Feasibility of navigation-assisted endoscopic transnasal optic nerve decompression for the treatment of traumatic optic neuropathy in patients with midfacial fractures
- Affiliations
-
- 1Departments of Oral and Maxillofacial Surgery, Shimane University Faculty of Medicine, Izumo, Japan
- 2Departments of Otorhinolaryngology-Head and Neck Surgery, Shimane University Faculty of Medicine, Izumo, Japan
- 3Department of Maxillofacial Diagnostic and Surgical Science, Kagoshima University, Kagoshima, Japan
- KMID: 2560823
- DOI: http://doi.org/10.5125/jkaoms.2024.50.5.273
Abstract
Objectives
Traumatic optic neuropathy (TON), a relatively rare condition, can cause visual functional impairment and permanent functional damage.Surgeons should be familiar with its diagnostic criteria and treatment to effectively manage cases of facial trauma with TON. We investigated the feasibility of navigation-assisted endoscopic trans-nasal optic nerve decompression (ETOND) to treat TON in maxillofacial trauma patients.
Patients and Methods
We retrospectively analyzed data from the clinical investigation of four consecutive patients, two males and two females with an average age of 75 years, with midfacial fractures and TON between April 2021 and September 2023. All patients had swelling and subcutaneous periorbital hemorrhage accompanied by optic nerve canal and zygomaticomaxillary complex fractures on the affected side. Three patients had lacerations on the lateral eyebrow or upper eyelid. All patients were evaluated by an ophthalmologist for visual impairment; two patients could see hand motion at a 30 cm distance, one patient could perceive light, and one did not have any loss of visual acuity. Among the four patients, three had visual impairment immediately after the injury, and one showed delayed impairment.
Results
The patients were treated with navigation-assisted ETOND conducted by an endoscopic rhinologist. Three of the ETONDs were performed along with open reduction and internal fixation (ORIF); the other ETOND was delayed. Orbital reconstruction was performed in three patients. Steroid therapy was administered to two patients, one pre-operatively and one post-operatively. The two patients with pre-operative vision loss showed improved visual acuity post-operatively, and the two patients with no pre-operative visual impairment had no vision loss associated with ORIF for their midfacial fractures. No patient had post-operative complications.
Conclusion
Navigation-assisted ETOND can be performed easily by endoscopic rhinologists; and prompt examination, diagnosis, and treatment are important in patients with facial trauma and TON.
Keyword
Figure
-
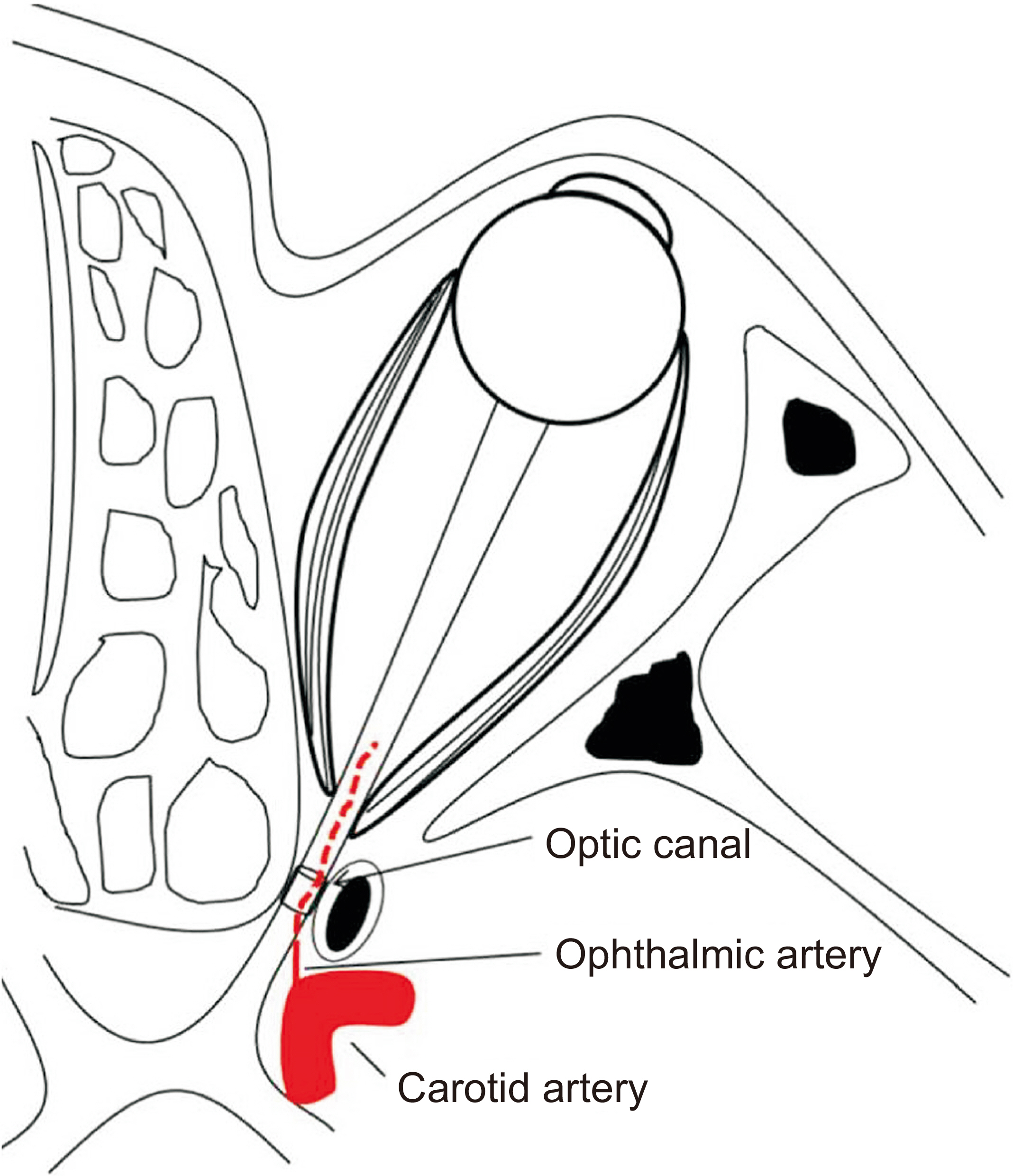
Fig. 1 The anatomical relationships among the structures surrounding the optic nerve.

