Surgical and wound management for hand-localized kaposiform hemangioendothelioma: a case report
- Affiliations
-
- 1Department of Plastic and Reconstructive Surgery, Institute for Human Tissue Restoration, Yonsei University, College of Medicine, Seoul, Korea
- KMID: 2558742
- DOI: http://doi.org/10.12790/ahm.24.0021
Abstract
- Kaposiform hemangioendothelioma (KHE) is a rare, aggressive vascular tumor predominantly seen in children. It can infiltrate the deeper soft tissues and is clinically marked by erythematous to violet plaques, sometimes associated with the Kasabach-Merritt phenomenon. A male neonate presented with a substantial mass on the dorsum of his left hand. Surgical excision on the 8th day after birth identified the tumor as KHE, without evidence of Kasabach-Merritt syndrome. Two additional operations were performed over the following year to address contractures and restore finger function. At a 6-month follow-up, the patient showed no significant functional impairment. KHE poses unique clinical challenges due to its aggressive nature. This case highlights the need for prompt surgical intervention, given the tumor’s size and location. Managing KHE requires a rapid diagnosis and intervention, particularly in functionally critical areas, to ensure optimal outcomes.
Keyword
Figure
-
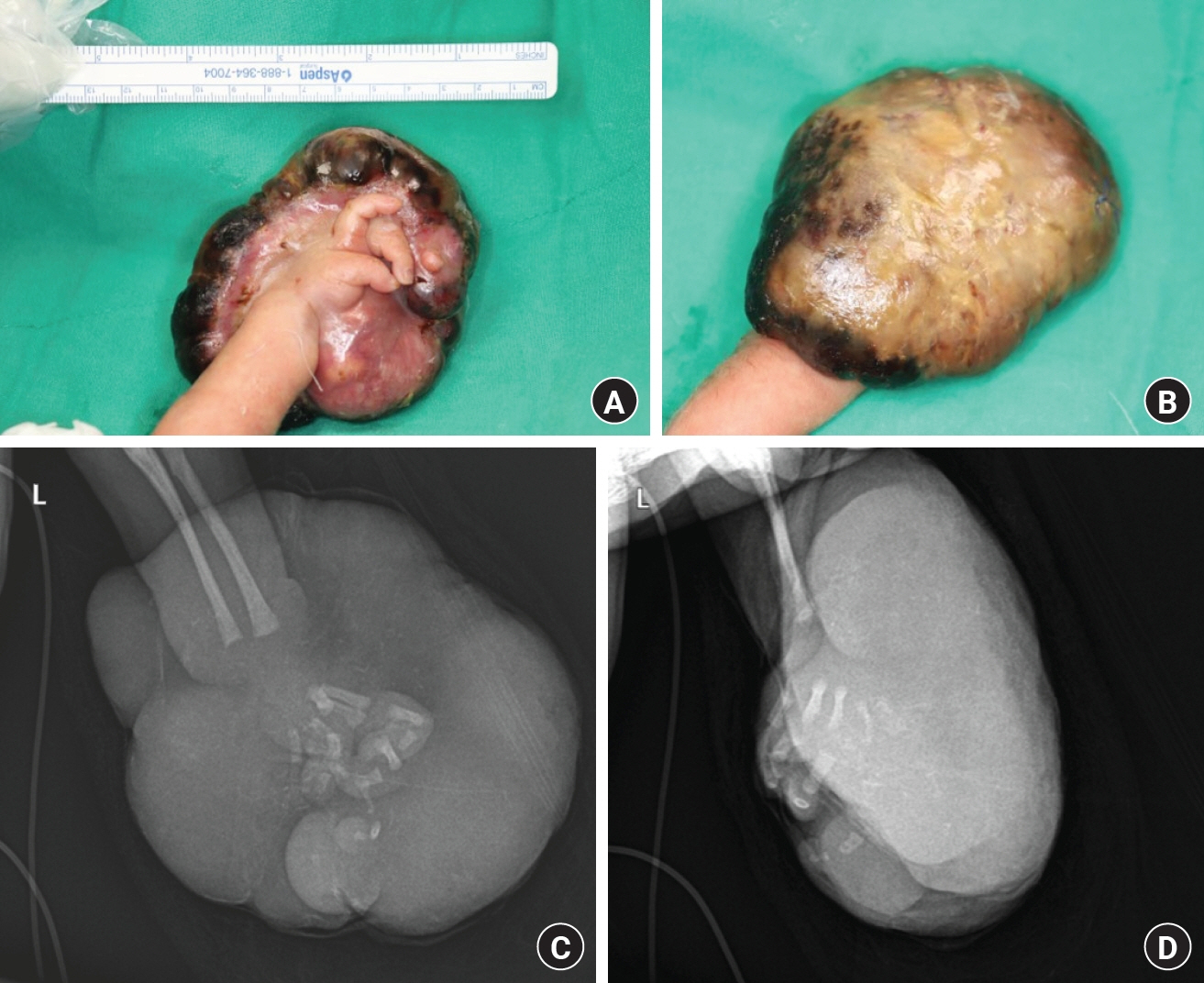
Fig. 1. Preoperative evaluation of the neonate’s lesion. (A, B) Gross photographs depicting the substantial mass on the dorsum of the left hand prior to surgical intervention. (C, D) X-ray images showing the internal structure and extent of the lesion on the affected arm, providing essential diagnostic information.
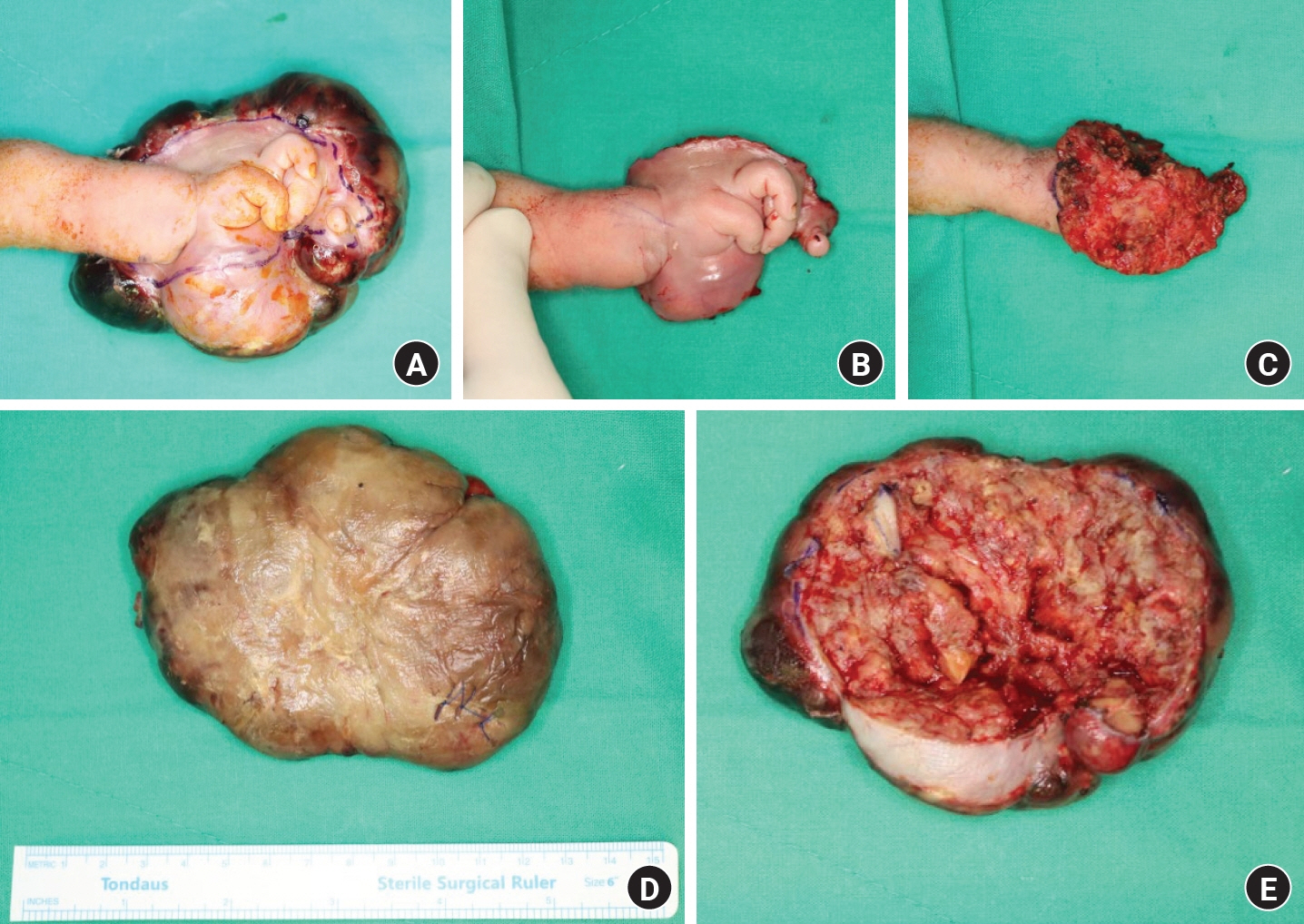
