Programmed Follow-up and Quality Control of Treatment Techniques Enhance Chronic Thromboembolic Pulmonary Hypertension Management: Lessons From a Multidisciplinary Team
- Affiliations
-
- 1Division of Cardiology, Department of Internal Medicine, Heart Vascular Stroke Institute, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea
- 2Department of Radiology, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea
- 3Division of Nuclear Medicine, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea
- 4Division of Pulmonology and Critical Care Medicine, Department of Internal Medicine, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea
- 5Division of Thoracic and Cardiovascular Surgery, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea
- 6Division of Cardiology, Department of Internal Medicine, Samsung Changwon Hospital, Sungkyunkwan University School of Medicine, Changwon, Korea
- KMID: 2557981
- DOI: http://doi.org/10.4070/kcj.2024.0021
Abstract
- Background and Objectives
The recent developments in chronic thromboembolic pulmonary hypertension (CTEPH) are emphasizing the multidisciplinary team. We report on the changes in clinical practice following the development of a multidisciplinary team, based on our 7 years of experience.
Methods
Multidisciplinary team was established in 2015 offering both balloon pulmonary angioplasty (BPA) and pulmonary endarterectomy (PEA) with technical upgrades by internal and external expertise. For operable cases, PEA was recommended as the primary treatment modality, followed by pulmonary angiography and right heart catheterization after 6 months to evaluate treatment effect and identify patients requiring further BPA. For patients with inoperable anatomy or high surgical risk, BPA was recommended as the initial treatment modality. Patient data and clinical outcomes were closely monitored.
Results
The number of CTEPH treatments rapidly increased and postoperative survival improved after team development. Before the team, 38 patients were treated by PEA for 18 years; however, 125 patients were treated by PEA or BPA after the team for 7 years. The number of PEA performed was 64 and that of BPA 342 sessions. World Health Organization functional class I or II was achieved in 93% of patients. The patients treated with PEA was younger, male dominant, higher pulmonary artery pressure, and smaller cardiac index, than BPA-only patients. In-hospital death after PEA was only 1 case and none after BPA.
Conclusions
The balanced development of BPA and PEA through a multidisciplinary team approach proved synergistic in increasing the number of actively treated CTEPH patients and improving clinical outcomes.
Keyword
Figure
-
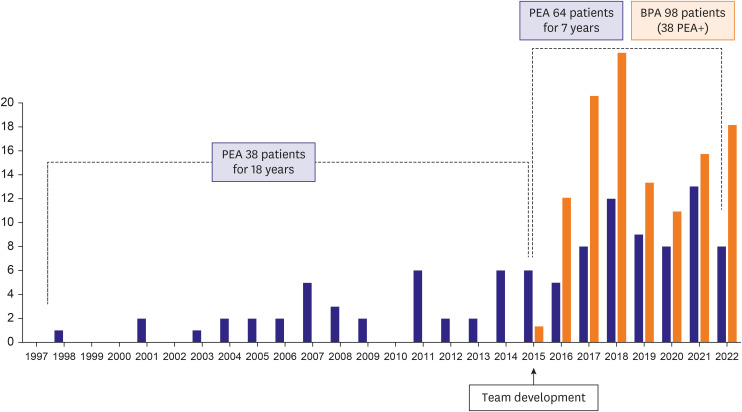
Figure 1 Number of CTEPH patients before and after CTEPH team development. The annual number of PEA cases is represented by the blue bar, while the orange bar represents the annual number of BPA cases.BPA = balloon pulmonary angioplasty; CTEPH = chronic thromboembolic pulmonary hypertension; PEA = pulmonary endarterectomy.
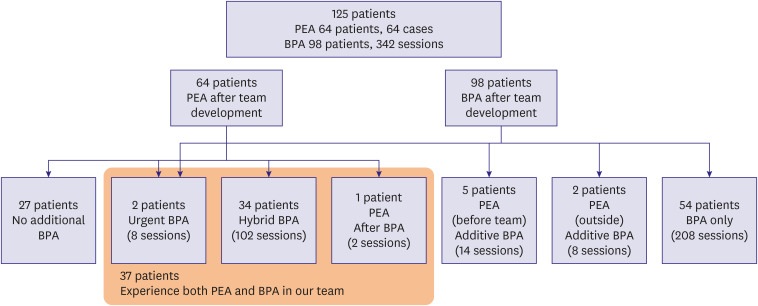
Figure 2 Details of treatment of chronic thromboembolic pulmonary hypertension patients after multidisciplinary team development.BPA = balloon pulmonary angioplasty; PEA = pulmonary endarterectomy.
