Clinical Application of Optical Genome Mapping for Molecular Diagnosis of Facioscapulohumeral Muscular Dystrophy
- Affiliations
-
- 1Department of Laboratory Medicine, Graduate School of Medical Sciences, Brain Korea 21 Project, Yonsei University College of Medicine, Seoul, Korea
- 2MDxK (Molecular Diagnostics Korea), Inc., Gwacheon, Korea
- 3Department of Genetics, School of Medicine, Washington University in St. Louis, St. Louis, MO, USA
- 4Department of Laboratory Medicine, Yonsei University College of Medicine, Seoul, Korea
- 5Dxome Co. Ltd., Seongnam, Korea
- 6Department of Neurology, Gangnam Severance Hospital, Yonsei University College of Medicine, Seoul, Korea
- KMID: 2559150
- DOI: http://doi.org/10.3343/alm.2023.0437
Abstract
- Background
Facioscapulohumeral muscular dystrophy (FSHD) is a common form of muscular dystrophy that mainly affects skeletal muscle. FSHD1 accounts for 95% of all FSHD cases and can be diagnosed based on the pathogenic contraction of the D4Z4-repeat array on chromosome 4q35. Genetic diagnosis of FSHD1 is challenging because of the large size and repetitive nature of the D4Z4 region. We evaluated the clinical applicability of optical genome mapping (OGM) for the genetic diagnosis of FSHD1.
Methods