Fig. 2. Surgical management of kaposiform hemangioendothelioma. (A) Intraoperative design marking the boundaries for tumor resection. (B, C) Immediate postoperative photographs illustrating the initial outcome following tumor excision. (D, E) Photographs of the excised specimen, confirming the diagnosis of kaposiform hemangioendothelioma.

Fig. 3. Postoperative follow-up at 3 months. (A, B) Images of the patient’s left hand demonstrating moderate scar contracture, which necessitated further surgical intervention for contracture release.
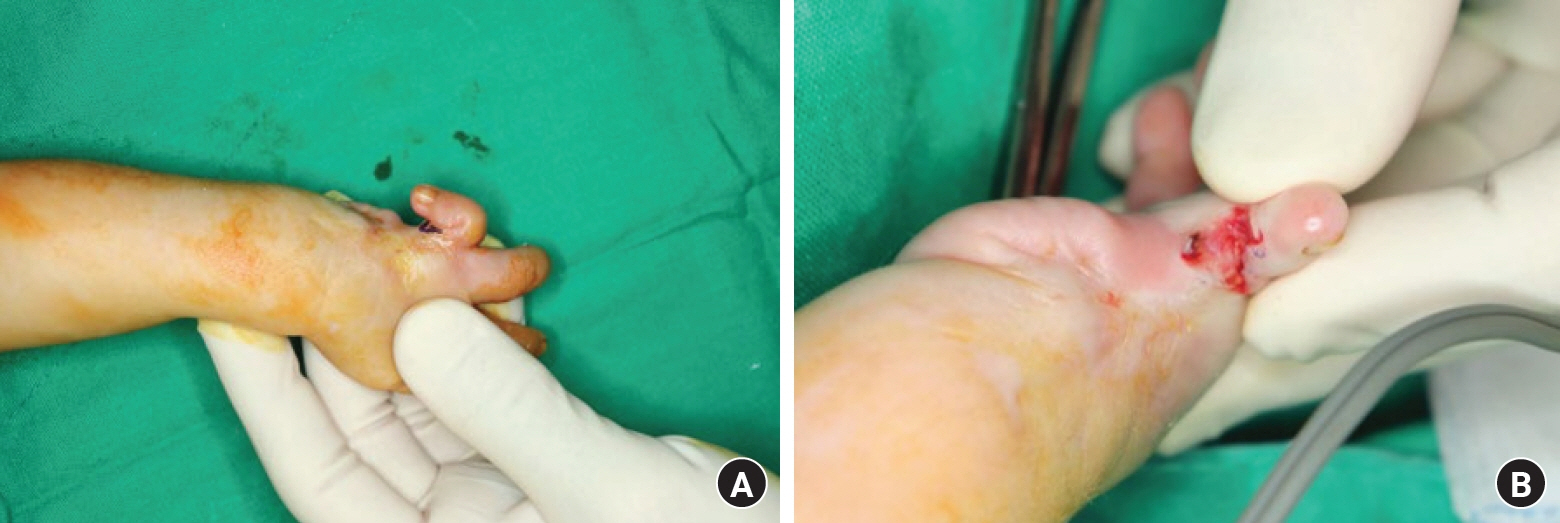
Fig. 4. Preoperative and postoperative photographs of the second operation. (A) Severe scar contracture was noted before surgery, and (B) partial scar contracture release with a MatriDerm graft (MedSkin Solutions Dr. Suwelack AG, Billerbeck, Germany) was done in the second operation.