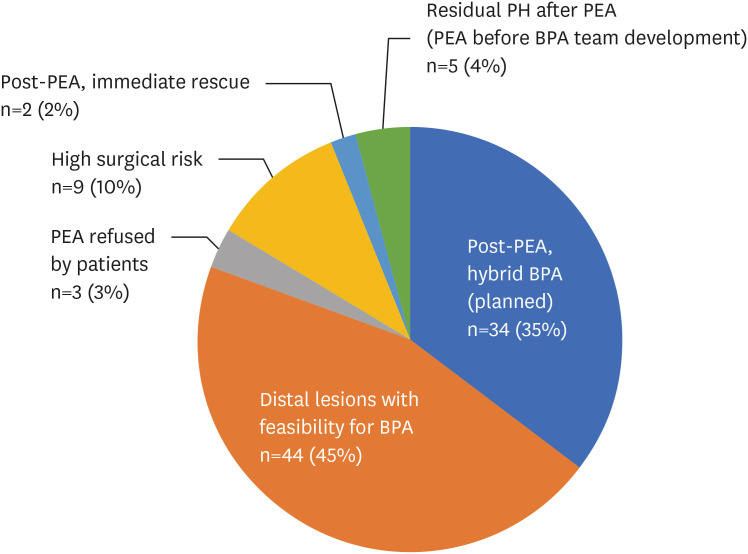
Figure 3 The reasons for performing BPA.BPA = balloon pulmonary angioplasty; PEA = pulmonary endarterectomy; PH = pulmonary hypertension.
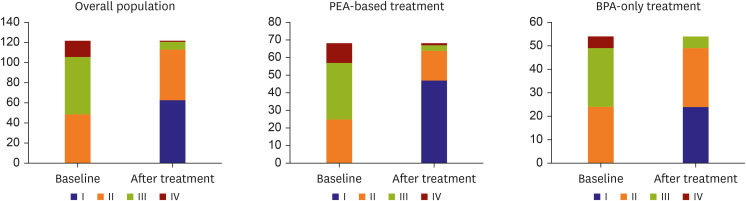
Figure 4 Functional improvement after treatment in overall population and by treatment strategy.BPA-only = patients who were treated exclusively with balloon pulmonary angioplasty without surgery; PEA-based = patients who were treated with pulmonary endarterectomy with or without balloon pulmonary angioplasty.
Cited by 1 articles
-
Multidisciplinary Team Approach for the Management of Chronic Thromboembolic Pulmonary Hypertension
Hiromi Matsubara
Korean Circ J. 2024;54(7):422-424. doi: 10.4070/kcj.2024.0193.
Reference
-
1. Kim NH, Delcroix M, Jenkins DP, et al. Chronic thromboembolic pulmonary hypertension. J Am Coll Cardiol. 2013; 62:D92–D99. PMID: 24355646.
Article2. Jenkins D, Madani M, Fadel E, D’Armini AM, Mayer E. Pulmonary endarterectomy in the management of chronic thromboembolic pulmonary hypertension. Eur Respir Rev. 2017; 26:160111. PMID: 28298388.
Article3. Ogawa A, Satoh T, Fukuda T, et al. Balloon pulmonary angioplasty for chronic thromboembolic pulmonary hypertension: results of a multicenter registry. Circ Cardiovasc Qual Outcomes. 2017; 10:e004029. PMID: 29101270.
Article4. Kurzyna M, Darocha S, Pietura R, et al. Changing the strategy of balloon pulmonary angioplasty resulted in a reduced complication rate in patients with chronic thromboembolic pulmonary hypertension. A single-centre European experience. Kardiol Pol. 2017; 75:645–654. PMID: 28553870.5. Guth S, D’Armini AM, Delcroix M, et al. Current strategies for managing chronic thromboembolic pulmonary hypertension: results of the worldwide prospective CTEPH Registry. ERJ Open Res. 2021; 7:00850-2020. PMID: 34409094.