Fig. 2 Pre-operative computed tomography (CT) findings of Patient #1. A, B. Axial and coronal CT images showing a fracture of the lateral wall of the left optic nerve canal. The bone fragment compresses the left optic nerve within the nerve canal (yellow arrows). C, D. Coronal and three-dimensional CT images showing naso-orbito-ethmoid type I fracture, left zygomaticomaxillary complex fracture, and inferior wall fracture of the left orbit (yellow arrow).

Fig. 3 Surgical view of Patient #1. A. During navigation-assisted endoscopic trans-nasal optic nerve decompression performed by an endoscopic rhinologist, a depressed bone fragment was identified in the distal part of the optic canal. B. Depressed bone fragments were filed. C. Decompression of the optic nerve canal was performed. The optic nerve sheath (white arrow) was visualized after bone removal. D. open reduction and internal fixation (ORIF) of midfacial fractures; the left zygomaticomaxillary complex fractures were treated by ORIF with a hemi-coronal incision approach. E. Bone was harvested from the anterior wall of the maxillary sinus. F. The harvested bone was shaped according to the morphology of the left orbital floor. G. The orbital floor was reconstructed using the harvested bone and fixed with micro-titanium screws.

Fig. 4 Post-operative computed tomography (CT) findings of Patient #1. A. Axial CT showing removal and release of the bone fragments around the optic nerve canal (yellow arrow). B-D. Three-dimensional CT shows that the midfacial fracture, including orbital morphology, was adequately reconstructed (yellow arrows).

Fig. 5 Computed tomography (CT) findings and surgical view of Patient #2. A, B. Axial and coronal pre-operative CT showing a fracture of the lateral wall of the left optic nerve canal. A bone fragment was compressing the left optic nerve within the nerve canal (yellow arrows). C, D. Axial and three-dimensional pre-operative CT showing a left zygomaticomaxillary complex fracture with medial displacement of bone fragments. E. During navigation-assisted endoscopic trans-nasal optic nerve decompression performed by an endoscopic rhinologist, a depressed bone fragment was identified in the distal part of the optic nerve canal. F. Bone fragment removal. G, H. Axial and coronal post-operative CT showing the removal and release of the bone fragments around the optic nerve canal (yellow arrows). I. Three-dimensional post-operative CT shows that the zygomatic fragment was repositioned symmetrically.

Fig. 6 Pre-operative computed tomography (CT) findings of Patient #3. A. Axial CT showing a fracture of the frontal bone. B. Axial CT showing a fracture of the left zygomaticomaxillary complex. C, D. Coronal and axial CT showing a left type IV blowout fracture, medial orbital wall fracture, and optic nerve canal fracture (yellow arrow). E. Three-dimensional CT showing fracture of the frontal bone, a type I left naso-orbito-ethmoid fracture, and a left zygomaticomaxillary complex fracture.