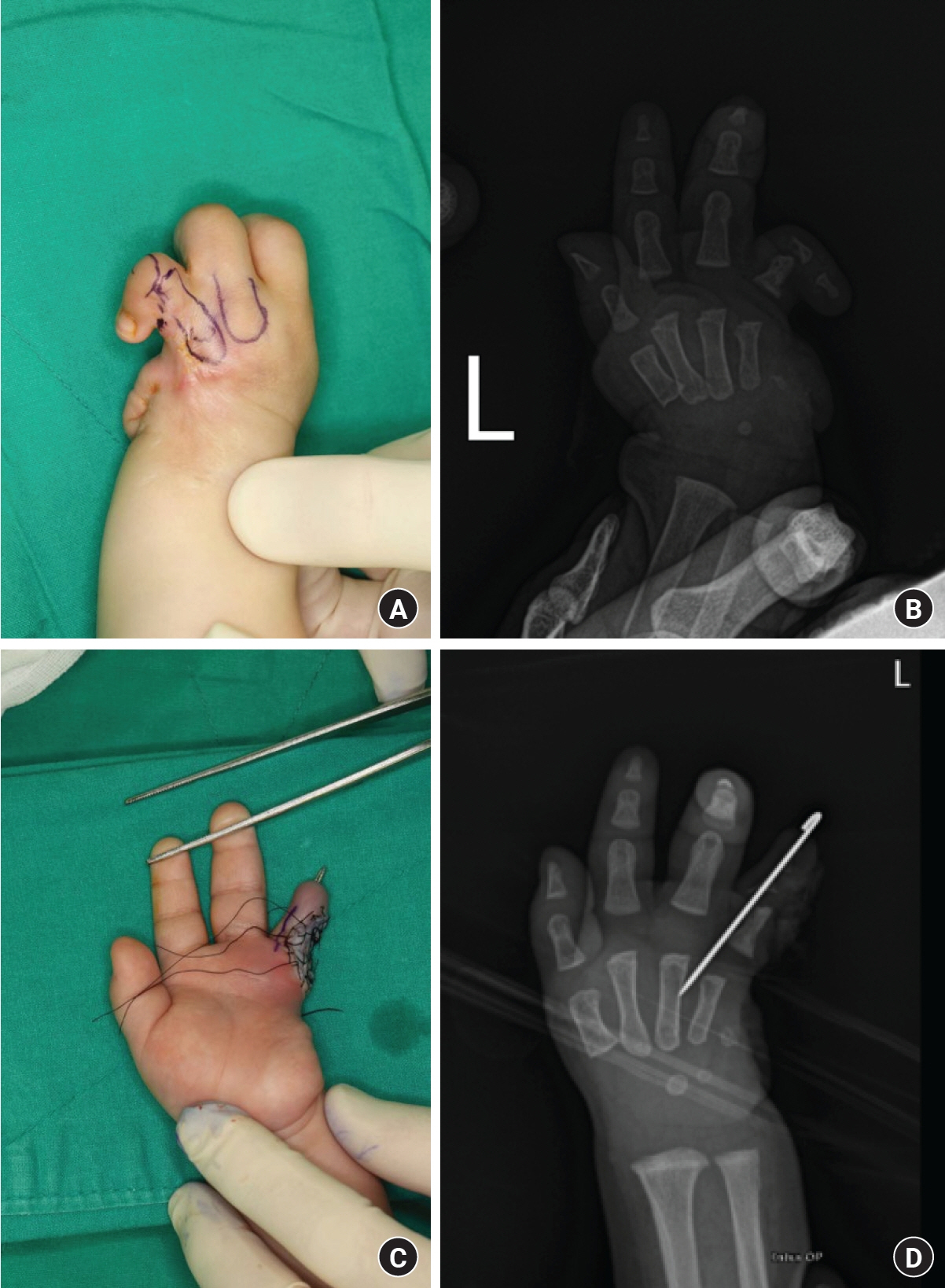
Fig. 5. Preoperative and postoperative photographs of the third operation. (A) The preoperative design shows the metacarpal bones, (B) preoperative X-ray, (C) immediate postoperative photograph with a full-thickness skin graft and Kirschner wire (K-wire) fixation, and (D) postoperative X-ray showing a K-wire.
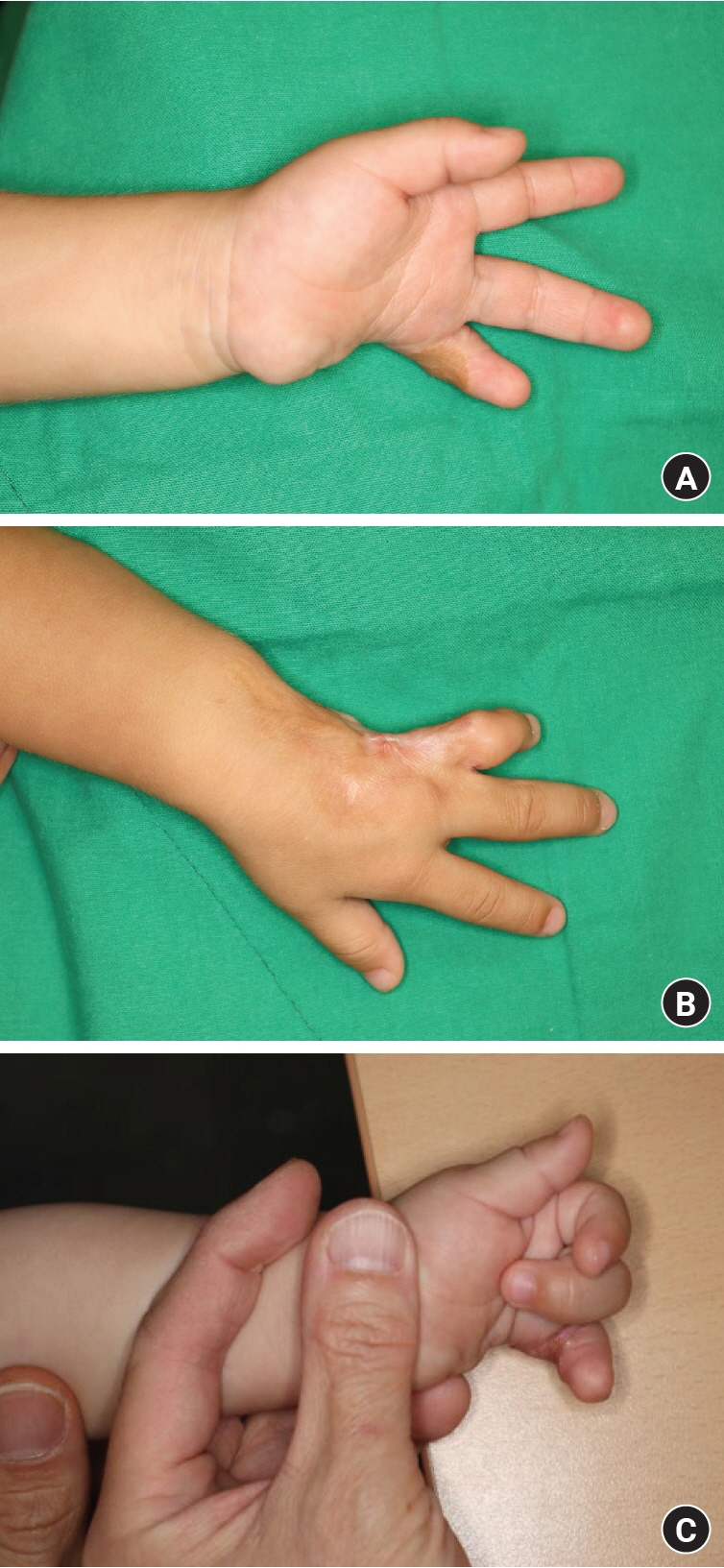
Fig. 6. Outcome after the third surgical intervention. (A, B) Photographs of the patient’s left hand taken 3 months after the third operation, which involved scar contracture release and coverage with a full-thickness skin graft. These images show full recovery of the remaining fingers with no remaining contracture. (C) Photograph of the patient’s left hand with the ring finger flexion, showing intact function of the proximal phalangeal joint.