We included 25 individuals with clinically confirmed or suspected/probable FSHD and their families. Ultra-high-molecular-weight DNA from peripheral blood was labeled, stained, and imaged using a single-molecule OGM platform (Bionano Genomics Saphyr system). D4Z4 repeat size and haplotype information were analyzed using the manufacturer’s dedicated pipeline. We also compared the workflow and test time between Southern blot analysis and OGM.
Results
We obtained concordant OGM and Southern blot results with 10 samples from patients with clinically confirmed FSHD. The D4Z4 repeat size differed within 1 unit between the Southern blot analysis and OGM. Among nine patients with clinically suspected or probable FSHD, six patients were confirmed to have pathogenic contractions by OGM. In our cohort, one de novo mosaic FSHD1 patient was successfully diagnosed with OGM. Moreover, OGM has a more straightforward and less time-consuming workflow than Southern blot analysis.
Conclusions
OGM enables accurate and reliable detection of pathogenic contraction of the D4Z4-repeat array and is a valuable tool for the genetic diagnosis of FSHD1.
Figure
-
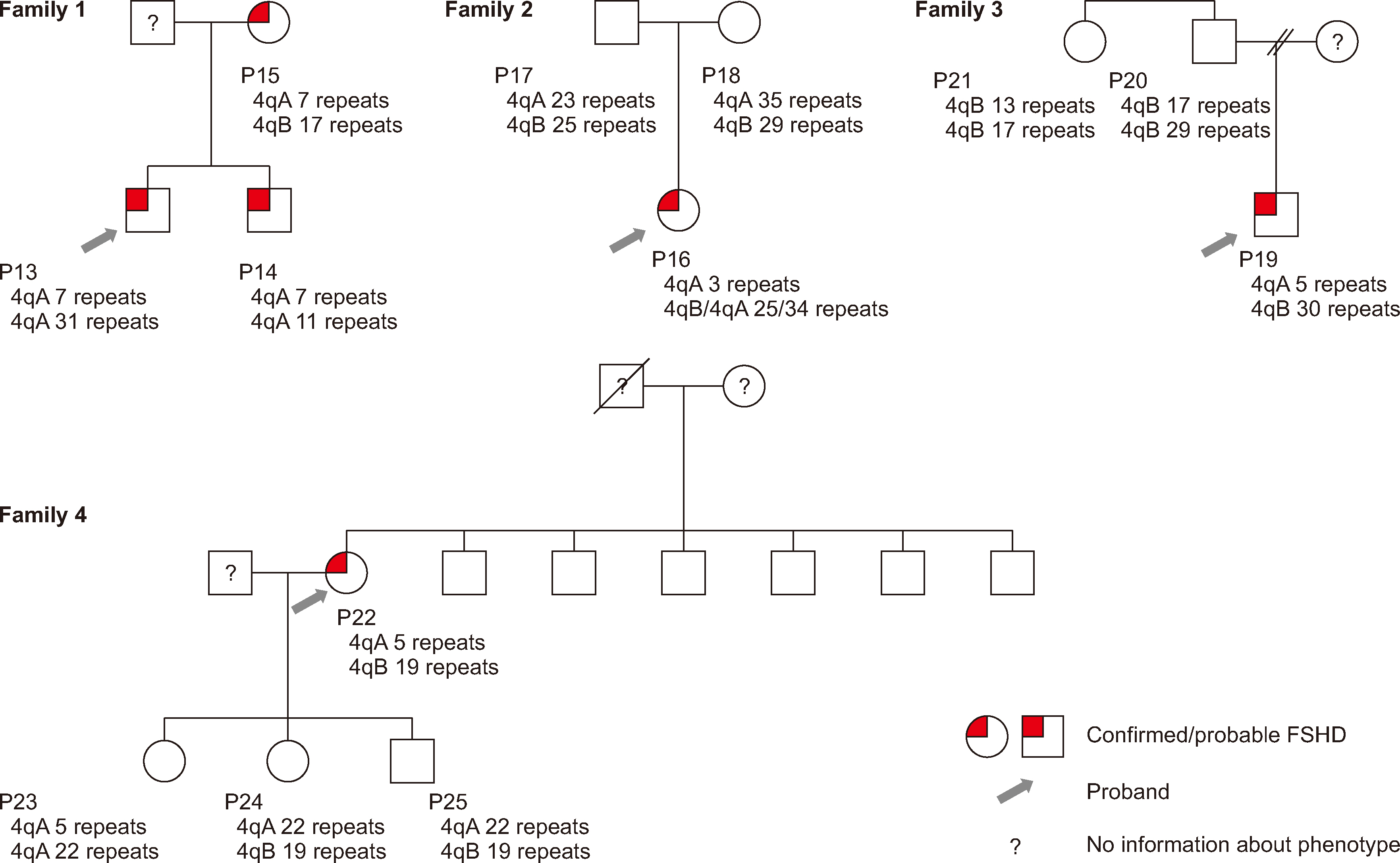
Fig. 1 Pedigrees of four families and their OGM results. Abbreviation: OGM, optical genome mapping.
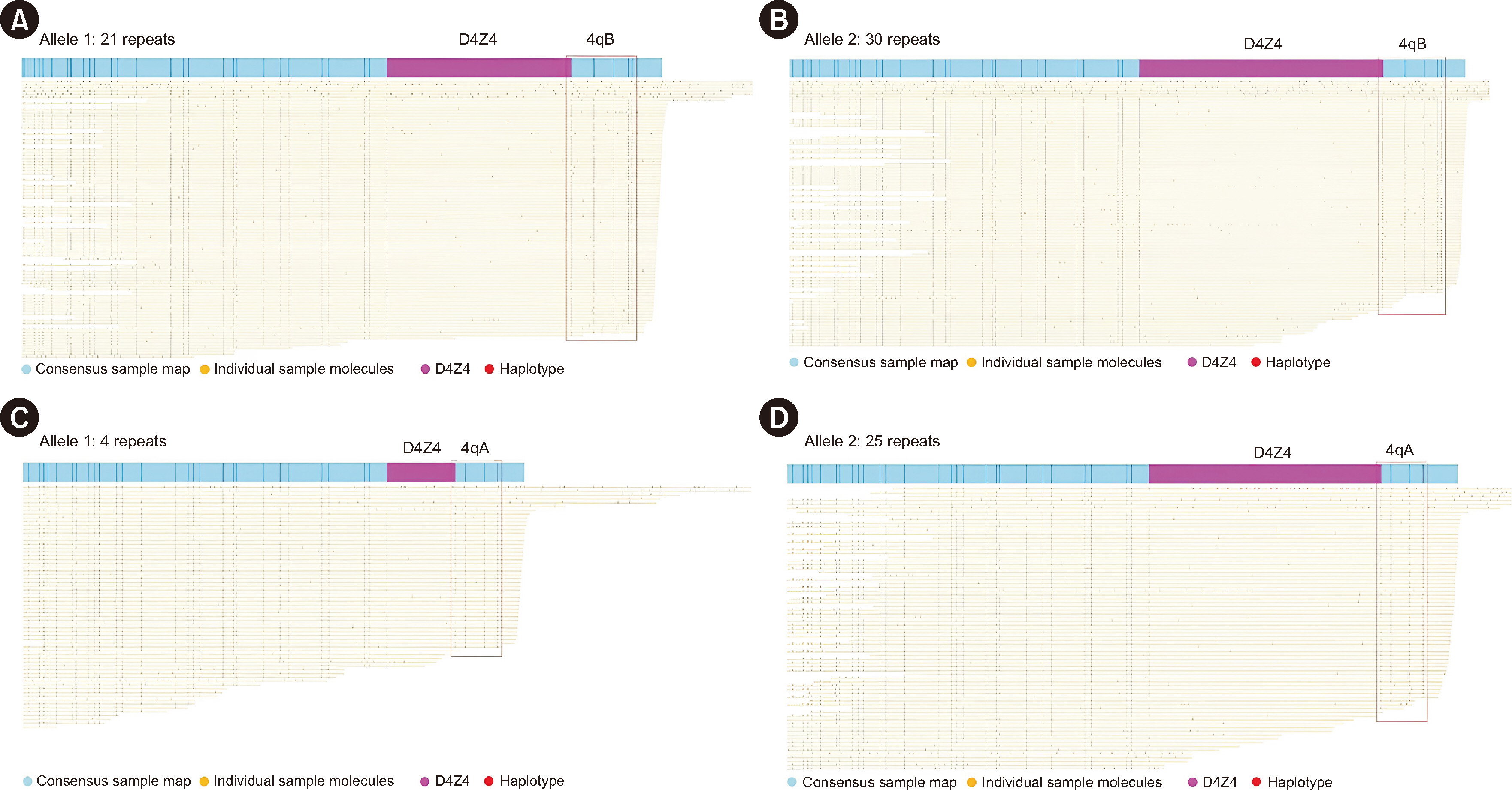
