Clinical Features and Arthroscopic Findings of Partial Thickness Rotator Cuff Tears
- Affiliations
-
- 1Department of Orthopaedic Surgery, Uijongbu St. Mary's Hospital, College of Medicine, The Catholic University of Korea, Uijeongbu, Korea. oskn@catholic.ac.kr
- 2Department of Orthopaedic Surgery, Kangnam St. Mary's Hospital, College of Medicine, The Catholic University of Korea, Uijeongbu, Korea.
- KMID: 854585
- DOI: http://doi.org/10.4055/jkoa.2007.42.2.177
Abstract
- PURPOSE: To compare the clinical features of partial thickness rotator cuff tears according to location of the tear and to classify the partial thickness rotator cuff tears based on arthroscopic findings. MATERIALS AND METHODS: This study evaluated 138 patients who were arthroscpically proven to be partial thickness rotator cuff tears. Three groups were identified; 56 in the articular side tear, 58 in the bursal side tear, 24 in the both sides tear. The comparison included preoperative clinical features such as pain, range of motion and impingement sign. The partial thickness rotator cuff tears were classified according to the arthroscopic findings. RESULTS: There was no significant difference in the clinical features between articular, bursal and both sides tears. Partial thickness rotator cuff tear can be divided into 5 groups. Type I (n=41): fraying or fibrillation on surface of the cuff. Type II (n=35): fiber disruptions with or without displacement. Type III (n=38): flap tear or fragmentation. Type IV (n=16): both articular and bursal side tears without communications. Type V (n=8): impending a full thickness tear. CONCLUSION: It is difficult to differentiate the clinical features based on the physical examinations according to the locations of tears. Newly designed classification may help in deternmining the appropriate arthroscopic treatment of a partial thickness rotator cuff tear.
Keyword
Figure
-
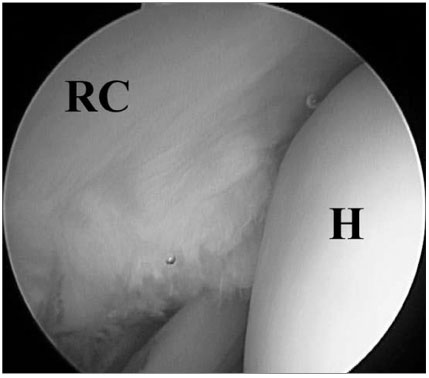
Fig. 1 Posterior arthroscopic view indicated fraying and fibrillations on the articular surface of the cuff. RC, rotator cuff; H, humeral head.

Fig. 2 Arthroscopic view of an articular surface of the cuff presented fiber disruption with displacement. H, humeral head; RC, rotator cuff.

Fig. 3 Arthroscopic image showing flap formation and fragmentation on articular side. RC, rotator cuff; H, humeral head.

Fig. 4 Arthroscopic image showing fragmentation on the bursal side of the rotator cuff. A, acromion; RC, rotator cuff.
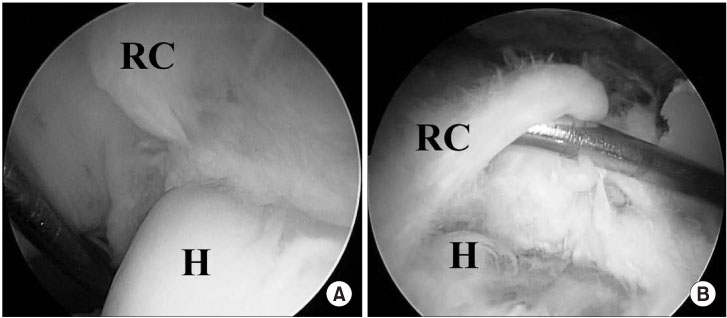
Fig. 5 Arthroscopic views revealed (A) displaced fiber disruption on the articular side of the cuff and (B) a large flap formation on bursal side of the cuff. RC, rotator cuff; H, humeral head.

