Role of CT Venography in the Diagnosis and Treatment of Benign Thoracic Central Venous Obstruction
- Affiliations
-
- 1Department of Radiology, Seoul National University College of Medicine; Institute of Radiation Medicine, SNUMRC; and Clinical Research Institute, Seoul National University Hospital. chungjw@radcom.snu.ac.kr
- KMID: 754017
- DOI: http://doi.org/10.3348/kjr.2003.4.3.146
Abstract
OBJECTIVE
To evaluate the role of CT venography in the diagnosis and treatment of benign thoracic central venous obstruction. MATERIALS AND METHODS: Eighteen patients who had undergone both CT venography and digital subtraction venography were prospectively enrolled in this study. The following features were analyzed by two observers: the cause, degree, and extent of venous obstruction; associated thrombosis; and implications for the planning of treatment. CT venography and digital subtraction venography were compared in defined venous segments, and the degree of obstruction, and correlation was expressed using Spearman's rank correlation coefficient. RESULTS: In all patients, CT venography depicted the causes of obstruction, including extrinsic compression of the left brachiocephalic vein, and mediastinal inflammatory pseudotumor. Interobserver agreement regarding classification of the degree of obstruction was judged as good for CT venography (k=0.864), and in evaluating this, there was significant correlation between CT venography and digital subtraction venography (reader 1: Rs = 0.58, p < 0.01; reader 2: Rs = 0.56, p < 0.01). In evaluating the status of central veins proximal to long segmental obstruction, and associated thrombosis, CT venography was superior to digital subtraction venography. In half of all patients, the findings of CT venography led to changes in the treatment plan. CONCLUSION: The findings of CT venography correlated closely with those of digital subtraction venography, and the former accurately depicted the degree and extent of benign venous obstruction.
Keyword
Figure
-
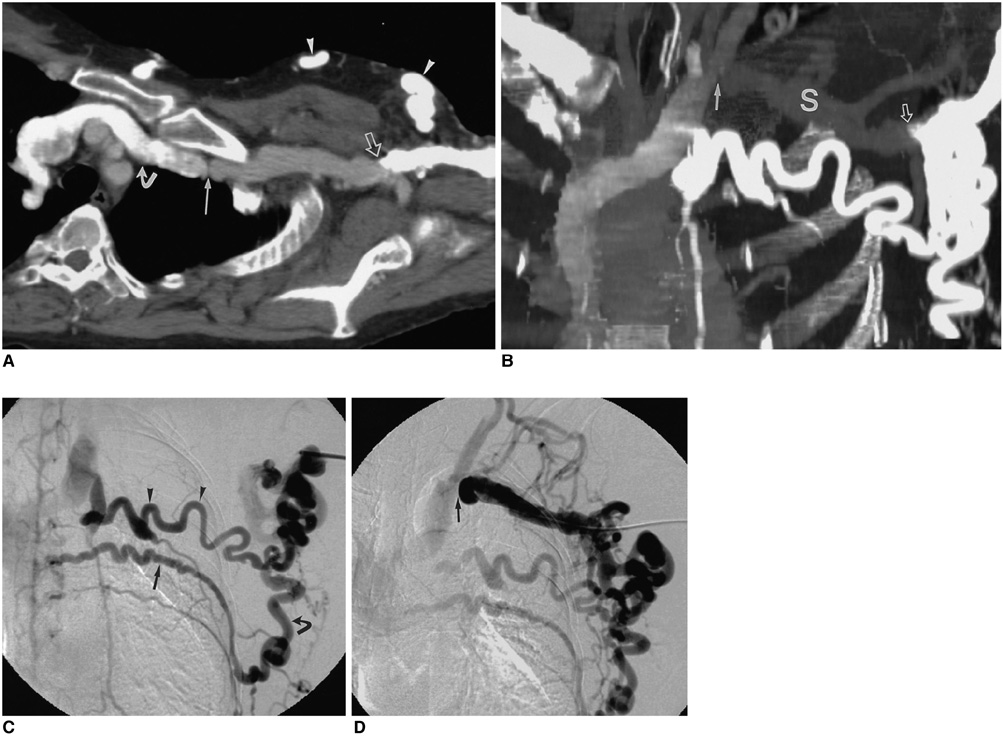
Fig. 1 Complete occlusion of the left subclavian vein occurring at ipsilateral contrast material injection. A. Curved planar reformation image demonstrates membranous obstruction of the proximal portion of the left subclavian vein (arrow). Reader 1 interpreted this as severe stenosis, and reader 2 as occlusion. The brachial vein, thoracoepigastric vein (arrowheads), and left brachiocephalic vein (curved arrow) are clearly