A Newly Designed Nitinol Stent: Early Clinical Experience in the Treatment of Iliac Artery Stenoses and Occlusions
- Affiliations
-
- 1Department of Radiology, Seoul National University College of Medicine, Seoul, Korea. parkjh@radcom.snu.ac.kr
- KMID: 754099
- DOI: http://doi.org/10.3348/kjr.2001.2.3.145
Abstract
OBJECTIVE
To investigate the effectiveness of the newly designed Niti-S stent in the management of iliac arterial stenoses and occlusions. MATERIALS AND METHODS: Stenoses (n=25) or occlusions (n=5) in the iliac arteries of 25 patients (30 limbs) were treated. The site of the lesions was the common (n=15) or external (n=11) iliac artery, or both (n=4). Eight limbs were treated for diffuse disease, six for highly eccentric lesion, five for occlusive lesion, and 11 for failed angioplasty. RESULTS: In all patients, technical success was achieved without major complications. One death, not procedure-related, occurred within 30 days. Ankle-brachial indexes improved from 0.63 +/- 0.30 to 0.99 +/- 0.21, and ischemic symptoms showed improvement in 22 patients (88%). Fontaine classifications before stenting, namely IIa(n=3), IIb(n=16), III(n=2), and IV(n=4) improved to I(n=17), IIa(n=5), and IV(n=3). Follow-up over a 27 (mean, 19.8 +/- 8)-month period showed that cumulative patency rates were 95.8% at 1 year and 86.2% at 2 and 3 years. No significant decrease in the mean ankle-brachial index was observed. CONCLUSION: The Niti-S stent appears to be a safe and effective device for the treatment of iliac stenoses and occlusions. These preliminary results require confirmation with a larger series.
MeSH Terms
Figure
-
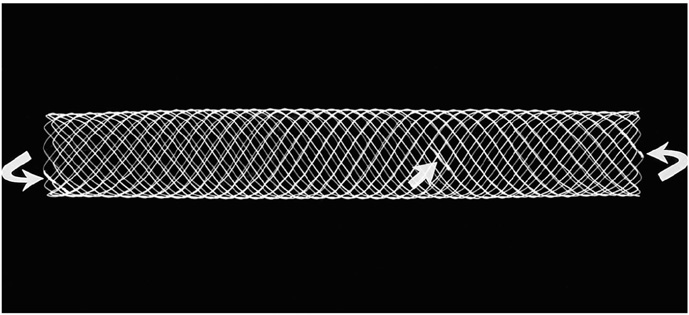
Fig. 1 The Niti-S consists of a monofilament nitinol wire wound on the mandrel in such a way that a series of interlacing wires creates a spiral mesh around its circumference. The distance between bends is approximately 2mm, and both ends of the wire are connected at the central portion of the stent (arrow). The leading and trailing ends of the stent are coated with platinum, which helps identify them and facilitates deployment (curved arrows).

Fig. 2 A. Pelvic angiogram obtained in a 68-year-old insulin dependent diabetic man with left-sided Fontaine stage-IIb claudication shows segmental occlusion of about 8cm involving the left common iliac artery, with opacification of the external iliac artery and numerous collateral channels. The translesional mean pressure gradient was 50 mmHg. B. Angiogram obtained after primary stent placement shows good patency of a previously occluded segment, and there is no residual pressure gradient across the lesion. During follow-up lasting 23 months, the patient was free of symptoms.
