Comparison between Conventional MR Arthrograhphy and Abduction and External Rotation MR Arthrography in Revealing Tears of the Antero-Inferior Glenoid Labrum
- Affiliations
-
- 1Department of Radiology, College of Medicine, Korea University Guro Hospital. mgkim@sanggyepaik.or.kr
- 2Department of Radiology, Sanggye Paik Hospital, Inje University.
- 3Department of Radiology, Chung-Ju Hospital, Konkok University.
- KMID: 754091
- DOI: http://doi.org/10.3348/kjr.2001.2.4.216
Abstract
OBJECTIVE
To compare, in terms of their demonstration of tears of the anterior glenoid labrum, oblique axial MR arthrography obtained with the patient's shoulder in the abduction and external rotation (ABER) position, with conventional axial MR arthrography obtained with the patient's arm in the neutral position. MATERIALS AND METHODS: MR arthrography of the shoulder, including additional oblique axial sequences with the patient in the ABER position, was performed in 30 patients with a clinical history of recurrent anterior shoulder dislocation. The degree of anterior glenoid labral tear or defect was evaluated in both the conventional axial and the ABER position by two radiologists. Decisions were reached by consensus, and a three-point scale was used: grade 1=normal; grade 2=probable tear, diagnosed when subtle increased signal intensity in the labrum was apparent; grade 3=definite tear/defect, when a contrast material-filled gap between the labrum and the glenoid rim or deficient labrum was present. The scores for each imaging sequence were averaged and to compare conventional axial and ABER position scans, Student's t test was performed. RESULTS: In 21 (70%) of 30 patients, the same degree of anterior instability was revealed by both imaging sequences. Eight (27%) had a lower grade in the axial position than in the ABER position, while one (3%) had a higher grade in the axial position. Three whose axial scan was grade 1 showed only equivocal evidence of tearing, but their ABER-position scan, in which a contrast material-filled gap between the labrum and the glenoid rim was present, was grade 3. The average grade was 2.5 (SD=0.73) for axial scans and 2.8 (SD=0.46) for the ABER position. The difference between axial and ABER-position scans was statistically significant (p<0.05). CONCLUSION: MR arthrography with the patient's shoulder in the ABER position is more efficient than conventional axial scanning in revealing the degree of tear or defect of the anterior glenoid labrum. When equivocal features are seen at conventional axial MR arthrography, oblique axial imaging in the ABER position is helpful.
Keyword
MeSH Terms
Figure
-
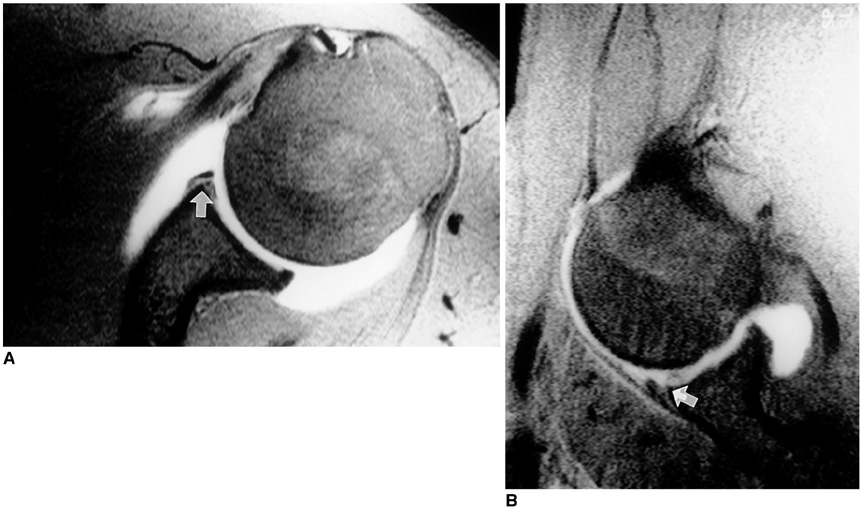
Fig. 1 In a 20-year-old man with a history of recurrent anterior shoulder dislocation, a grade-2 anterior glenoid labral tear is revealed by both axial and abduction and external rotation images. A. Axial fat-suppressed T1-weighted MR arthrogram reveals subtle increased signal intensity in the anterior glenoid labrum (arrow). B. Abduction and external rotation oblique axial fat-suppressed T1-weighted MR arthrogram of this same region shows similar findings (arrow).
