Clinical Applicability and Safety of Conventional Frame-Based Stereotactic Techniques for Stereoelectroencephalography
- Affiliations
-
- 1Department of Neurological Surgery, Asan Medical Center, University of Ulsan College of Medicine, Seoul, Korea
- 2Division of Pediatric Neurology, Department of Pediatrics, Asan Medical Center Children’s Hospital, University of Ulsan College of Medicine, Seoul, Korea
- 3Department of Neurology, Asan Medical Center, University of Ulsan College of Medicine, Seoul, Korea
- KMID: 2560408
- DOI: http://doi.org/10.3340/jkns.2023.0246
Abstract
Objective
: Stereoelectroencephalography (SEEG) is increasingly being recognized as an important invasive modality for presurgical evaluation of epilepsy. This study focuses on the clinical and technical considerations of SEEG investigations when using conventional frame-based stereotaxy, drawing on institutional experience and a comprehensive review of relevant literature.
Methods
: This retrospective observational study encompassed the surgical implantation of 201 SEEG electrodes in 16 epilepsy patients using a frame-based stereotactic instrument at a single tertiary-level center. We provide detailed descriptions of the operative procedures and technical nuances for bilateral and multiple SEEG insertions, along with several illustrative cases. Additionally, we present a literature review on the technical aspects of the SEEG procedure, discussing its clinical implications and potential risks.
Results
: Frame-based SEEG electrode placements were successfully performed through sagittal arc application, with the majority (81.2%) of cases being bilateral and involving up to 18 electrodes in a single operation. The median skin-to-skin operation time was 162 minutes (interquartile range [IQR], 145–200), with a median of 13 minutes (IQR, 12–15) per electrode placement for time efficiency. There were two occurrences (1.0%) of electrode misplacement and one instance (0.5%) of a postoperative complication, which manifested as a delayed intraparenchymal hemorrhage. Following SEEG investigation, 11 patients proceeded with surgical intervention, resulting in favorable seizure outcomes for nine (81.8%) and complete remission for eight cases (72.7%).
Conclusion
: Conventional frame-based stereotactic techniques remain a reliable and effective option for bilateral and multiple SEEG electrode placements. While SEEG is a suitable approach for selected patients who are strong candidates for epilepsy surgery, it is important to remain vigilant concerning the potential risks of electrode misplacement and hemorrhagic complications.
Keyword
Figure
-
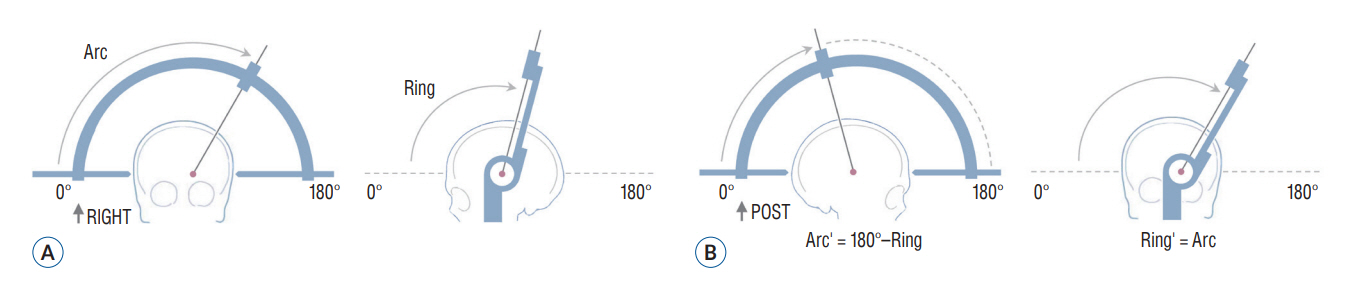
Fig. 1. Sagittal application of the stereotactic arc and corresponding angle parameters in the Leksell stereotactic system. A : Lateral-right orientation of the stereotactic arc. B : Sagittal-posterior orientation of the stereotactic arc (for the target in the left hemisphere). For stereoelectroencephalography requiring multiple and bilateral electrode placements, anterior/posterior orientations of the stereotactic arc may be preferred to the common lateralleft orientation. In these configurations, the arc support is attached to the x-axis of the coordinate frame instead of the y-axis. Following the center-of-arc principle, the target coordinate remains unchanged, but the coordinate on the arc axis needs to be set to its appropriate index mark : lateral-left orientation and anterior orientation share the same index, while the index for posterior orientation is obtained by subtracting from 200 mm. For anterior/posterior orientations, the arc axis should be set as the y-axis, which entails an additional adjustment of 15 mm from the x-axis value used for lateral orientations. Additionally, the ‘arc’ and ‘ring’ angle parameters need to be exchanged to maintain the correct entry point, with posterior arch orientation being optimal for the left hemisphere and anterior orientation for the right hemisphere. To convert between anterior and posterior orientations, both the ‘arc’ and ‘ring’ angles are simply subtracted from 180°.