Reference
-
1. Murphy KD, Encarnacion CE, Le VA, Palmaz JC. Iliac artery stent placement with the Palmaz stent; follow-up study. J Vasc Interv Radiol. 1995. 6:321–329.2. Liermann D, Strecker EP, Peters J. The Strecker stent: indications and results in iliac and femoropopliteal arteries. Cardiovasc Intervent Radiol. 1992. 1:298–305.3. Murphy TP, Webb MS, Lambiase RE, et al. Percutaneous revascularization of complex iliac artery stenoses and occlusions with use of Wallstents: three-year experience. J Vasc Interv Radiol. 1996. 7:21–27.4. Yedlich JW, Ferral H, Bjarnason H, Hunter DW, Castaneda-Zuniga WR, Amplatz K. Chronic iliac artery occlusion: primary recanalization with endovascular stents. J Vasc Interv Radiol. 1994. 5:843–847.5. Bosch JL, Hunink MGM. Meta-analysis of the results of percutaneous transluminal angioplasty and stent placement for aortoiliac occlusive disease. Radiology. 1997. 204:87–96.6. Dotter CT, Buschmann RW, McKinney MK, Rosch J. Transluminal expandable nitinol coil stent grafting: preliminary report. Radiology. 1983. 147:259–260.7. Cragg AH, Dejong S, Barnhart W, Landas S, Smith TP. Preliminary evaluation of the Cragg stent (abstr). Radiology. 1992. 185(P):162.8. Cragg AH, Lund G, Rysavy JA, Salomonowitz E, Castaneda-Zuniga WR, Amplatz K. Percutaneous arterial grafting. Radiology. 1984. 150:45–49.9. Foelich JJ, Alfke H, Wilke A, et al. Effects of nitinol Strecker stent placement on vascular response in normal and stenotic porcine iliac arteries. J Vasc Interv Radiol. 1999. 10:329–338.10. Shaw JW. Management of aortoiliac occlusive vascular disease with the Memotherm self-expanding nitinol stent. J Intervent Radiol. 1996. 11:119–127.11. Maynar M, Reyes R, Ferral H, et al. Cragg endopro system I: early experience. I. Femoral arteries. J Vasc Interv Radiol. 1997. 8:203–207.12. Hausegger KA, Cragg AH, Lammer J, et al. Iliac artery stent placement: clinical experience with a nitinol stent. Radiology. 1994. 190:199–202.13. Wakloo AK, Tio FO, Lieber BB, et al. Self-expandable nitinol stents in canine vertebral arteries: hemodynamics and tissue response. Am J Neuroradiol. 1995. 16:1043–1051.14. Schwarzenberg H, Muller-Hulsbeck S, Gluer CC, Steffens JC, Heller M. Evaluation of maximum neointima proliferation and plaque morphology in iliac self-expanding nitinol stents with intravascular sonography. AJR. 1998. 171:1627–1630.15. Lee KW, Park JH, Chung JW, Kim WS, Lee W, Yeon KM. Short-term effects of a new intravascular nitinol stent in canine arteries. Invest Radiol. 1999. 34:367–373.16. Pentecost MJ, Criqui MH, Dorros G, et al. Guidelines for peripheral percutaneous transluminal angioplasty of the abdominal aorta and lower extremity vessels. Circulation. 1994. 89:511–531.17. Rutherford RB, Necker GJ. Standards for evaluating and reporting the results of surgical and percutaneous therapy for peripheral arterial disease. J Vasc Interv Radiol. 1991. 2:169.18. McLean GK, Cekirge S, Weiss JP, Foster RG. Stent placement for iliac artery occlusions: modified "wire-loop" technique with use of the goose-neck loop snare. J Vasc Interv Radiol. 1994. 5:701–703.19. Palmaz JC, Laborde JC, Rivera FJ, et al. Stenting of the iliac arteries with the Palmaz stent: experience from a multicenter trial. Cardiovasc Intervent Radiol. 1992. 15:291–297.20. Schurmann K, Vorwerk D, Kulisch A, et al. Neointimal hyperplasia in low-profile nitinol stents, Palmaz stents, and Wallstents: a comparative experimental study. Cardiovasc Intervent Radiol. 1996. 19:248–254.21. Ballard JL, Sparks SR, Taylor FC, et al. Complications of iliac artery stent deployment. J Vasc Surg. 1996. 24:545–555.22. Blum U, Gabelmann A, Redecker M, et al. Percutaneous recanalization of iliac artery occlusions: results of a prospective study. Radiology. 1993. 189:536–540.23. Laborde JC, Dougherty S, Rivera FJ, Encarnacion CE, Palmaz JC. Influence of anatomic distribution of atherosclerosis in the outcome of iliac revascularization (abstract). J Vasc Interv Radiol. 1992. 3:31.24. Stokes KR, Strunk HM, Campbell DR, Gibbons GW, Wheeler HG, Clouse ME. Five-year result in iliac and femoropopliteal angioplasty in diabetic patients. Radiology. 1990. 174:977–982.25. Gunther RW, Vorwerk D, Bohndorf K, Peters I, el-Din A, Messmer B. Iliac and femoral artery stenoses and occlusions: treatment with intravascular stents. Radiology. 1989. 172:725–730.26. Long AL, Page PE, Raynaud AC, et al. Percutaneous iliac artery stent: angiographic long-term follow-up. Radiology. 1991. 180:771–778.27. Fitzgerald GA. Dipyridamole. N Engl J Med. 1987. 316:1247–1257.28. Montalescot G. Value of antiplatelet therapy in preventing thrombotic events in generalized vascular disease. Clin Cardiol. 2000. 23:18–22.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Efficacy and Safety of a Newly Developed Self- Expanding Open-Cell Type Nitinol Stent for Peripheral Arteries: A Preclinical Study in Minipigs
- Endovascular Stent Placement for the Treatment of Superficial Femoral Artery Stenoses and Occlusions
- Placement of Balloon-Expandable Intraluminal Stent in Recurrent Iliac Artery Stenosis
- A Case of Complex Restenosis of Aortoiliac Stent Mimicking Downward Stent Migration
- Treatment of Malignant Gastroduodenal Obstruction with Using a Newly Designed Complex Expandable Nitinol Stent: Initial Experiences
