Reconstruction of an upper lip vermilion defect with a mucosal V-Y advancement flap: a case report
- Affiliations
-
- 1Department of Oral and Maxillofacial Surgery, School of Dentistry, Kyungpook National University, Daegu, Korea
- KMID: 2559269
- DOI: http://doi.org/10.5125/jkaoms.2024.50.4.222
Abstract
- The upper lip is a functionally and aesthetically important area of the face. Therefore, reconstruction of an upper lip defect needs sufficient consideration to ensure functional and aesthetic recovery. Several methods, such as wedge resection, rotation flaps, advancement flaps, and myomucosal advancement flaps, have been used to reconstruct vermilion defects. However, it is challenging to reconstruct a vermilion defect because of the possibility of residual asymmetry or scars and restrictions to normal lip movement after the reconstruction. We present the case of a 51-year-old female that had an upper lip vermilion defect caused by a dog bite. The lip defect was reconstructed using a mucosal V-Y advancement flap. This mucosal flap was based on the orbicularis oris muscle with a branch of the superior labial artery to ensure sufficient blood supply. Therefore, flap survival was excellent, and there was no constriction of the flaps. Moreover, the color and contour were matched to the adjacent lip tissue, and re-establishment of the white roll and adequate lip volume were achieved. This mucosal V-Y advancement flap technique represents a reliable method to repair mucosal defects without vascular compromise of the flap.
Figure
-

Fig. 1 A. The lip wound was thoroughly debrided before reconstruction. B. Design of the mucosal V-Y advancement flap in the inner mucosal area. C. Completion of the mucosal V-Y advancement flap dissection based on the orbicularis oris muscle. An additional horizontal incision was made in the orbicularis oris muscle to facilitate flap mobilization. D. The shield-shaped flap was moved superiorly to approximate the superior flap margin to the vermilion border. E. The V-Y suture was placed between the inner mucosa and flap. F. After reconstruction of the upper lip defect, good color matching and volume were observed.
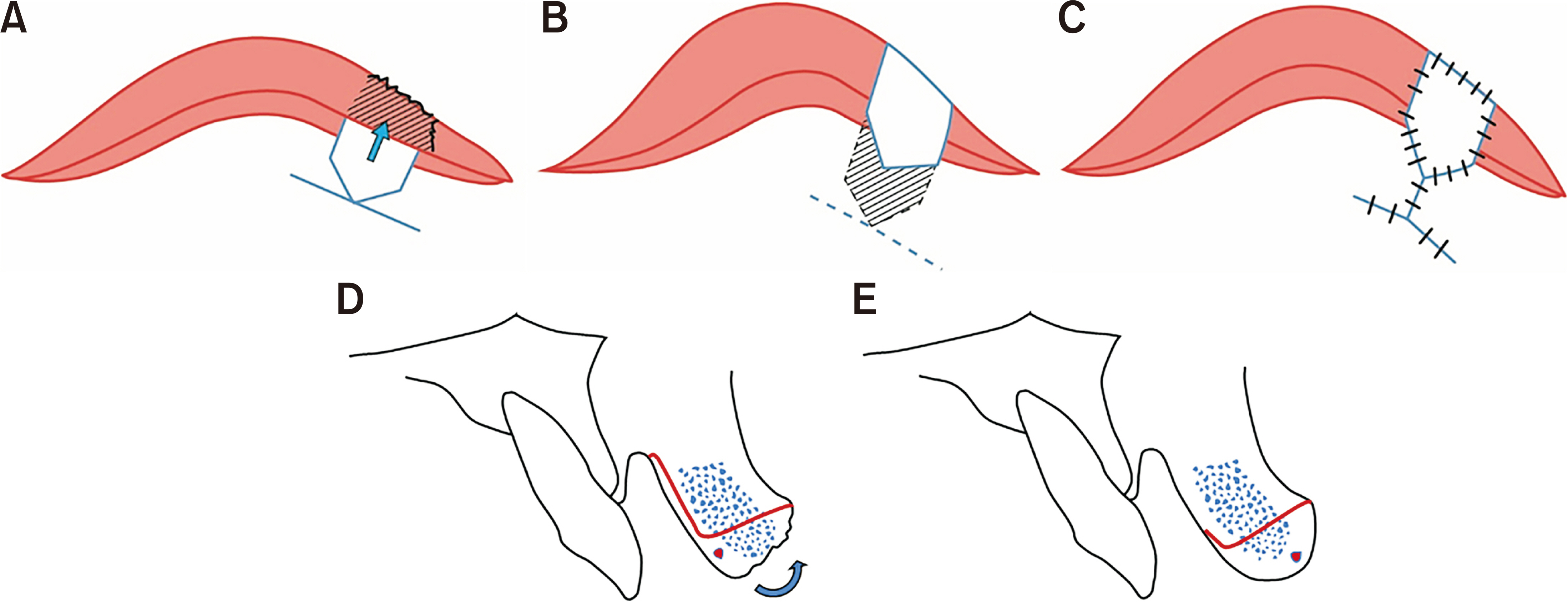
Fig. 2 Schematic illustration of the mucosal V-Y advancement flap. A-C. The mucosal incision was made at the inner lip mucosa. The mobilized mucosal flap was approximated to the vermilion-skin border. The inner vestibule was sutured in a Y-shaped manner. D, E. Cross section of the flap. The labial artery was included in the mucosal flap, and dissection proceeded.