Fig. 2 Representative OGM results from patients with clinically probable/suspected FSHD. (A, B) No pathogenic contraction was identified in a patient with clinically suspected FSHD (P8). (C, D) A pathogenic contraction was identified in a patient with clinically probable FSHD (P9). Abbreviations: OGM, optical genome mapping; FSHD, facioscapulohumeral muscular dystrophy.
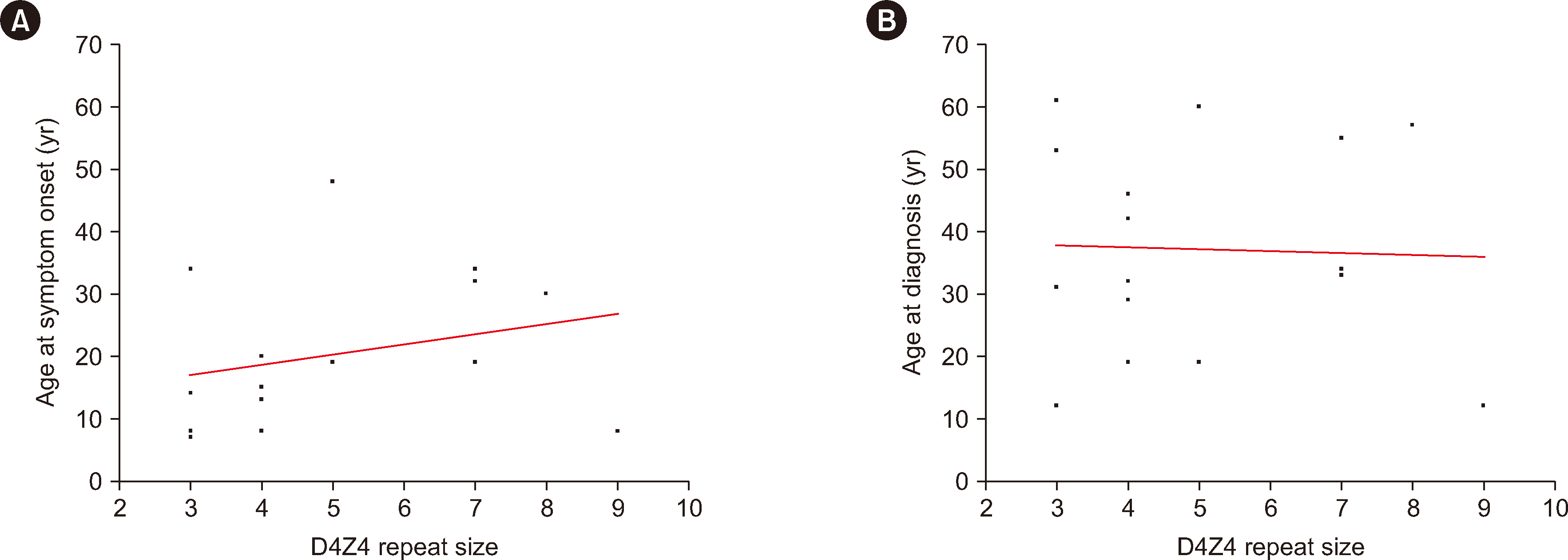
Fig. 3 Correlation between the D4Z4-repeat size and (A) age at symptom onset (r=0.364, R2=0.072, P=0.1654) and (B) age at diagnosis (r=0.020, R2=0.001, P=0.9424) based on OGM for patients with FSHD. Abbreviations: OGM, optical genome mapping; FSHD, facioscapulohumeral muscular dystrophy.
Cited by 1 articles
-
Application of Optical Genome Mapping to the Genetic Diagnosis of Facioscapulohumeral Muscular Dystrophy 1
Seung-Tae Lee
Ann Lab Med. 2024;44(5):383-384. doi: 10.3343/alm.2024.0197.
Reference
-
References
1. Padberg GW, Frants RR, Brouwer OF, Wijmenga C, Bakker E, Sandkuijl LA. 1995; Facioscapulohumeral muscular dystrophy in the Dutch population. Muscle Nerve Suppl. 2:S81–4. DOI: 10.1002/mus.880181315. PMID: 7739631.
Article2. van der Maarel SM, Deidda G, Lemmers RJ, van Overveld PG, van der Wielen M, Hewitt JE, et al. 2000; De novo facioscapulohumeral muscular dystrophy: frequent somatic mosaicism, sex-dependent phenotype, and the role of mitotic transchromosomal repeat interaction between chromosomes 4 and 10. Am J Hum Genet. 66:26–35. DOI: 10.1086/302730. PMID: 10631134. PMCID: PMC1288331.
