Kosin Med J.
2024 Dec;39(4):294-298. 10.7180/kmj.24.115.
Idiopathic pneumoperitoneum diagnosed and treated differently in preterm infants: two case reports
- Affiliations
-
- 1Department of Pediatrics, Pusan National University Hospital, Pusan National University School of Medicine, Busan, Korea
- KMID: 2562814
- DOI: http://doi.org/10.7180/kmj.24.115
Abstract
- Pneumoperitoneum that develops in the absence of a perforated abdominal viscus and does not require laparotomy is considered to be idiopathic. Differentiating between idiopathic pneumoperitoneum and highly lethal perforation due to necrotizing enterocolitis in preterm infants is important. Herein, we report two cases of idiopathic pneumoperitoneum in preterm infants who underwent exploratory laparotomy and conservative treatment, respectively. The first patient was born at 32+5 weeks of gestation and developed pneumoperitoneum on day 7 of life. The patient underwent exploratory laparotomy and was diagnosed with idiopathic pneumoperitoneum after surgery. The second patient was born at 30 weeks of gestation. He developed pneumoperitoneum on the eighth day of life. Idiopathic pneumoperitoneum was suspected, and the patient was treated conservatively without laparotomy. Based on our awareness and experience of the first case of idiopathic pneumoperitoneum, we were able to treat the second patient conservatively. These cases will be helpful for diagnosing and treating pneumoperitoneum in preterm infants.
Keyword
Figure
-
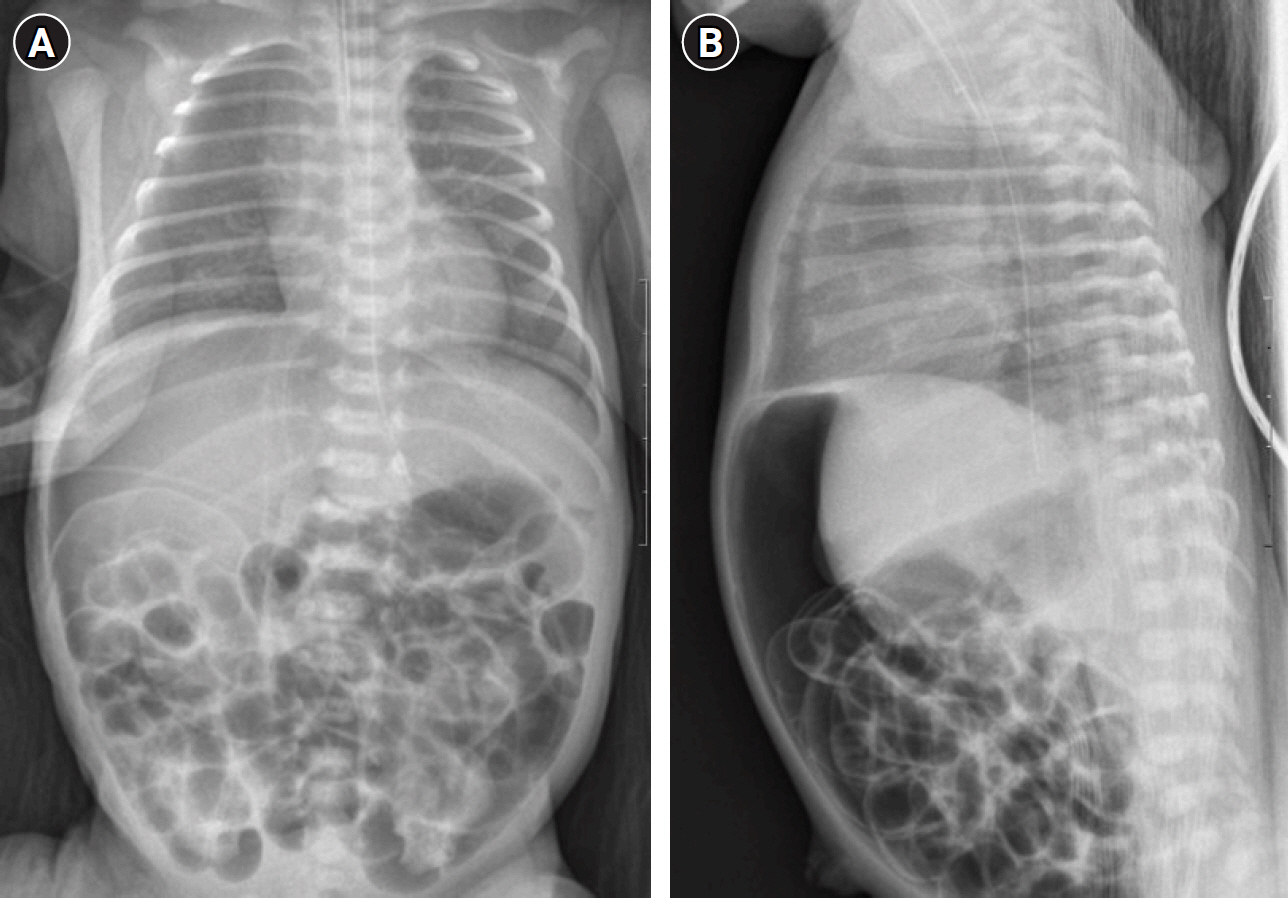
Fig. 1. Plain abdominal X-ray showing free peritoneal air occupying the entire abdomen in patient 1. (A) Supine view. (B) Lateral view.