Fig. 7 Surgical view of Patient #3. A. ORIF of the midfacial fractures, frontal bone fracture, and left zygomaticomaxillary complex fracture were treated by ORIF with a bi-coronal incision. B. The zygomaticomaxillary buttress and the nasomaxillary buttress were treated by ORIF through an oral vestibular incision. C. The infraorbital rim was treated by ORIF through a sub-tarsal incision. D. The bone used for orbital floor reconstruction was harvested from the parietal exostosis. E. Workflow based on intra-operative CT to update the navigation system and navigation-assisted ETOND and intra-operative CT imaging using mobile-type cone-beam CT (3D Accuitomo M, Morita). F. Registration of the navigation system (Stealth Station ENT) using intraoperatively acquired CT data. G. Screen view during registration to the navigation system. H. Navigation-assisted ETOND by an endoscopic rhinologist. I. During the navigation-assisted ETOND performed by the endoscopic rhinologist, the posterior wall of the posterior ethmoid sinus was removed to gain access to the sphenoid sinuses (black arrows). J. Optic prominence (white arrow) with a view of the sphenoid sinus. (ORIF: open reduction and internal fixation, CT: computed tomography, ETOND: endoscopic trans-nasal optic nerve decompression)

Fig. 8 Post-operative computed tomography (CT) findings of Patient #3. A, B. Three-dimensional construction and coronal CT showing that the midfacial fracture, including orbital morphology, were adequately reconstructed. C. Axial CT showing release of the bone on the medial side of the optic nerve canal (yellow arrow).
Reference
-
References
1. Chen B, Zhang H, Zhai Q, Li H, Wang C, Wang Y. 2022; Traumatic optic neuropathy: a review of current studies. Neurosurg Rev. 45:1895–913. https://doi.org/10.1007/s10143-021-01717-9. DOI: 10.1007/s10143-021-01717-9. PMID: 35034261.
Article2. Gupta D, Gadodia M. 2018; Transnasal endoscopic optic nerve decompression in post traumatic optic neuropathy. Indian J Otolaryngol Head Neck Surg. 70:49–52. https://doi.org/10.1007/s12070-017-1211-5. DOI: 10.1007/s12070-017-1211-5. PMID: 29456943. PMCID: PMC5807297.
Article3. Yan W, Chen Y, Qian Z, Selva D, Pelaez D, Tu Y, et al. 2017; Incidence of optic canal fracture in the traumatic optic neuropathy and its effect on the visual outcome. Br J Ophthalmol. 101:261–7. https://doi.org/10.1136/bjophthalmol-2015-308043. DOI: 10.1136/bjophthalmol-2015-308043. PMID: 27267448.
Article4. Xu R, Chen F, Zuo K, Ye X, Yang Q, Shi J, et al. 2014; Endoscopic optic nerve decompression for patients with traumatic optic neuropathy: is nerve sheath incision necessary? ORL. 76:44–9. https://doi.org/10.1159/000358305. DOI: 10.1159/000358305. PMID: 24713993.
Article5. Sasindran V, John MS. 2022; Endoscopic optic nerve decompression for direct traumatic optic neuropathy: our 10 years experience. Indian J Otolaryngol Head Neck Surg. 74:594–9. https://doi.org/10.1007/s12070-022-03194-y. DOI: 10.1007/s12070-022-03194-y. PMID: 36514422. PMCID: PMC9741668.
Article6. Tabatabaei SA, Soleimani M, Alizadeh M, Movasat M, Mansoori MR, Alami Z, et al. 2011; Predictive value of visual evoked potentials, relative afferent pupillary defect, and orbital fractures in patients with traumatic optic neuropathy. Clin Ophthalmol. 5:1021–6. https://doi.org/10.2147/OPTH.S21409. DOI: 10.2147/OPTH.S21409. PMID: 21845028. PMCID: PMC3151564.
Article7. Urolagin SB, Kotrashetti SM, Kale TP, Balihallimath LJ. 2012; Traumatic optic neuropathy after maxillofacial trauma: a review of 8 cases. J Oral Maxillofac Surg. 70:1123–30. https://doi.org/10.1016/j.joms.2011.09.045. DOI: 10.1016/j.joms.2011.09.045. PMID: 22177813.
Article8. Bodanapally UK, Shanmuganathan K, Katzman L, Geraymovych E, Saksobhavivat N, et al. Van der Byl G. 2014; Traumatic optic neuropathy prediction after blunt facial trauma: derivation of a risk score based on facial CT findings at admission. Radiology. 272:824–31. https://doi.org/10.1148/radiol.14131873. DOI: 10.1148/radiol.14131873. PMID: 24758554.