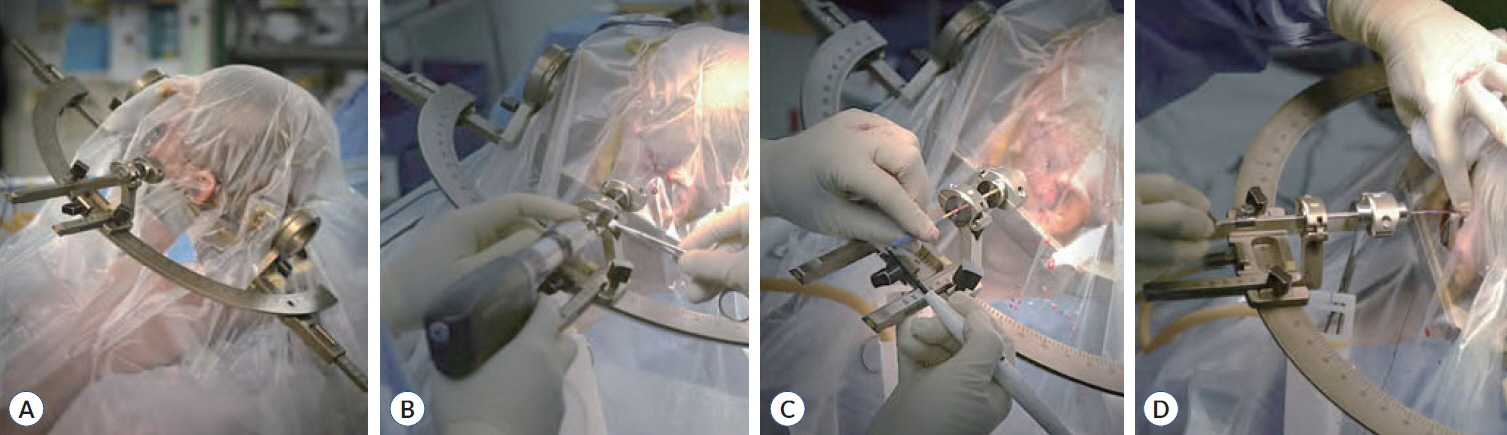
Fig. 2. Operative techniques for multiple SEEG electrode placement using frame-based stereotactic system. A : Patient positioning and application of the stereotactic arc (Leksell®; Elekta AB, Stockholm, Sweden). This orientation of the stereotactic arc allows bilateral access under a single surgical drape, though it is worth noting that the arc apparatus may obscure some areas in the occipital region. B : Drilling into the skull using a twist drill. Pre-measured skull depth at the entry point ensures procedure safety. C : Dural puncture with a monopolar cautery. This step proceeds in a blind manner, and practitioners should be vigilant to avoid violations to the brain parenchyma and superficial vessels. D : Fixation of the anchor bolt (Depthalon®; PMT Co., Chanhassen, MN, USA). The depth for electrode advancement is determined by subtracting the measured length between the arc and the fixed anchor point from the working length (typically 190 mm in the demonstrated system).