enhanced, whereas the subclavian vein and axillary vein show only slight enhancement. Because the collateral circulation bypassed the occluded subclavian vein, no obstructive lesion was seen in the left axillary vein at the abrupt transition in contrast enhancement (open arrow). B. Oblique coronal thin-slab maximum-intensity-projection image obtained after segmentation of the left clavicle and first rib reveals membranous obstruction (arrow) of the proximal portion of the left subclavian vein and faint enhancement of this vein (S). The injected contrast material drained into the left brachiocephalic vein through the lateral thoracic and thoracoepigastric vein (open arrow), and this explains the lesser degree of contrast enhancement of the left subclavian vein. C. Digital subtraction venography performed with the catheter tip in the left axillary vein depicts the thoracoepigastric vein (arrowheads), lateral thoracic vein (curved arrow), posterior intercostal vein (arrow), and left brachiocephalic vein. The left subclavian vein and proximal axillary vein are not opacified, so the level of stenosis can be mistaken for the mid-portion of the axillary vein. D. Digital subtraction venography with the catheter tip placed just before the obstructing membrane in the left subclavian vein demonstrates complete occlusion (arrow) of the left subclavian vein. The left brachiocephalic vein beyond the obstruction is opacified by collateral circulation via the left external jugular vein. The left axillary vein is widely patent.
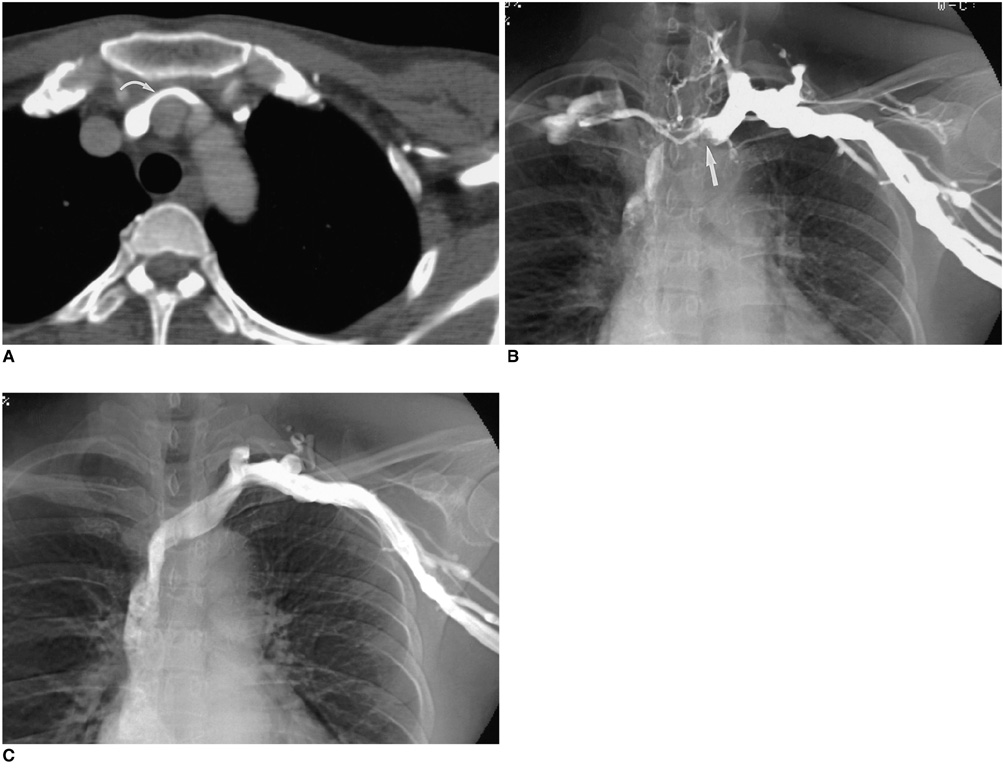
Fig. 2 Dynamic obstruction of the left brachiocephalic vein due to extrinsic compression. A. Transverse CT scan obtained during inspiration after ipsilateral contrast material injection shows a moderate degree of stenosis (curved arrow) in the left brachiocephalic vein due to extrinsic compression between the right brachiocephalic artery and sternum. B. Digital subtraction venography at expiration reveals complete occlusion of the left brachiocephalic vein (arrow), and prominent collateral veins. C. Digital subtraction venography at inspiration demonstrates restoration of blood flow through the left brachiocephalic vein, without the involvement of collateral veins. This phenomenon indicates that according to the point reached in the respiration cycle, extrinsic compression of the left brachiocephalic vein between the arch vessels and the sternum exaggerated at inspiration, can cause dynamic obstruction.