Fig. 6 Arthroscopic finding demonstrated almost completely ruptured tendon fibers like full thickness tear with some fibers remaining in the middle layers of the cuff. (A) articular side and (B) bursal side. RC, rotator cuff; H, humeral head.
Reference
-
1. Bey MJ, Ramsey ML, Soslowsky LJ. Intratendinous strain fields of the supraspinatus tendon: effect of a surgically created articular-surface rotator cuff tear. J Shoulder Elbow Surg. 2002. 11:562–569.
Article2. Burkhart SS, Esch JC, Jolson RS. The rotator crescent and rotator cable: an anatomic description of the shoulder's "suspension bridge". Arthroscopy. 1993. 9:611–616.
Article3. Carpenter JE, Thomopoulos S, Flanagan CL, DeBano CM, Soslowsky LJ. Rotator cuff defect healing: a biomechanical and histologic analysis in an animal model. J Shoulder Elbow Surg. 1998. 7:599–605.
Article4. Ellman H. Diagnosis and treatment of incomplete rotator cuff tears. Clin Orthop Relat Res. 1990. 254:64–74.
Article5. Fukuda H. The management of partial-thickness tears of the rotator cuff. J Bone Joint Surg Br. 2003. 85:3–11.
Article6. Fukuda H, Hamada K, Yamanaka K. Pathology and pathogenesis of bursal-side rotator cuff tears viewed from en bloc histologic sections. Clin Orthop Relat Res. 1990. 254:75–80.
Article7. Huang CY, Wang VM, Pawluk RJ, et al. Inhomogeneous mechanical behavior of the human supraspinatus tendon under uniaxial loading. J Orthop Res. 2005. 23:924–930.
Article8. Jobe CM. Rotator cuff disorder: anatomy, function, pathogenesis and natural history. Orthopaedic knowledge update. 2002. Shoulder & Elbow, AAOS;143–154.9. Lee SB, Nakajima T, Luo ZP, Zobitz ME, Chang YW, An KN. The bursal and articular sides of the supraspinatus tendon have a different compressive stiffness. Clin Biomech (Bristol, Avon). 2000. 15:241–247.
Article10. Lehman RC, Perry CR. Arthroscopic surgery for partial rotator cuff tears. Arthroscopy. 2003. 19:E81–E84.
Article11. Lichtenberg S, Siebold R, Habermeyer P. Arthroscopic supraspinatus tendon repair using suture anchors and a modified Mason-Allen technique: an intra-articular approach. Arthroscopy. 2004. 20:1007–1011.
Article12. Lo IK, Burkhart SS. Transtendon arthroscopic repair of partial-thickness, articular surface tears of the rotator cuff. Arthroscopy. 2004. 20:214–220.
Article13. Luo ZP, Hsu HC, Grabowski JJ, Morrey BF, An KN. Mechanical environment associated with rotator cuff tears. J Shoulder Elbow Surg. 1998. 7:616–620.
Article14. MacDonald PB, Clark P, Sutherland K. An analysis of the diagnostic accuracy of the Hawkins and Neer subacromial impingement signs. J Shoulder Elbow Surg. 2000. 9:299–301.
Article15. Matava MJ, Purcell DB, Rudzki JR. Partial-thickness rotator cuff tears. Am J Sports Med. 2005. 33:1405–1417.
Article16. Murrell GA, Walton JR. Diagnosis of rotator cuff tears. Lancet. 2001. 357:769–770.
Article17. Nakajima T, Rokuuma N, Hamada K, Toomatsu T, Fukuda H. Histologic and biomechanical characteristics of the supraspinatus tendon: reference to rotator cuff tearing. J Shoulder Elbow Surg. 1994. 3:79–87.
Article18. Park HB, Yokota A, Gill HS, El Rassi G, McFarland EG. Diagnostic accuracy of clinical tests for the different degrees of subacromial impingement syndrome. J Bone Joint Surg Am. 2005. 87:1446–1455.
Article19. Reilly P, Amis AA, Wallace AL, Emery RJ. Mechanical factors in the initiation and propagation of tears of the rotator cuff. Quantification of strains of the supraspinatus tendon in vitro. J Bone Joint Surg Br. 2003. 85:594–599.20. Reilly P, Amis AA, Wallace AL, Emery RJ. Supraspinatus tears: propagation and strain alteration. J Shoulder Elbow Surg. 2003. 12:134–138.
Article21. Rhee YG. Strength weakness, anatomy and biomechanics. The shoulder: diagnosis and treatment. 2003. Yeong Chang Medical Books;157–162.22. Snyder SJ. Arthroscopic repair of articular supraspinatus tendon avulsions: PASTA lesion of the rotator cuff. Shoulder arthroscopy. 2003. 2nd ed. Lippincott Williams & Wilkins;219–229.23. Uhthoff HK, Sano H. Pathology of failure of the rotator cuff tendon. Orthop Clin North Am. 1997. 28:31–41.
Article24. Waibl B, Buess E. Partial-thickness articular surface supraspinatus tears: a new transtendon suture technique. Arthroscopy. 2005. 21:376–381.
Article25. Wakabayashi I, Itoi E, Sano H, et al. Mechanical environment of the supraspinatus tendon: a two-dimensional finite element model analysis. J Shoulder Elbow Surg. 2003. 12:612–617.
Article26. Yamaguchi K, Tetro AM, Blam O, Evanoff BA, Teefey SA, Middleton WD. Natural history of asymptomatic rotator cuff tears: a longitudinal analysis of asymptomatic tears detected sonographically. J Shoulder Elbow Surg. 2001. 10:199–203.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Comparative Study of MR-arthrography and Arthroscopy in Partial Thickness Rotator Cuff Tears
- Partial-thickness rotator cuff tears: a review of current literature on evaluation and management
- Partial-Thickness Tear of Supraspinatus and Infraspinatus Tendon Revisited: Based on MR Findings
- Current Concept of Management of Partial-thickness Rotator Cuff Tear
- Comparisons of the Various Partial-Thickness Rotator Cuff Tears on MR Arthrography and Arthroscopic Correlation