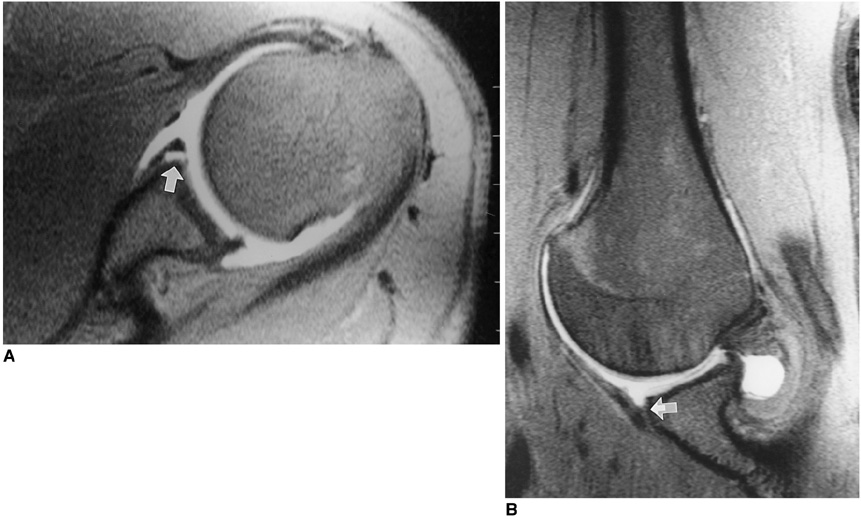
Fig. 2 In a 24-year-old man with a history of recurrent anterior shoulder dislocation, a grade-3 anterior glenoid labral tear is seen on both axial and abduction and external rotation images. A. Axial fat-suppressed T1-weighted MR arthrogram shows contrast material filling the tear (arrow) in the anterior glenoid labrum. B. Abduction and external rotation oblique axial fat-suppressed T1-weighted MR arthrogram also reveals contrast material filling the gap between the anterior glenoid labrum and glenoid rim, showing a Bankart lesion (arrow).
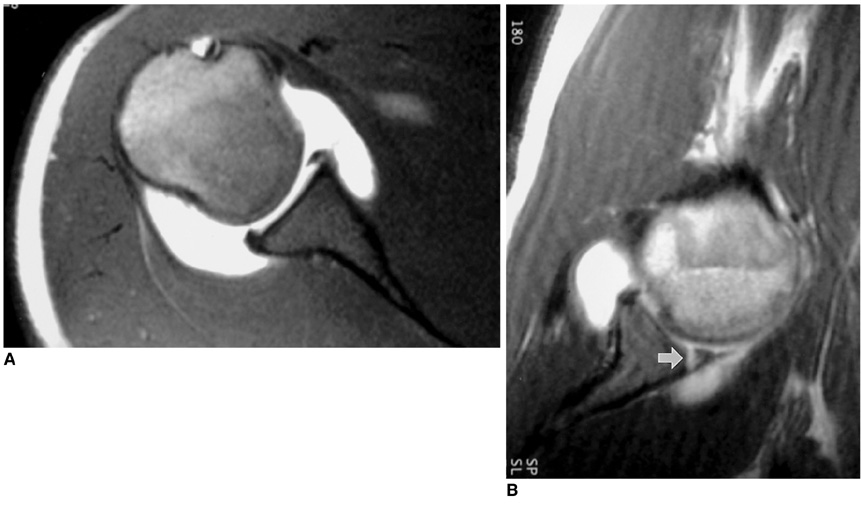
Fig. 3 In a 20-year-old man with a history of recurrent anterior shoulder dislocation, axial scanning demonstrates a grade-2 anterior glenoid labral tear. Abduction and external rotation scanning, however, indicates that this is grade 3. A. Axial fat-suppressed T1-weighted MR arthrogram shows slightly increased signal intensity of the anterior glenoid labrum. B. Abduction and external rotation oblique axial fat-suppressed T1-weighted MR arthrogram reveals a contrast material-filled gap between the labrum and the glenoid rim (arrow).

Fig. 4 In a 19-year-old man with a history of recurrent anterior shoulder dislocation, axial scanning demonstrates a grade-1 anterior glenoid labral tear, but an abduction and external rotation-position scan indicates that this is grade 3. A. On this axial fat-suppressed T1-weighted MR arthrogram, the presence of an anterior glenoid labrum tear is seen. B. Abduction and external rotation oblique axial fat-suppressed T1-weighted MR arthrogram reveals detached labral tear with periosteal stripping (arrow).
