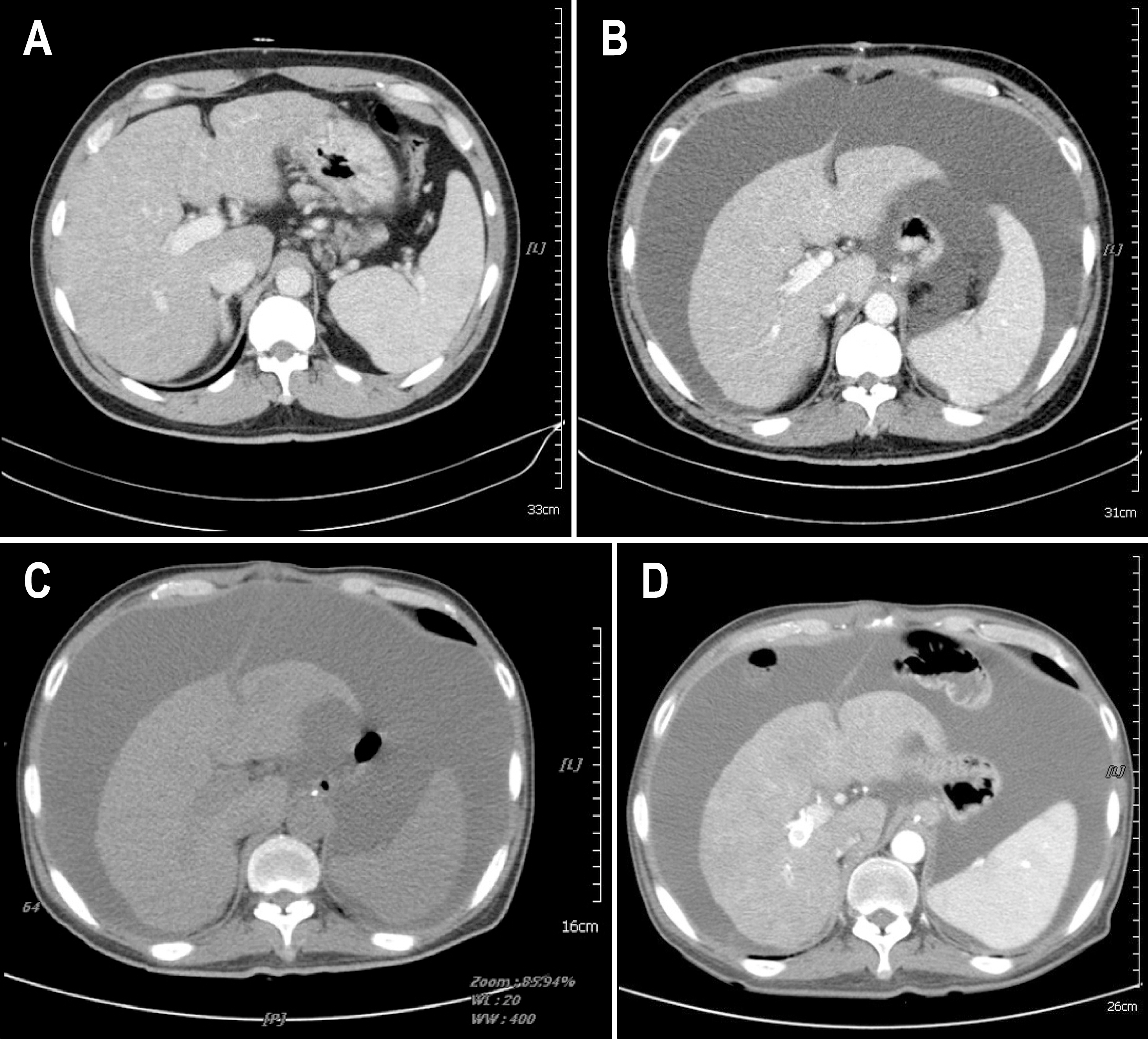
Fig. 1. Abdominal CT scan of the patient before (A) and 18 days after (B) total gastrectomy. Preoperative CT showed features of chronic liver disease without ascites. Postoperative CT showed large amount of ascites and slightly decreased liver volume. Abdominal CT scan after admission to our hospital (C) showed similar findings. After TIPS, ascites decreased slightly, with longer intervals of therapeutic paracentesis (D). TIPS, transjugular intrahepatic portosystemic shunt.