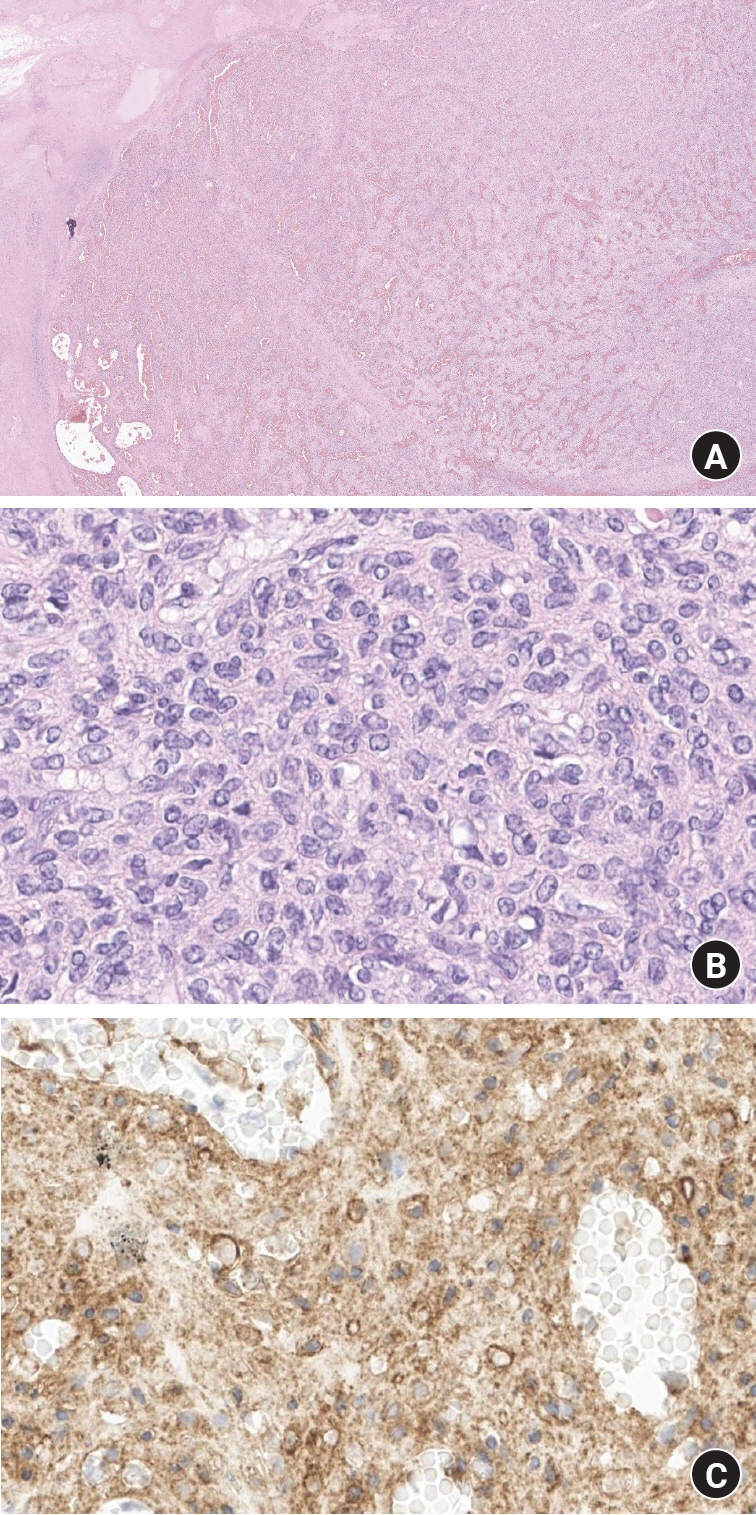
Fig. 7. Histopathological features of kaposiform hemangioendothelioma. (A) Overview showing a capillary hemangioma-like multinodular mass. Hematoxylin and eosin (H&E) stain, ×15. (B) Higher magnification displaying mild to moderate nuclear pleomorphism with rare mitotic figures. H&E stain, ×400. (C) Immunohistochemical staining showing diffuse cytoplasmic positivity, indicating vascular endothelial differentiation in tumor cells. CD34 stain, ×400.
Reference
-
References
1. Cinotti E, Rongioletti F. Kaposiform hemangioendothelioma. In : Rongioletti F, Margaritescu I, Smoller BR, editors. Rare malignant skin tumors. New York, NY: Springer New York;2014. p. 