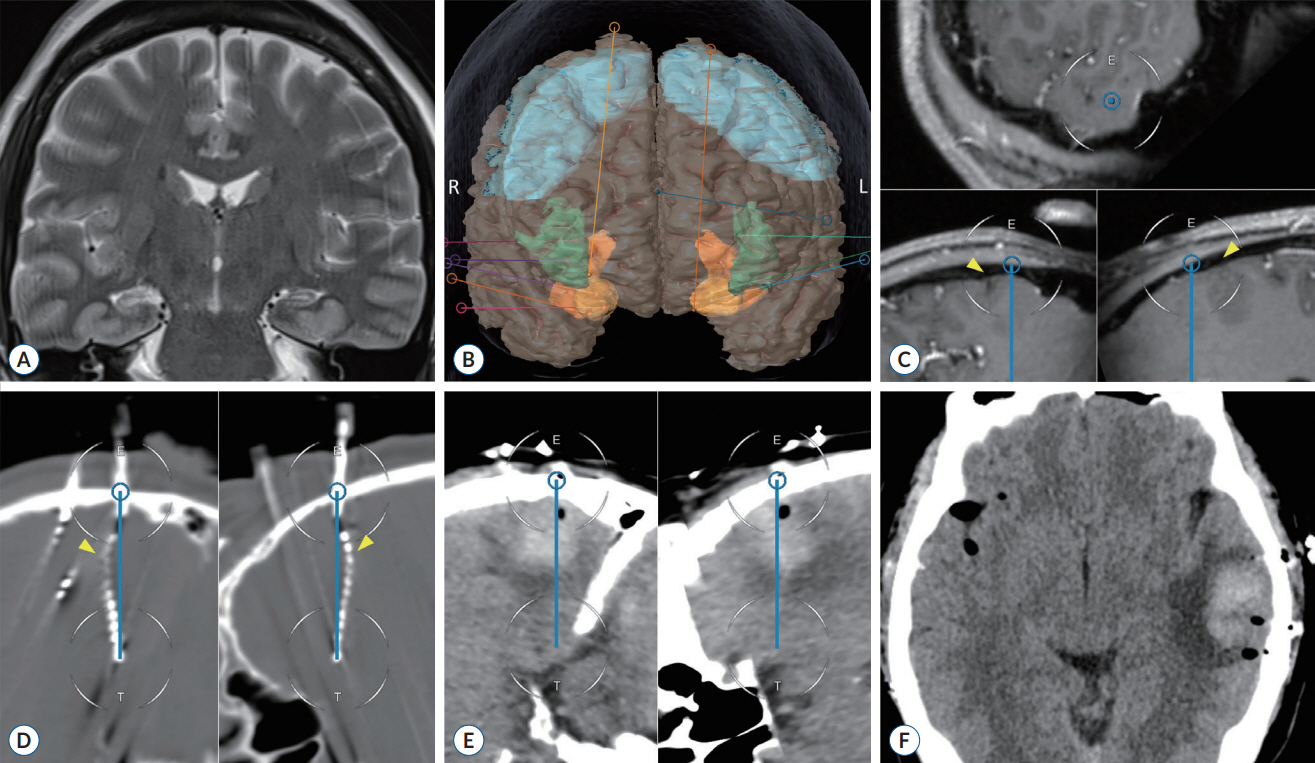
Fig. 3. Postoperative intracranial hemorrhage following SEEG. Pre- and postoperative MRIs and the SEEG planning are presented (case #16). A 49-year-old female with a history of encephalitis and status epilepticus was referred for surgical intervention due to drug-resistant focal epilepsy, despite being on five antiseizure medications. MRI scans revealed bilateral hippocampal sclerosis and sequalae of encephalitis (A). SEEG was conducted to explore both the bilateral mesial temporal and operculo-insular regions (B). Preoperative post-contrast MRIs showed that a trajectory for targeting the left hippocampus was designed to ensure safe entry into brain parenchyma without damaging adjacent vasculature (C, arrowheads). However, during the procedure the SEEG electrode deviated from the planned trajectory, likely due to brain shift, passing through the nearby sulci (D, arrowheads). Initially, the patient tolerated the procedure well and was sent to epilepsy monitoring unit for long-term SEEG monitoring. However, a week later, the patient developed global dysphasia, and a follow-up imaging scans revealed a delayed postoperative hemorrhage (E and F). SEEG : stereoelectroencephalography, MRI : magnetic resonance imaging.