Article3. Tawil R, Kissel JT, Heatwole C, Pandya S, Gronseth G, Benatar M, et al. 2015; Evidence-based guideline summary: evaluation, diagnosis, and management of facioscapulohumeral muscular dystrophy: report of the Guideline Development, Dissemination, and Implementation Subcommittee of the American Academy of Neurology and the Practice Issues Review Panel of the American Association of Neuromuscular & Electrodiagnostic Medicine. Neurology. 85:357–64. DOI: 10.1212/WNL.0000000000001783. PMID: 26215877. PMCID: PMC4520817.
Article4. Gabriëls J, Beckers MC, Ding H, De Vriese A, Plaisance S, van der Maarel SM, et al. 1999; Nucleotide sequence of the partially deleted D4Z4 locus in a patient with FSHD identifies a putative gene within each 3.3 kb element. Gene. 236:25–32. DOI: 10.1016/S0378-1119(99)00267-X. PMID: 10433963.
Article5. Hamel J, Tawil R. 2018; Facioscapulohumeral muscular dystrophy: update on pathogenesis and future treatments. Neurotherapeutics. 15:863–71. DOI: 10.1007/s13311-018-00675-3. PMID: 30361930. PMCID: PMC6277282.
Article6. Bakker E, Wijmenga C, Vossen RH, Padberg GW, Hewitt J, van der Wielen M, et al. 1995; The FSHD-linked locus D4F104S1 (p13E-11) on 4q35 has a homologue on 10qter. Muscle Nerve Suppl. 2:S39–44. DOI: 10.1002/mus.880181309.