Reference
-
1. Mohtadi NG. Advances in the understanding of anterior instability of the shoulder. Clin Sports Med. 1991. 10:863–870.2. Chandnani VP, Gagliardi JA, Murnane TG, et al. Glenohumeral ligaments and shoulder capsular mechanism: evaluation with MR arthrography. Radiology. 1995. 196:27–32.3. Chandnani VP, Yeager TD, DeBerardino T, et al. Glenoid labral tears: prospective evaluation with MR imaging, MR arthrography, and CT arthrography. AJR. 1993. 161:1229–1235.4. Zlatkin MB, Iannotti JP, Esterhai JL, et al. Evaluation of rotator cuff disease and glenohumeral instability with MR imaging: correlation with arthroscopy and arthrotomy in a large population of patients (abstr.). Magn Reson Imaging. 1990. 8:S. 78.5. Legan JM, Burkhard TK, Goff WB II, et al. Tears of the glenoid labrum: MR imaging of 88 arthroscopically confirmed cases. Radiology. 1991. 179:241–246.6. Gusmer PB, Potter HG, Schatz JA, et al. Labral injuries: accuracy of detection with unenhanced MR imaging of the shoulder. Radiology. 1996. 200:519–524.7. Seeger LL, Gold RH, Bassett LW. Shoulder instability: evaluation with MR imaging. Radiology. 1988. 168:695–697.8. Liu SH, Henry MH, Nuccion S, Shapiro MS, Dorey F. Diagnosis of glenoid labral tear: comparison between magnetic resonance imaging and clinical examinations. Am J Sports Med. 1996. 24:149–154.9. Green MR, Christensen KP. Magnetic resonance imaging of the glenoid labrum in anterior instability. Am J Sports Med. 1994. 22:493–498.10. Imhoff A, Hodler J. Arthroscopy and MRI of the shoulder: a comparative retrospective analysis. Z Orthrop Ihre Grenzgeb. 1992. 13:188–196.11. McCauley TR, Pope CF, Jokl P. Normal and abnormal glenoid labrum: assessment with multiplanar gradient-echo imaging. Radiology. 1992. 183:35–37.12. Palmer WE, Brown JH, Rosenthal DI. Labral-ligamentous complex of the shoulder: evaluation with MR arthrography. Radiology. 1994. 190:645–651.13. Willemsen UF, Wiedemann E, Brunner U, et al. Prospective evaluation of MR arthrography performed with high-volume intraarticular saline enhancement in patients with recurrent anterior dislocations of the shoulder. AJR. 1998. 170:79–84.14. Kwak SM, Brown RR, Trudell D, Resnick D. Glenohumeral joint: comparison of shoulder positions at MR arthrography. Radiology. 1998. 208:375–380.15. Cvitanic O, Tirman PFJ, Feller JF, Bost FW, Minter J, Carroll KW. Using abduction and external rotation of the shoulder to increase the sensitivity of MR arthrography in revealing tears of the anterior glenoid labrum. AJR. 1997. 169:837–844.16. Tirman PFJ, Applegate GR, Flannigan BD, Stauffer AE, Crues JV III. Magnetic resonance arthrography of the shoulder. Magn Reson Imaging Clin N Am. 1993. 1:125–142.17. Tirman PFJ, Bost FW, Steinbach LS, et al. MR arthrographic depiction of tears of the rotator cuff: benefit of abduction and external rotation of the arm. Radiology. 1994. 192:851–856.18. Kaplan PA, Bryans KC, Davick JP, Otte M, Stinson WW, Dussault RG. MR imaging of the normal shoulder: variants and pitfalls. Radiology. 1992. 184:519–524.19. Flannigan B, Kursunoglu-Brahme S, Snyder S, Karzel R, Del Pizzo W, Resnick D. MR arthrography of the shoulder: comparison with conventional MR imaging. AJR. 1990. 155:829–832.20. Tirman RM, Janecki CJ, Eubanks RG, Nelson CL. Shoulder arthrography. Contemp Orthop. 1970. 1:26.21. Tirman PFJ, Stauffer AE, Crues JV, Turner RM, Schobert WE, Nottage WM. Saline MR arthrography in the evaluation of glenohumeral instability. Arthroscopy. 1993. 9:141–146.22. Palmer WE, Caslowitz PL, Chew FS. MR arthrography of the shoulder: normal intraarticular structures and common abnormalities. AJR. 1995. 164:141–146.23. Palmer WE, Caslowitz PL. Anterior shoulder instability: diagnostic criteria determined from prospective analysis of 121 MR arthrograms. Radiology. 1995. 197:819–825.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Arthrosonography of the Shoulder Joint for Evaluation of the Glenoid Labrum, Glenoid Rim and Humeral Head: Comparison with Conventional Ultrasonography and MR Arthrography
- Comparison of Shoulder Positions at MR Arthrography: Change of Labroligamentous Complex Shape and Diagnosis of Labral Tears
- Feasibility of Ultrasonography and MR Arthrography during Evaluation of Rotator Cuff Injury
- Comparative Study of MR-arthrography and Arthroscopy in Partial Thickness Rotator Cuff Tears
- Ankle Ligaments: Comparison of MR Arthrography with Conventional MR Imaging in Amputated Feet