Fig. 3 Focal stenosis of the left subclavian vein hidden behind overlapping collateral veins. A. Transverse thin-slab maximum-intensity-projection image obtained after segmentation of the left clavicle and first rib reveals severe stenosis of the left subclavian vein (arrow). Note the presence of a large overlying collateral vein (arrowhead). B. Volume-rendering image in frontal projection shows that the stenotic portion of the left subclavian vein is hidden behind the collateral vein (arrow). C. Volume-rendering image obtained at craniocaudal angulation reveals stenosis (arrow). D. At digital subtraction venography, it is difficult to recognize significant stenosis in the left subclavian vein. The prominence of the collateral veins, however, suggests the presence of hemodynamically significant stenosis. E. Digital subtraction venography performed after the catheter tip placed in the left subclavian vein has revealed severe focal stenosis (arrow) of the left subclavian vein.
Cited by 1 articles
-
MDCT Application in the Vascular System
Hwan Seok Yong
J Korean Med Assoc. 2007;50(1):25-32. doi: 10.5124/jkma.2007.50.1.25.
Reference
-
1. Yim CD, Sane SS, Bjarnason H. Superior vena cava stenting. Radiol Clin North Am. 2000. 38:409–424.2. Parish JM, Marschke RF Jr, Dines DE, Lee RE. Etiologic considerations in superior vena cava syndrome. Mayo Clin Proc. 1981. 56:407–413.3. Qanadli SD, el-Hajjam M, Bruckert F, et al. Helical CT phlebography of the superior vena cava: diagnosis and evaluation of venous obstruction. AJR Am J Roentgenol. 1999. 172:1327–1333.4. Glanz S, Gordon DH, Lipkowitz GS, Butt KM, Hong J, Sclafani SJ. Axillary and subclavian vein stenosis: percutaneous angioplasty. Radiology. 1988. 168:371–373.5. Schwab SJ, Quarles LD, Middleton JP, Cohan RH, Saeed M, Dennis VW. Hemodialysis-associated subclavian vein stenosis. Kidney Int. 1988. 33:1156–1159.6. Surratt RS, Picus D, Hicks ME, Darcy MD, Kleinhoffer M, Jendrisak M. The importance of preoperative evaluation of the subclavian vein in dialysis access planning. AJR Am J Roentgenol. 1991. 156:623–625.7. el-Shahawy MA, Gadallah MF, Teitelbaum GP, Kaptein E, Akmal M. Compression of the left brachiocephalic vein by the innominate artery resulting in massive arm edema in a hemodialysis patient. Am J Nephrol. 1992. 12:108–110.8. Glanz S, Gordon DH, Butt KM, Hong J, Lipkowitz GS. The role of percutaneous angioplasty in the management of chronic hemodialysis fistulas. Ann Surg. 1987. 206:777–781.9. Gray RJ, Horton KM, Dolmatch BL, et al. Use of Wallstents for hemodialysis access-related venous stenoses and occlusions untreatable with balloon angioplasty. Radiology. 1995. 195:479–484.10. Haage P, Vorwerk D, Piroth W, Schuermann K, Guenther RW. Treatment of hemodialysis-related central venous stenosis or occlusion: results of primary Wallstent placement and follow-up in 50 patients. Radiology. 1999. 212:175–180.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Spiral CT Venography in Central Venous Obstruction
- Central Venous Catheter Induced Thrombotic Obstruction of the Superior Vena Cava
- Significance of Contrast Enhanced Rapid MR Sequence(True FISP) in Deep Vein Thrombosis
- The Interobserver Agreement between Residents and Experienced Radiologists for Detecting Pulmonary Embolism and DVT with Using CT Pulmonary Angiography and Indirect CT Venography
- Reassessment of the Diagnostic Role of Technetium-99m-RBC Venography for Leg Venous Diseases