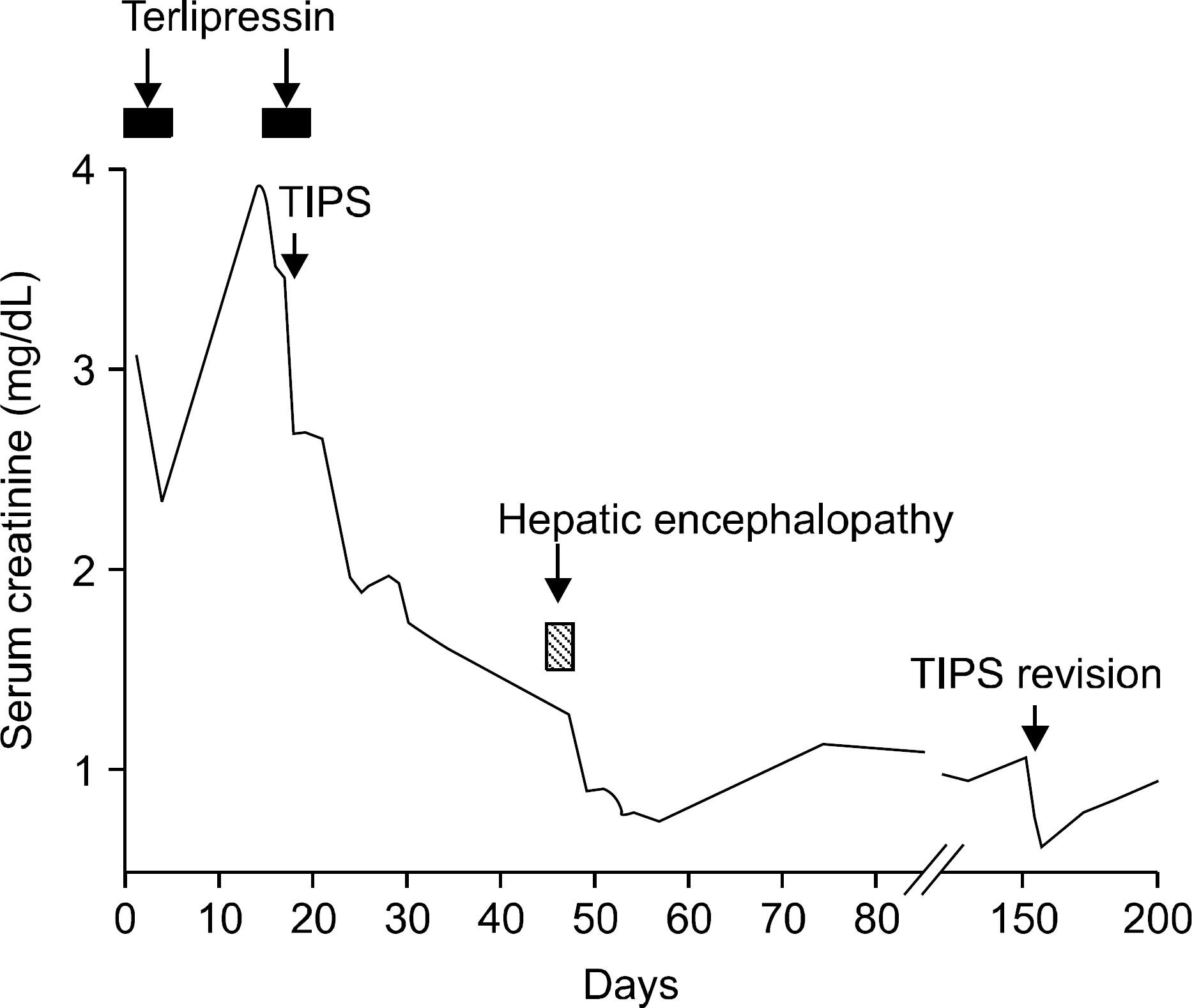
Fig. 2. Hospital course of the patient. See text for details. TIPS, transjugular intrahepatic portosystemic shunt.

Fig. 3. Transjugular intrahepatic portosystemic shunt for the management of type 2 hepatorenal syndrome developed in HCV-related cirrhotic patient who underwent radical total gastrectomy. IVC pressure was measured as 11 mmHg. Portal vein was punctured from hepatic vein and main portal vein pressure was measured as 25 mmHg (A) The tract was dilated with a balloon catheter, and 10 mm×7 cm stent was deployed (B). Main portal vein pressure dropped to 21 mmHg after the procedure. Stent stenosis was detected on day 154 (C), and portal venous pressure rose to 26 mmHg. After balloon dilatation, the portal pressure reduced back to 17 mmHg (D).
Reference
-
1. Arroyo V, Terra C, Ginès P. Advances in the pathogenesis and treatment of type-1 and type-2 hepatorenal syndrome. J Hepatol. 2007; 46:935–946.
Article2. Salerno F, Gerbes A, Ginès P, Wong F, Arroyo V. Diagnosis, prevention and treatment of hepatorenal syndrome in cirrhosis. Postgrad Med J. 2008; 84:662–670.
Article3. Rössle M, Gerbes AL. TIPS for the treatment of refractory ascites, hepatorenal syndrome and hepatic hydrothorax: a critical update. Gut. 2010; 59:988–1000.
Article4. Brensing KA, Textor J, Perz J, et al. Long term outcome after transjugular intrahepatic portosystemic stent-shunt in non-transplant cirrhotics with hepatorenal syndrome: a phase II study. Gut. 2000; 47:288–295.
Article5. Testino G, Ferro C, Sumberaz A, et al. Type-2 hepatorenal syndrome and refractory ascites: role of transjugular intrahepatic portosystemic stent-shunt in eighteen patients with advanced cirrhosis awaiting orthotopic liver transplantation. Hepatogastroenterology. 2003; 50:1753–1755.6. Lee JH, Kim J, Cheong JH, Hyung WJ, Choi SH, Noh SH. Gastric cancer surgery in cirrhotic patients: result of gastrectomy with D2 lymph node dissection. World J Gastroenterol. 2005; 11:4623–4627.
Article7. Isozaki H, Okajima K, Ichinona T, Fujii K, Nomura E, Izumi N. Surgery for gastric cancer in patients with cirrhosis. Surg Today. 1997; 27:17–21.
Article8. Mariette C. Is there a place for esogastric cancer surgery in cirrhotic patients? Ann Surg Oncol. 2008; 15:680–682.
Article9. Jang HJ, Kim JH, Song HH, et al. Clinical outcomes of patients with liver cirrhosis who underwent curative surgery for gastric cancer: a retrospective multicenter study. Dig Dis Sci. 2008; 53:399–404.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Evaluation of Renal Resistive Index in Cirrhotic Patients for Predicting the Hepatorenal Syndrome
- Acute Kidney Injury in Cirrhotic Patients with Portal Hypertension
- Hepatorenal Syndrome
- Predictors of response to therapy with terlipressin and albumin in patients with cirrhosis and type 1 hepatorenal syndrome
- Hepatorenal Syndrome