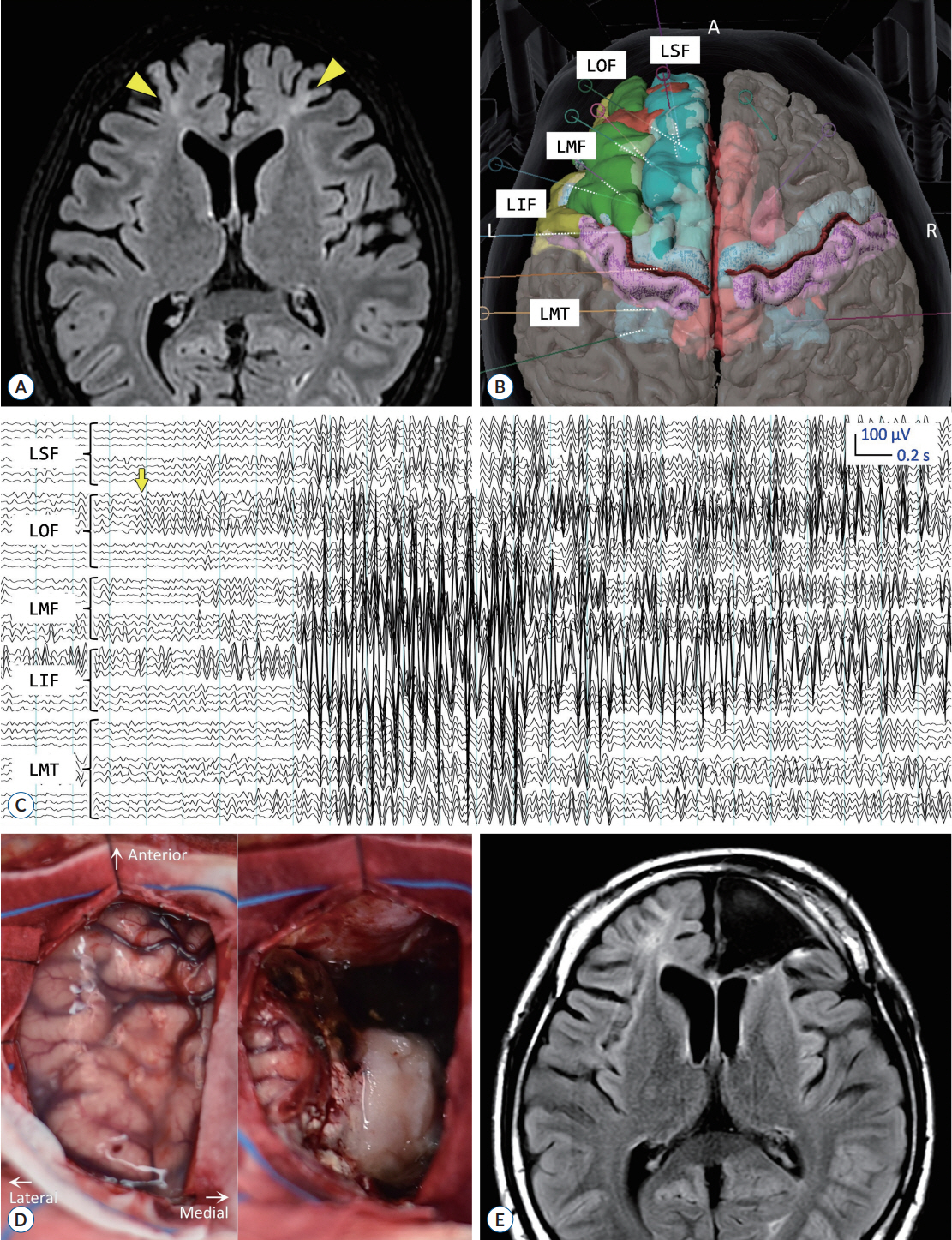
Fig. 4. Successful seizure control following SEEG-guided resective surgery. The figure illustrates pre- and postoperative MRIs, SEEG planning, and intraoperative gross inspections from a representative case (case #13). A 15-year-old male with a history of hypoxic-ischemic encephalopathy had bilateral frontal atrophy with encephalomalacia (A, arrowheads). His seizures, characterized by hyperkinetic movements occurring several times a day, remained intractable despite the use of four antiseizure medications, causing significant distress to his caregiver. SEEG monitoring was performed to assess the feasibility of resective surgery (B). During SEEG, seizures were observed to initiate at the left orbitofrontal (C, arrow) and anterior cingulate regions, corresponding to the structural lesion observed in the MRI. The patient underwent a left frontal lobectomy (D and E) and subsequently achieved seizure remission while also reducing the number of medications (Engel Ia). LOF : left orbitofrontal gyrus, LSF : left superior frontal gyrus, LMF : left middle frontal gyrus, LIF : left inferior frontal gyrus, SEEG : stereoelectroencephalography, MRI : magnetic resonance imaging.