Article7. Deidda G, Cacurri S, Grisanti P, Vigneti E, Piazzo N, Felicetti L. 1995; Physical mapping evidence for a duplicated region on chromosome 10qter showing high homology with the facioscapulohumeral muscular dystrophy locus on chromosome 4qter. Eur J Hum Genet. 3:155–67. DOI: 10.1159/000472291. PMID: 7583041.
Article8. Lemmers RJLF, de Kievit P, Sandkuijl L, Padberg GW, van Ommen GJB, Frants RR, et al. 2002; Facioscapulohumeral muscular dystrophy is uniquely associated with one of the two variants of the 4q subtelomere. Nat Genet. 32:235–6. DOI: 10.1038/ng999. PMID: 12355084.
Article9. Wang LH, Tawil R. 2016; Facioscapulohumeral dystrophy. Curr Neurol Neurosci Rep. 16:66. DOI: 10.1007/s11910-016-0667-0. PMID: 27215221.
Article10. Lemmers RJLF, Goeman JJ, van der Vliet PJ, van Nieuwenhuizen MP, Balog J, Vos-Versteeg M, et al. 2015; Inter-individual differences in CpG methylation at D4Z4 correlate with clinical variability in FSHD1 and FSHD2. Hum Mol Genet. 24:659–69. DOI: 10.1093/hmg/ddu486. PMID: 25256356. PMCID: PMC4291246.
Article11. van den Boogaard ML, Lemmers RJLF, Balog J, Wohlgemuth M, Auranen M, Mitsuhashi S, et al. 2016; Mutations in DNMT3B modify epigenetic repression of the D4Z4 repeat and the penetrance of facioscapulohumeral dystrophy. Am J Hum Genet. 98:1020–9. DOI: 10.1016/j.ajhg.2016.03.013. PMID: 27153398. PMCID: PMC4863565.
Article12. Mul K, Voermans NC, Lemmers RJLF, Jonker MA, van der Vliet PJ, Padberg GW, et al. 2018; Phenotype-genotype relations in facioscapulohumeral muscular dystrophy type 1. Clin Genet. 94:521–7. DOI: 10.1111/cge.13446. PMID: 30211448.
Article13. Statland JM, Tawil R. 2014; Risk of functional impairment in facioscapulohumeral muscular dystrophy. Muscle Nerve. 49:520–7. DOI: 10.1002/mus.23949. PMID: 23873337.
Article14. Lunt PW, Jardine PE, Koch M, Maynard J, Osborn M, Williams M, et al. 1995; Phenotypic-genotypic correlation will assist genetic counseling in 4q35-facioscapulohumeral muscular dystrophy. Muscle Nerve Suppl. 2:S103–9. DOI: 10.1002/mus.880181319. PMID: 7739619.
Article15. Banerji CRS, Cammish P, Evangelista T, Zammit PS, Straub V, Marini-Bettolo C. 2020; Facioscapulohumeral muscular dystrophy 1 patients participating in the UK FSHD registry can be subdivided into 4 patterns of self-reported symptoms. Neuromuscul Disord. 30:315–28. DOI: 10.1016/j.nmd.2020.03.001. PMID: 32327287.
Article16. Lin F, Wang ZQ, Lin MT, Murong SX, Wang N. 2015; New insights into genotype-phenotype correlations in Chinese facioscapulohumeral muscular dystrophy: a retrospective analysis of 178 patients. Chin Med J (Engl). 128:1707–13. DOI: 10.4103/0366-6999.159336. PMID: 26112708. PMCID: PMC4733718. PMID: 4cd7d6ae0ac34356886360b845d5fdb0.17. Lemmers RJLF, O'Shea S, Padberg GW, Lunt PW, van der Maarel SM. 2012; Best practice guidelines on genetic diagnostics of facioscapulohumeral muscular dystrophy: workshop 9th June 2010, LUMC, Leiden, The Netherlands. Neuromuscul Disord. 22:463–70. DOI: 10.1016/j.nmd.2011.09.004. PMID: 22177830.