161–3.2. Barabash-Neila R, García-Rodríguez E, Bernabeu-Wittel J, Bueno-Rodríguez I, Ramírez-Villar G, López-Gutierrez JC. Kaposiform hemangioendothelioma with Kasabach-Merritt phenomenon: successful treatment with vincristine and ticlopidine. Indian J Pediatr. 2012; 79:1386–7.
Article3. Lyons LL, North PE, Mac-Moune Lai F, Stoler MH, Folpe AL, Weiss SW. Kaposiform hemangioendothelioma: a study of 33 cases emphasizing its pathologic, immunophenotypic, and biologic uniqueness from juvenile hemangioma. Am J Surg Pathol. 2004; 28:559–68.4. Zukerberg LR, Nickoloff BJ, Weiss SW. Kaposiform hemangioendothelioma of infancy and childhood. An aggressive neoplasm associated with Kasabach-Merritt syndrome and lymphangiomatosis. Am J Surg Pathol. 1993; 17:321–8.5. Croteau SE, Liang MG, Kozakewich HP, et al. Kaposiform hemangioendothelioma: atypical features and risks of Kasabach-Merritt phenomenon in 107 referrals. J Pediatr. 2013; 162:142–7.
Article6. Cooper JG, Edwards SL, Holmes JD. Kaposiform haemangioendothelioma: case report and review of the literature. Br J Plast Surg. 2002; 55:163–5.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Effective Management of Kaposiform Hemangioendotheliomas Associatedwith Kasabach-Merritt Syndrome Using Chemotherapy
- Kaposiform Hemangioendothelioma Complicated by Kasabach - Merritt Phenomenon with Bone Involvement in an Adult
- Cerebellopontine Angle Kaposiform Hemangioendothelioma: A Case Report
- Composite Hemangioendothelioma: A Case Report
- A Case of Hemangioendothelioma on the Nasal Septum