Reference
-
References
1. Bartolomei F, Lagarde S, Wendling F, McGonigal A, Jirsa V, Guye M, et al. Defining epileptogenic networks: contribution of SEEG and signal analysis. Epilepsia. 58:1131–1147. 2017.
Article2. Bartolomei F, Nica A, Valenti-Hirsch MP, Adam C, Denuelle M. Interpretation of SEEG recordings. Neurophysiol Clin. 48:53–57. 2018.
Article3. Bonda DJ, Pruitt R, Theroux L, Goldstein T, Stefanov DG, Kothare S, et al. Robot-assisted stereoelectroencephalography electrode placement in twenty-three pediatric patients: a high-resolution analysis of individual lead placement time and accuracy at a single institution. Childs Nerv Syst. 37:2251–2259. 2021.
Article4. Bottan JS, Rubino PA, Lau JC, MacDougall KW, Parrent AG, Burneo JG, et al. Robot-assisted insular depth electrode implantation through oblique trajectories: 3-dimensional anatomical nuances, technique, accuracy, and safety. Oper Neurosurg (Hagerstown). 18:278–283. 2020.
Article5. Bourdillon P, Châtillon CE, Moles A, Rheims S, Catenoix H, Montavont A, et al. Effective accuracy of stereoelectroencephalography: robotic 3D versus Talairach orthogonal approaches. J Neurosurg. 131:1938–1946. 2018.
Article6. Budke M, Avecillas-Chasin JM, Villarejo F. Implantation of depth electrodes in children using VarioGuide® frameless navigation system: technical Note. Oper Neurosurg (Hagerstown). 15:302–309. 2018.
Article7. Candela-Cantó S, Aparicio J, López JM, Baños-Carrasco P, Ramírez-Camacho A, Climent A, et al. Frameless robot-assisted stereoelectroencephalography for refractory epilepsy in pediatric patients: accuracy, usefulness, and technical issues. Acta Neurochir (Wien). 160:2489–2500. 2018.
Article8. Cardinale F, Cossu M, Castana L, Casaceli G, Schiariti MP, Miserocchi A, et al. Stereoelectroencephalography: surgical methodology, safety, and stereotactic application accuracy in 500 procedures. Neurosurgery. 72:353–366. discussion 366. 2013.9. Cardinale F, Rizzi M, d’Orio P, Casaceli G, Arnulfo G, Narizzano M, et al. A new tool for touch-free patient registration for robot-assisted intracranial surgery: application accuracy from a phantom study and a retrospective surgical series. Neurosurg Focus. 42:E8. 2017.
Article10. Cardinale F, Rizzi M, d’Orio P, Castana L. Stereotactic accuracy of stereoelectroencephalography procedures should be measured at both the entry and target points. Acta Neurochir (Wien). 163:1369–1370. 2021.
Article11. Chen Y, Huang T, Sun Y, Liao J, Cao D, Li L, et al. Surface-based registration of MR scan versus refined anatomy-based registration of CT scan: effect on the accuracy of SEEG electrodes implantation performed in prone position under frameless neuronavigation. Stereotact Funct Neurosurg. 98:73–79. 2020.
Article12. D’Agostino E, Kanter J, Song Y, Aronson JP. Stereoencephalography electrode placement accuracy and utility using a frameless insertion platform without a rigid cannula. Oper Neurosurg (Hagerstown). 18:409–416. 2020.
Article13. Dedrickson T, Davidar AD, Azad TD, Theodore N, Anderson WS. Use of the Globus ExcelsiusGPS system for robotic stereoelectroencephalography: an initial experience. World Neurosurg. 175:e686–e692. 2023.
Article14. Dewan MC, Shults R, Hale AT, Sukul V, Englot DJ, Konrad P, et al. Stereotactic EEG via multiple single-path omnidirectional trajectories within a single platform: institutional experience with a novel technique. J Neurosurg. 129:1173–1181. 2018.
Article15. Dorfer C, Minchev G, Czech T, Stefanits H, Feucht M, Pataraia E, et al. A novel miniature robotic device for frameless implantation of depth electrodes in refractory epilepsy. J Neurosurg. 126:1622–1628. 2017.