Article18. Lemmers RJLF, Osborn M, Haaf T, Rogers M, Frants RR, Padberg GW, et al. 2003; D4F104S1 deletion in facioscapulohumeral muscular dystrophy: phenotype, size, and detection. Neurology. 61:178–83. DOI: 10.1212/01.WNL.0000078889.51444.81. PMID: 12874395.
Article19. Lemmers RJLF, van der Wielen MJR, Bakker E, Padberg GW, Frants RR, van der Maarel SM. 2004; Somatic mosaicism in FSHD often goes undetected. Ann Neurol. 55:845–50. DOI: 10.1002/ana.20106. PMID: 15174019.
Article20. Stence AA, Thomason JG, Pruessner JA, Sompallae RR, Snow AN, Ma D, et al. 2021; Validation of optical genome mapping for the molecular diagnosis of facioscapulohumeral muscular dystrophy. J Mol Diagn. 23:1506–14. DOI: 10.1016/j.jmoldx.2021.07.021. PMID: 34384893. PMCID: PMC8647435.
Article21. Zhang Q, Xu X, Ding L, Li H, Xu C, Gong Y, et al. 2019; Clinical application of single-molecule optical mapping to a multigeneration FSHD1 pedigree. Mol Genet Genomic Med. 7:e565. DOI: 10.1002/mgg3.565. PMID: 30666819. PMCID: PMC6418370.
Article22. Dai Y, Li P, Wang Z, Liang F, Yang F, Fang L, et al. 2020; Single-molecule optical mapping enables quantitative measurement of D4Z4 repeats in facioscapulohumeral muscular dystrophy (FSHD). J Med Genet. 57:109–20. DOI: 10.1136/jmedgenet-2019-106078. PMID: 31506324. PMCID: PMC7029236.
Article23. Mitsuhashi S, Nakagawa S, Takahashi Ueda M, Imanishi T, Frith MC, Mitsuhashi H. 2017; Nanopore-based single molecule sequencing of the D4Z4 array responsible for facioscapulohumeral muscular dystrophy. Sci Rep. 7:14789. DOI: 10.1038/s41598-017-13712-6. PMID: 29093467. PMCID: PMC5665936.
Article24. Delourme M, Charlene C, Gerard L, Ganne B, Perrin P, Vovan C, et al. 2023; Complex 4q35 and 10q26 rearrangements: a challenge for molecular diagnosis of patients with facioscapulohumeral dystrophy. Neurol Genet. 9:e200076. DOI: 10.1212/NXG.0000000000200076. PMID: 37200893. PMCID: PMC10188231.25. Ricci E, Galluzzi G, Deidda G, Cacurri S, Colantoni L, Merico B, et al. 1999; Progress in the molecular diagnosis of facioscapulohumeral muscular dystrophy and correlation between the number of KpnI repeats at the 4q35 locus and clinical phenotype. Ann Neurol. 45:751–7. DOI: 10.1002/1531-8249(199906)45:6<751::AID-ANA9>3.0.CO;2-M. PMID: 10360767.26. van Overveld PGM, Enthoven L, Ricci E, Rossi M, Felicetti L, Jeanpierre M, et al. 2005; Variable hypomethylation of D4Z4 in facioscapulohumeral muscular dystrophy. Ann Neurol. 58:569–76. DOI: 10.1002/ana.20625. PMID: 16178028.
Article27. Park HJ, Hong JM, Lee JH, Lee HS, Shin HY, Kim SM, et al. 2015; Low D4Z4 copy number and gender difference in Korean patients with facioscapulohumeral muscular dystrophy type 1. Neuromuscul Disord. 25:859–64. DOI: 10.1016/j.nmd.2015.08.004. PMID: 26319123.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Application of Optical Genome Mapping to the Genetic Diagnosis of Facioscapulohumeral Muscular Dystrophy 1
- Facioscapulohumeral muscular dystrophy: report of two cases
- Facioscapulohumeral Muscular Dystrophy Confirmedby D4Z4 Analysis
- Shoulder Motion after Scapulothoracic Arthrodesis of the Facioscapulohumeral Type of Progressive Muscular Dystrophy ( PMD )
- Extensive inflammatory reaction in facioscapulohumeral muscular dystrophy