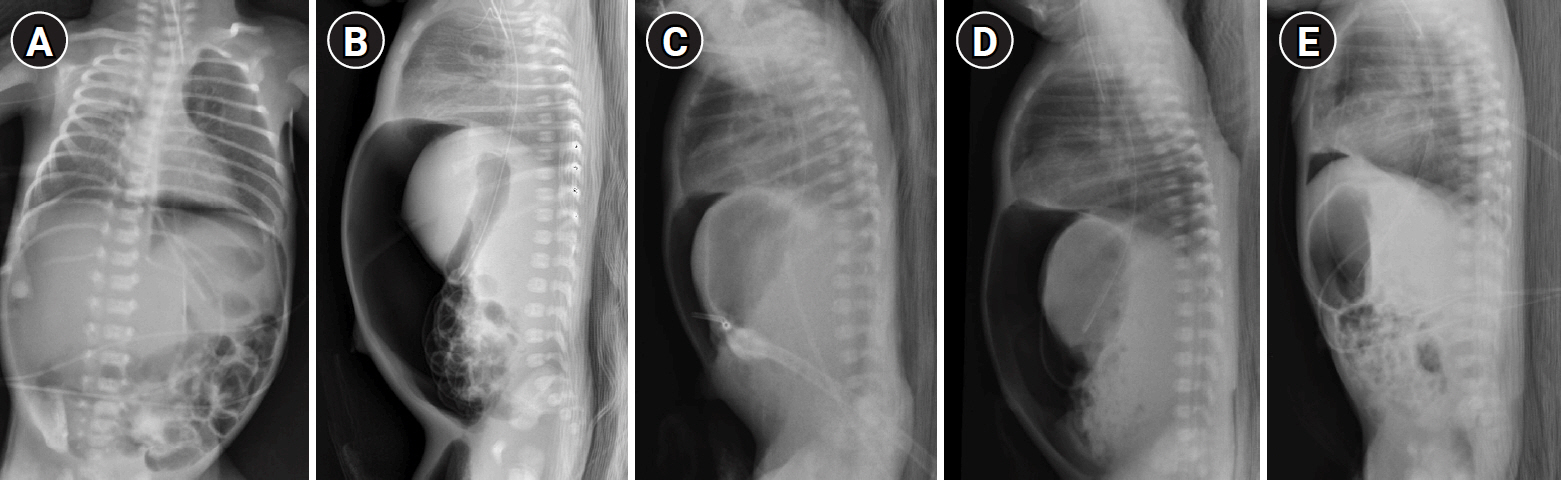
Fig. 2. Plain abdominal X-ray showing free air in patient 2. (A, B) Day of pneumoperitoneum onset. (C) Three days after onset, a lateral abdominal X-ray showed decreased pneumoperitoneum. (D) Four days after onset, pneumoperitoneum worsened after feeding. (E) Eight days after onset, the free air had nearly resolved.
Reference
-
References
1. Abdelmohsen SM, Osman MA. Idiopathic neonatal pneumoperitoneum, a case report. Int J Surg Case Rep. 2017; 31:250–3.
Article2. Gutkin Z, Iellin A, Meged S, Sorkine P, Geller E. Spontaneous pneumoperitoneum without peritonitis. Int Surg. 1992; 77:219–23.3. Duan SX, Sun ZB, Wang GH, Zhong J, Ou WH, Fu MX, et al. Diagnosis and treatment of pediatric benign pneumoperitoneum: a case report series of 9 patients. Medicine (Baltimore). 2017; 96:e5814.4. Karaman A, Demirbilek S, Akin M, Gurunluoglu K, Irsi C. Does pneumoperitoneum always require laparotomy? Report of six cases and review of the literature. Pediatr Surg Int. 2005; 21:819–24.
Article5. McLaren O. Spontaneous idiopathic recurrent pneumoperitoneum. J Surg Case Rep. 2013; 2013:rjt071.
Article6. Mularski RA, Ciccolo ML, Rappaport WD. Nonsurgical causes of pneumoperitoneum. West J Med. 1999; 170:41–6.7. Gupta R, Bihari Sharma S, Golash P, Yadav R, Gandhi D. Pneumoperitoneum in the newborn: is surgical intervention always indicated? J Neonatal Surg. 2014; 3:32.
Article8. He TZ, Xu C, Ji Y, Sun XY, Liu M. Idiopathic neonatal pneumoperitoneum with favorable outcome: a case report and review. World J Gastroenterol. 2015; 21:6417–21.
Article9. Park J, Jung E. Spontaneous pneumoperitoneum in two extremely preterm infants during nasal intermittent positive pressure ventilation. Pediatr Int. 2019; 61:424–5.
Article10. Song JH. Idiopathic pneumoperitoneum in a premature infant. Soonchunhyang Med Sci. 2016; 22:71–4.
Article11. Khan TR, Rawat JD, Ahmed I, Rashid KA, Maletha M, Wakhlu A, et al. Neonatal pneumoperitoneum: a critical appraisal of its causes and subsequent management from a developing country. Pediatr Surg Int. 2009; 25:1093–7.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Idiopathic Pneumoperitoneum in a Premature Infant
- A Case of Spontaneous Pneumoperitoneum Associated with Idiopathic Intestinal Pseudoobstruction
- Comparison of gastric and other bowel perforations in preterm infants: a review of 20 years' experience in a single institution
- Scrotal Abscess Following Emergency Laparotomy in a Preterm Infant
- Clinical Characteristics of Apnea in Full-Term Infants: Compared to Late Preterm Infants