Article6. Delcroix M, Torbicki A, Gopalan D, et al. ERS statement on chronic thromboembolic pulmonary hypertension. Eur Respir J. 2021; 57:2002828. PMID: 33334946.
Article7. Ghofrani HA, Simonneau G, D’Armini AM, et al. Macitentan for the treatment of inoperable chronic thromboembolic pulmonary hypertension (MERIT-1): results from the multicentre, phase 2, randomised, double-blind, placebo-controlled study. Lancet Respir Med. 2024; 12:e21–e30. PMID: 38548406.8. Simonneau G, D’Armini AM, Ghofrani HA, et al. Riociguat for the treatment of chronic thromboembolic pulmonary hypertension: a long-term extension study (CHEST-2). Eur Respir J. 2015; 45:1293–1302. PMID: 25395036.
Article9. Kim NH, Papamatheakis DG, Fernandes TM. Evolution of randomized, controlled studies of medical therapy in chronic thromboembolic pulmonary hypertension. Pulm Circ. 2021; 11:20458940211007373. PMID: 34104419.10. Humbert M, Kovacs G, Hoeper MM, et al. 2022 ESC/ERS guidelines for the diagnosis and treatment of pulmonary hypertension. Eur Heart J. 2022; 43:3618–3731. PMID: 36017548.11. Martin-Suarez S, Loforte A, Cavalli GG, et al. Therapeutic alternatives in chronic thromboembolic pulmonary hypertension: from pulmonary endarterectomy to balloon pulmonary angioplasty to medical therapy. State of the art from a multidisciplinary team. Ann Cardiothorac Surg. 2022; 11:120–127. PMID: 35433353.
Article12. Madani MM, Auger WR, Pretorius V, et al. Pulmonary endarterectomy: recent changes in a single institution’s experience of more than 2,700 patients. Ann Thorac Surg. 2012; 94:97–103. PMID: 22626752.
Article13. Poch DS, Mahmud E, Patel M, et al. Patient selection for balloon pulmonary angioplasty: six-year results from a high volume PTE surgical center. Pulm Circ. 2022; 12:e12148. PMID: 36325508.
Article14. Liu HY, Wu YJ, Huang SC, Liu CL, Hsu HH, Yu CJ. Experiences with pulmonary endarterectomy for chronic thromboembolic pulmonary hypertension at multiple centers in Taiwan. J Formos Med Assoc. 2022; 121:604–612. PMID: 34373177.15. Bashar Izzat M, Almohammad F, Raslan AF. A survey on pulmonary thromboendarterectomy in the Asia-Pacific region. Asian Cardiovasc Thorac Ann. 2017; 25:345–349. PMID: 28457173.
Article16. Oh DK, Song JM, Park DW, et al. The effect of a multidisciplinary team on the implementation rates of major diagnostic and therapeutic procedures of chronic thromboembolic pulmonary hypertension. Heart Lung. 2019; 48:28–33. PMID: 30115494.
Article17. Barco S, Klok FA, Konstantinides SV, et al. Sex-specific differences in chronic thromboembolic pulmonary hypertension. Results from the European CTEPH registry. J Thromb Haemost. 2020; 18:151–161. PMID: 31479557.
Article18. Hu S, Tan JS, Liu S, et al. The long-term survival in patients with chronic thromboembolic pulmonary hypertension: experience from a single center in China. J Thromb Thrombolysis. 2022; 53:926–933. PMID: 34705198.
Article19. Siennicka A, Darocha S, Banaszkiewicz M, et al. Treatment of chronic thromboembolic pulmonary hypertension in a multidisciplinary team. Ther Adv Respir Dis. 2019; 13:1753466619891529. PMID: 31878837.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Multidisciplinary Team Approach for the Management of Chronic Thromboembolic Pulmonary Hypertension
- The Role of Lung Ventilation/Perfusion Scan in the Management of Chronic Thromboembolic Pulmonary Hypertension
- Clinical Year in Review of Pulmonary Vascular Disease
- A Case of Computed Tomography Angiography Imaging of Chronic Thromboembolic Pulmonary Hypertension Secondary to Patent Ductus Arteriosus
- Pulmonary arterial hypertension due to antiphospholipid syndrome initially mimicking chronic thromboembolic pulmonary hypertension