Fig. 3 A. Clinical findings of the lip immediately after the surgery. B. One-month postoperative photograph. Excessive lip volume from the mobilized flap was revised after excision of the redundant lip tissue. C. Six-month postoperative view. D. One year after the reconstruction, both the volume and width of the flap were symmetrical and matched the original color.
Reference
-
References
1. Daraei P, Calligas JP, Katz E, Etra JW, Sethna AB. 2014; Reconstruction of upper lip avulsion after dog bite: case report and review of literature. Am J Otolaryngol. 35:219–25. https://doi.org/10.1016/j.amjoto.2013.11.008. DOI: 10.1016/j.amjoto.2013.11.008. PMID: 24332929.
Article2. Jin X, Teng L, Zhang C, Xu J, Lu J, Zhang B, et al. 2011; Reconstruction of partial-thickness vermilion defects with a mucosal V-Y advancement flap based on the orbicularis oris muscle. J Plast Reconstr Aesthet Surg. 64:472–6. https://doi.org/10.1016/j.bjps.2010.07.017. DOI: 10.1016/j.bjps.2010.07.017. PMID: 20709612.3. Malard O, Corre P, Jégoux F, Durand N, Dréno B, Beauvillain C, et al. 2010; Surgical repair of labial defect. Eur Ann Otorhinolaryngol Head Neck Dis. 127:49–62. https://doi.org/10.1016/j.anorl.2010.04.001. DOI: 10.1016/j.anorl.2010.04.001. PMID: 20822758.
Article4. Madorsky S, Meltzer O. 2020; Myomucosal lip island flap for reconstruction of small to medium lower lip defects. Facial Plast Surg Aesthet Med. 22:200–6. https://doi.org/10.1089/fpsam.2020.0068. DOI: 10.1089/fpsam.2020.0068. PMID: 32255366. PMCID: PMC7312741.
Article5. Pepper JP, Baker SR. 2013; Local flaps: cheek and lip reconstruction. JAMA Facial Plast Surg. 15:374–82. https://doi.org/10.1001/jamafacial.2013.1608. DOI: 10.1001/jamafacial.2013.1608. PMID: 24051684.
Article6. Srivastava S. 1989; Reconstruction of traumatic loss of vermilion and mucocutaneous junction of the lips. Br J Plast Surg. 42:526–9. https://doi.org/10.1016/0007-1226(89)90038-6. DOI: 10.1016/0007-1226(89)90038-6. PMID: 2804516.
Article7. Kolhe PS, Leonard AG. 1988; Reconstruction of the vermilion after "lip-shave". Br J Plast Surg. 41:68–73. https://doi.org/10.1016/0007-1226(88)90147-6. DOI: 10.1016/0007-1226(88)90147-6. PMID: 3345410.
Article8. Lane JE, Kent DE. 2007; Repair of vermilion Mohs defect with unilateral axial myocutaneous advancement flap. Dermatol Surg. 33:1502–4. discussion 1504. https://doi.org/10.1111/j.1524-4725.2007.33324.x. DOI: 10.1111/j.1524-4725.2007.33324.x. PMID: 18076619.
Article9. Martin TJ, Zhang Y, Rhee JS. 2008; Options for upper lip reconstruction: a survey-based analysis. Dermatol Surg. 34:1652–8. https://doi.org/10.1111/j.1524-4725.2008.34342.x. DOI: 10.1111/j.1524-4725.2008.34342.x. PMID: 19018829.
Article10. Boson AL, Boukovalas S, Hays JP, Hammel JA, Cole EL, Wagner RF Jr. 2021; Upper lip anatomy, mechanics of local flaps, and considerations for reconstruction. Cutis. 107:144–8. https://doi.org/10.12788/cutis.0205. DOI: 10.12788/cutis.0205. PMID: 33956606.
Article11. Nicholas MN, Liu A, Chan AR, Jia J, Fuller K, Eisen DB. 2021; Postoperative outcomes of local skin flaps used in oncologic reconstructive surgery of the upper cutaneous lip: a systematic review. Dermatol Surg. 47:1047–51. https://doi.org/10.1097/DSS.0000000000003063. DOI: 10.1097/DSS.0000000000003063. PMID: 33927091.
Article12. Duan M, Yue C, Dai Y, Wu Y, Peng J. 2024; Technical solution for reconstruction of upper lip defect by bilateral V-Y advanced flaps. J Am Acad Dermatol. 90:e67–8. https://doi.org/10.1016/j.jaad.2022.09.047. DOI: 10.1016/j.jaad.2022.09.047. PMID: 36206935.13. Drosou A, Trieu D, Goldberg LH. 2017; Reconstruction of a postoperative mohs defect of the upper cutaneous and vermilion lip involving cupid's bow. Dermatol Surg. 43 Suppl 1:S96–8. https://doi.org/10.1097/DSS.0000000000001034. DOI: 10.1097/DSS.0000000000001034. PMID: 28079636.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Effective method for reconstruction of remaining lower lip vermilion defect after a mental V-Y advancement flap
- Vermilion Reconstruction with Mucosal Island Flap
- Reconstruction of a small defect of the lower vermilion adjacent to white roll using a modified O-Z flap
- Correction of Whistle Deformity Using Modified V-Y Advancement Flap
- Mucosal Roofing Flap Reconstruction to Minimize Horizontal Lip Length Loss and Preserve Mouth Opening in Lower Lip Squamous Cell Carcinoma