Article9. Zhao X, Jin M, Xie X, Ye P, He S, Duan C, et al. 2022; Vision improvement in indirect traumatic optic neuropathy treated by endoscopic transnasal optic canal decompression. Am J Otolaryngol. 43:103453. https://doi.org/10.1016/j.amjoto.2022.103453. DOI: 10.1016/j.amjoto.2022.103453. PMID: 35460972.
Article10. Dhaliwal SS, Sowerby LJ, Rotenberg BW. 2016; Timing of endoscopic surgical decompression in traumatic optic neuropathy: a systematic review of the literature. Int Forum Allergy Rhinol. 6:661–7. https://doi.org/10.1002/alr.21706. DOI: 10.1002/alr.21706. PMID: 26782715.
Article11. Luxenberger W, Stammberger H, Jebeles JA, Walch C. 1998; Endoscopic optic nerve decompression: the Graz experience. Laryngoscope. 108:873–82. https://doi.org/10.1097/00005537-199806000-00016. DOI: 10.1097/00005537-199806000-00016. PMID: 9628503.
Article12. Thota R, Kumar R, Kumar R, Jat B. 2019; Navigation-assisted endonasal endoscopic optic nerve decompression in fibrous dysplasia. BMJ Case Rep CP. 12:e230621. https://doi.org/10.1136/bcr-2019-230621. DOI: 10.1136/bcr-2019-230621. PMID: 31888916. PMCID: PMC6936570.
Article13. Wladis EJ, Aakalu VK, Sobel RK, McCulley TJ, Foster JA, Tao JP, et al. 2021; Interventions for indirect traumatic optic neuropathy: a report by the American Academy of Ophthalmology. Ophthalmology. 128:928–37. https://doi.org/10.1016/j.ophtha.2020.10.038. DOI: 10.1016/j.ophtha.2020.10.038. PMID: 33161071.
Article14. Chen F, Zuo K, Feng S, Guo J, Fan Y, Shi J, et al. 2014; A modified surgical procedure for endoscopic optic nerve decompression for the treatment of traumatic optic neuropathy. N Am J Med Sci. 6:270–3. https://doi.org/10.4103/1947-2714.134372. DOI: 10.4103/1947-2714.134372. PMID: 25006562. PMCID: PMC4083528.
Article15. Yu B, Ma Y, Tu Y, Wu W. 2016; The outcome of endoscopic transethmosphenoid optic canal decompression for indirect traumatic optic neuropathy with no-light-perception. J Ophthalmol. 2016:6492858. https://doi.org/10.1155/2016/6492858. DOI: 10.1155/2016/6492858. PMID: 27965891. PMCID: PMC5124648.
Article16. Yu-Wai-Man P. 2015; Traumatic optic neuropathy: clinical features and management issues. Taiwan J Ophthalmol. 5:3–8. https://doi.org/10.1016/j.tjo.2015.01.003. DOI: 10.1016/j.tjo.2015.01.003. PMID: 26052483. PMCID: PMC4457437.
Article17. Emanuelli E, Bignami M, Digilio E, Fusetti S, Volo T, Castelnuovo P. 2015; Post-traumatic optic neuropathy: our surgical and medical protocol. Eur Arch Otorhinolaryngol. 272:3301–9. https://doi.org/10.1007/s00405-014-3408-5. DOI: 10.1007/s00405-014-3408-5. PMID: 25472815.
Article18. Leitner I, Andrianakis A, Gellner V, Kiss P, Andrianakis D, Tomazic PV. 2022; Optic nerve injury in preoperative imaging is associated with visual improvement outcome in endoscopic optic nerve decompression. Wien Klin Wochenschr. 134:185–94. https://doi.org/10.1007/s00508-021-01915-x. DOI: 10.1007/s00508-021-01915-x. PMID: 34342713. PMCID: PMC8921008.
Article19. Berhouma M, Jacquesson T, Abouaf L, Vighetto A, Jouanneau E. 2014; Endoscopic endonasal optic nerve and orbital apex decompression for nontraumatic optic neuropathy: surgical nuances and review of the literature. Neurosurg Focus. 37:E19. https://doi.org/10.3171/2014.7.FOCUS14303. DOI: 10.3171/2014.7.FOCUS14303. PMID: 25270138.