Article16. Fisher RS, Cross JH, French JA, Higurashi N, Hirsch E, Jansen FE, et al. Operational classification of seizure types by the International League Against Epilepsy: position paper of the ILAE commission for classification and terminology. Epilepsia. 58:522–530. 2017.
Article17. Girgis F, Ovruchesky E, Kennedy J, Seyal M, Shahlaie K, Saez I. Superior accuracy and precision of SEEG electrode insertion with frame-based vs. frameless stereotaxy methods. Acta Neurochir (Wien). 162:2527–2532. 2020.
Article18. Gomes FC, Larcipretti ALL, Nager G, Dagostin CS, Udoma-Udofa OC, Pontes JPM, et al. Robot-assisted vs. manually guided stereoelectroencephalography for refractory epilepsy: a systematic review and meta-analysis. Neurosurg Rev. 46:102. 2023.
Article19. González-Martínez J, Bulacio J, Thompson S, Gale J, Smithason S, Najm I, et al. Technique, results, and complications related to robot-assisted stereoelectroencephalography. Neurosurgery. 78:169–180. 2016.
Article20. Hines K, Matias CM, Leibold A, Sharan A, Wu C. Accuracy and efficiency using frameless transient fiducial registration in stereoelectroencephalography and deep brain stimulation. J Neurosurg. 138:299–305. 2023.
Article21. Hou Z, Chen X, Shi XJ, An N, Yang MH, Yang H, et al. Comparison of neuronavigation and frame-based stereotactic systems in implanting epileptic depth electrodes. Turk Neurosurg. 26:574–581. 2016.22. Isnard J, Taussig D, Bartolomei F, Bourdillon P, Catenoix H, Chassoux F, et al. French guidelines on stereoelectroencephalography (SEEG). Neurophysiol Clin. 48:5–13. 2018.
Article23. Joris V, Ribeiro-Vaz JG, Finet P, El Tahry R, Elkaim LM, Raftopoulos C, et al. Stereoelectroencephalography implantation using frameless neuronavigation and varioguide: prospective analysis of accuracy and safety in a case series of 11 patients. World Neurosurg. 174:e62–e71. 2023.
Article24. Kandregula S, Matias CM, Malla BR, Sperling MR, Wu C, Sharan AD. Accuracy of electrode insertion using frame-based with robot guidance technique in stereotactic electroencephalography: supine versus lateral position. World Neurosurg. 154:e325–e332. 2021.
Article25. Kawashima T, Uda T, Koh S, Yindeedej V, Ishino N, Ichinose T, et al. Intraparenchymal and subarachnoid hemorrhage in stereotactic electroencephalography caused by indirect adjacent arterial injury: illustrative case. Brain Sci. 13:440. 2023.
Article26. Kim LH, Feng AY, Ho AL, Parker JJ, Kumar KK, Chen KS, et al. Robotassisted versus manual navigated stereoelectroencephalography in adult medically-refractory epilepsy patients. Epilepsy Res. 159:106253. 2020.
Article27. Kim LH, Parker JJ, Ho AL, Feng AY, Kumar KK, Chen KS, et al. Contemporaneous evaluation of patient experience, surgical strategy, and seizure outcomes in patients undergoing stereoelectroencephalography or subdural electrode monitoring. Epilepsia. 62:74–84. 2021.
Article28. Kogias E, Altenmüller DM, Karakolios K, Egger K, Coenen VA, Schulze-Bonhage A, et al. Electrode placement for SEEG: combining stereotactic technique with latest generation planning software for intraoperative visualization and postoperative evaluation of accuracy and accuracy predictors. Clin Neurol Neurosurg. 213:107137. 2022.
Article29. Ladisich B, Machegger L, Romagna A, Krainz H, Steinbacher J, Leitinger M, et al. VarioGuide® frameless neuronavigation-guided stereoelectroencephalography in adult epilepsy patients: technique, accuracy and clinical experience. Acta Neurochir (Wien). 163:1355–1364. 2021.
Article30. Lee EJ, Kalia SK, Hong SH. A primer on magnetic resonance-guided laser interstitial thermal therapy for medically refractory epilepsy. J Korean Neurosurg Soc. 62:353–360. 2019.
Article31. Machetanz K, Grimm F, Wuttke TV, Kegele J, Lerche H, Tatagiba M, et al. Frame-based and robot-assisted insular stereo-electroencephalography via an anterior or posterior oblique approach. J Neurosurg. 135:1477–1486. 2021.