Article20. Azarmehr I, Stokbro K, Bell RB, Thygesen T. 2017; Surgical navigation: a systematic review of indications, treatments, and outcomes in oral and maxillofacial surgery. J Oral Maxillofac Surg. 75:1987–2005. https://doi.org/10.1016/j.joms.2017.01.004. DOI: 10.1016/j.joms.2017.01.004. PMID: 28193444.
Article21. Yu H, Shen G, Wang X, Zhang S. 2010; Navigation-guided reduction and orbital floor reconstruction in the treatment of zygomatic-orbital-maxillary complex fractures. J Oral Maxillofac Surg. 68:28–34. https://doi.org/10.1016/j.joms.2009.07.058. DOI: 10.1016/j.joms.2009.07.058. PMID: 20006151.
Article22. Liu Y, Yu H, Zhen H. 2019; Navigation-assisted, endonasal, endoscopic optic nerve decompression for the treatment of nontraumatic optic neuropathy. J Craniomaxillofac Surg. 47:328–33. https://doi.org/10.1016/j.jcms.2018.12.009. DOI: 10.1016/j.jcms.2018.12.009. PMID: 30600198.
Article23. Hassfeld S, Mühling J. 2001; Computer assisted oral and maxillofacial surgery: a review and an assessment of technology. Int J Oral Maxillofac Surg. 30:2–13. https://doi.org/10.1054/ijom.2000.0024. DOI: 10.1054/ijom.2000.0024. PMID: 11289616.
Article24. Sukegawa S, Kanno T, Furuki Y. 2018; Application of computer-assisted navigation systems in oral and maxillofacial surgery. Jpn Dent Sci Rev. 54:139–49. https://doi.org/10.1016/j.jdsr.2018.03.005. DOI: 10.1016/j.jdsr.2018.03.005. PMID: 30128061. PMCID: PMC6094868.
Article25. van Hout WM, Van Cann EM, Muradin MS, Frank MH, Koole R. 2014; Intraoperative imaging for the repair of zygomaticomaxillary complex fractures: a comprehensive review of the literature. J Craniomaxillofac Surg. 42:1918–23. https://doi.org/10.1016/j.jcms.2014.07.012. DOI: 10.1016/j.jcms.2014.07.012. PMID: 25213198.
Article26. Xiao R, Miller JA, Sabharwal NC, Lubelski D, Alentado VJ, Healy AT, et al. 2017; Clinical outcomes following spinal fusion using an intraoperative computed tomographic 3D imaging system. J Neurosurg Spine. 26:628–37. https://doi.org/10.3171/2016.10.SPINE16373. DOI: 10.3171/2016.10.SPINE16373. PMID: 28291408.
Article27. Sun J, Cai X, Zou W, Zhang J. 2021; Outcome of endoscopic optic nerve decompression for traumatic optic neuropathy. Ann Otol Rhinol Laryngol. 130:56–9. https://doi.org/10.1177/0003489420939594. DOI: 10.1177/0003489420939594. PMID: 32627571.
Article28. Yang QT, Zhang GH, Liu X, Ye J, Li Y. 2012; The therapeutic efficacy of endoscopic optic nerve decompression and its effects on the prognoses of 96 cases of traumatic optic neuropathy. J Trauma Acute Care Surg. 72:1350–5. https://doi.org/10.1097/TA.0b013e3182493c70. DOI: 10.1097/TA.0b013e3182493c70. PMID: 22673265.
Article29. He ZH, Lan ZB, Xiong A, Hou GK, Pan YW, Li Q, et al. 2016; Endoscopic decompression of the optic canal for traumatic optic neuropathy. Chin J Traumatol. 19:330–2. https://doi.org/10.1016/j.cjtee.2016.03.004. DOI: 10.1016/j.cjtee.2016.03.004. PMID: 28088936. PMCID: PMC5198913.
Article30. Zhao SF, Yong L, Zhang JL, Wu JP, Liu HC, Sun S, et al. 2021; Role of delayed wider endoscopic optic decompression for traumatic optic neuropathy: a single-center surgical experience. Ann Transl Med. 9:136. https://doi.org/10.21037/atm-20-7810. DOI: 10.21037/atm-20-7810. PMID: 33569438. PMCID: PMC7867910.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- 2 Cases of Optic Nerve Decompression of Two Traumatic Optic Neuropathies Using Intranasal Endoscope
- Endoscopic Optic Nerve Decompression in Traumatic Optic Neuropathy
- Three Cases of Endoscopic Endonasal Optic Nerve Decompression for Nontraumatic Optic Neuropathy
- The Etiology of Optic Neuropathy
- Clinical Evaluation of the Traumatic Optic Neuropathy