Article32. McGovern RA, Ruggieri P, Bulacio J, Najm I, Bingaman WE, Gonzalez-Martinez JA. Risk analysis of hemorrhage in stereo-electroencephalography procedures. Epilepsia. 60:571–580. 2019.
Article33. Mullin JP, Shriver M, Alomar S, Najm I, Bulacio J, Chauvel P, et al. Is SEEG safe? A systematic review and meta-analysis of stereo-electroencephalography-related complications. Epilepsia. 57:386–401. 2016.
Article34. Nowell M, Rodionov R, Diehl B, Wehner T, Zombori G, Kinghorn J, et al. A novel method for implementation of frameless StereoEEG in epilepsy surgery. Neurosurgery 10 Suppl. 4:525–533. discussion 533-534. 2014.
Article35. Reif PS, Strzelczyk A, Rosenow F. The history of invasive EEG evaluation in epilepsy patients. Seizure. 41:191–195. 2016.
Article36. Roessler K, Sommer B, Merkel A, Rampp S, Gollwitzer S, Hamer HM, et al. A frameless stereotactic implantation technique for depth electrodes in refractory epilepsy using intraoperative magnetic resonance imaging. World Neurosurg. 94:206–210. 2016.
Article37. Sharma JD, Seunarine KK, Tahir MZ, Tisdall MM. Accuracy of robot-assisted versus optical frameless navigated stereoelectroencephalography electrode placement in children. J Neurosurg Pediatr. 23:297–302. 2019.
Article38. Song S, Dai Y, Chen Z, Shi S. Accuracy and feasibility analysis of SEEG electrode implantation using the VarioGuide frameless navigation system in patients with drug-resistant epilepsy. J Neurol Surg A Cent Eur Neurosurg. 82:430–436. 2021.
Article39. Spyrantis A, Cattani A, Woebbecke T, Konczalla J, Strzelczyk A, Rosenow F, et al. Electrode placement accuracy in robot-assisted epilepsy surgery: a comparison of different referencing techniques including frame-based CT versus facial laser scan based on CT or MRI. Epilepsy Behav. 91:38–47. 2019.
Article40. Vakharia VN, Duncan JS. Automation advances in stereoelectroencephalography planning. Neurosurg Clin N Am. 31:407–419. 2020.
Article41. Vakharia VN, Rodionov R, Miserocchi A, McEvoy AW, O’Keeffe A, Granados A, et al. Comparison of robotic and manual implantation of intracerebral electrodes: a single-centre, single-blinded, randomised controlled trial. Sci Rep. 11:17127. 2021.
Article42. Vakharia VN, Sparks R, O’Keeffe AG, Rodionov R, Miserocchi A, McEvoy A, et al. Accuracy of intracranial electrode placement for stereoencephalography: a systematic review and meta-analysis. Epilepsia. 58:921–932. 2017.43. van der Loo LE, Schijns OEMG, Hoogland G, Colon AJ, Wagner GL, Dings JTA, et al. Methodology, outcome, safety and in vivo accuracy in traditional frame-based stereoelectroencephalography. Acta Neurochir (Wien). 159:1733–1746. 2017.
Article44. Verburg N, Baayen JC, Idema S, Klitsie MA, Claus S, de Jonge CS, et al. In vivo accuracy of a frameless stereotactic drilling technique for diagnostic biopsies and stereoelectroencephalography depth electrodes. World Neurosurg. 87:392–398. 2016.
Article45. Yu H, Pistol C, Franklin R, Barborica A. Clinical accuracy of customized stereotactic fixtures for stereoelectroencephalography. World Neurosurg. 109:82–88. 2018.
Article46. Zheng J, Liu YL, Zhang D, Cui XH, Sang LX, Xie T, et al. Robot-assisted versus stereotactic frame-based stereoelectroencephalography in medically refractory epilepsy. Neurophysiol Clin. 51:111–119. 2021.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Frameless stereotactic brain biopsy: technical considerations and clinical results regarding safety and efficacy
- Stereotactic computed tomography-guided aspiration of intracerebral hemorrhage using the Cosman-Roberts-Wells system
- How to use neuronavigation for the brain
- Stereoelectroencephalography in Pediatric Epilepsy Surgery
- Evaluation of Stereotactic Aspiration of Spontaneous Intracerebral Hematoma using Multiple Catheters
