Measurement of Knee Extensor Torque During Repetitive Peripheral Magnetic Stimulation: Comparison of the Forces Induced by Different Stimulators
- Affiliations
-
- 1Doctoral Program in Rehabilitation, Graduate School of Health Science and Technology, Kawasaki University of Medical Welfare, Kurashiki, Japan
- 2Department of Physical Therapy, Faculty of Rehabilitation, Kawasaki University of Medical Welfare, Kurashiki, Japan
- 3Department of Occupational Therapy, Faculty of Rehabilitation, Kawasaki University of Medical Welfare, Kurashiki, Japan
- KMID: 2557067
- DOI: http://doi.org/10.5535/arm.230025
Abstract
Objective
To investigate the factors that induce strong contractions during repetitive peripheral magnetic stimulation (rPMS) and compare the muscle torque induced by two stimulators (Stim A and Stim B) with different coil properties.
Methods
rPMS was applied to the right vastus lateralis of 30 healthy young adults. Stim A contained a 10.1 cm2 rectangular iron core coil, while Stim B contained a 191 cm2 round coil. The knee extensor torque (KET) induced by rPMS at 30 Hz was measured isometrically and divided by the maximum voluntary contraction (MVC) to obtain a relative value of MVC (%MVC). KET at 100% intensity of Stim A (A100%, 1.08 T) was compared to those at 100% or 70% intensity of Stim B (B100%, 1.47 T vs. B70%, 1.07 T). Additionally, we conducted a comprehensive literature search for studies that measured the KET during rPMS.
Results
Both the mean values of %MVC using B100% and B70% were significantly greater than that using A100%. Furthermore, the KET induced by Stim B was found to be larger than that described in previous reports, unless booster units were used to directly stimulate the main trunk of the femoral nerve.
Conclusion
Stim B induced a stronger muscle contraction force than Stim A did. This may be because the larger the coil area, the wider the area that can be stimulated. Additionally, a circular coil allows for deeper stimulation.
Figure
-
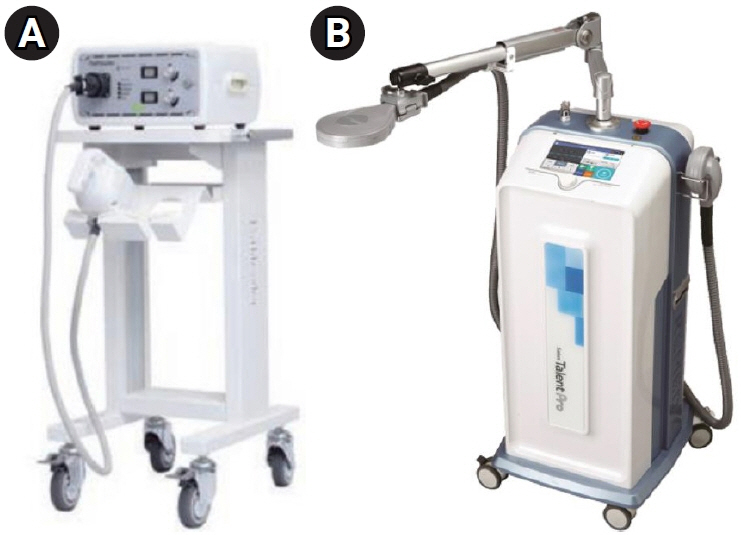
Fig. 1. Magnetic stimulators used for muscle contraction. (A) Air-cooled type stimulator manufactured by IFG Co. Ltd. (Stim A). (B) Oil-cooled type stimulator manufactured by REMED Co. Ltd. (Stim B).

Fig. 2. Muscle contraction induced by repetitive peripheral magnetic stimulation and measurement of muscle torque. (A) Contraction induced by the stimulator manufactured by IFG Co. Ltd. (Stim A). (B) Contraction induced by the stimulator manufactured by REMED Co. Ltd. (Stim B).
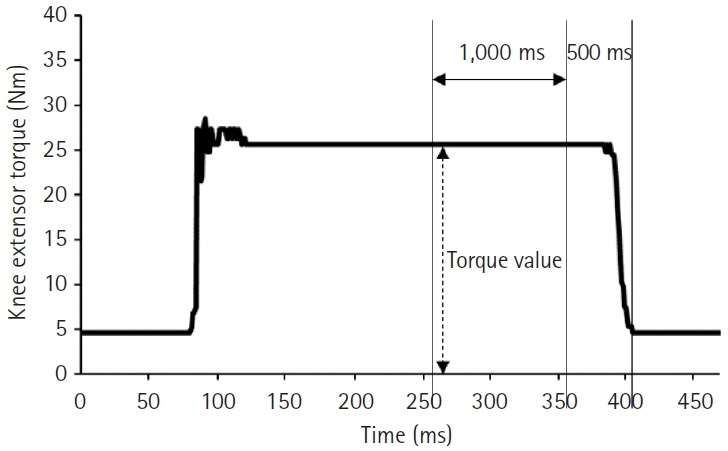
Fig. 3. Knee extensor torque waveform during repetitive peripheral magnetic stimulation. Torque value: mean torque for 1 second from 500 to 1,500 ms before the waveform returned to baseline after contraction.
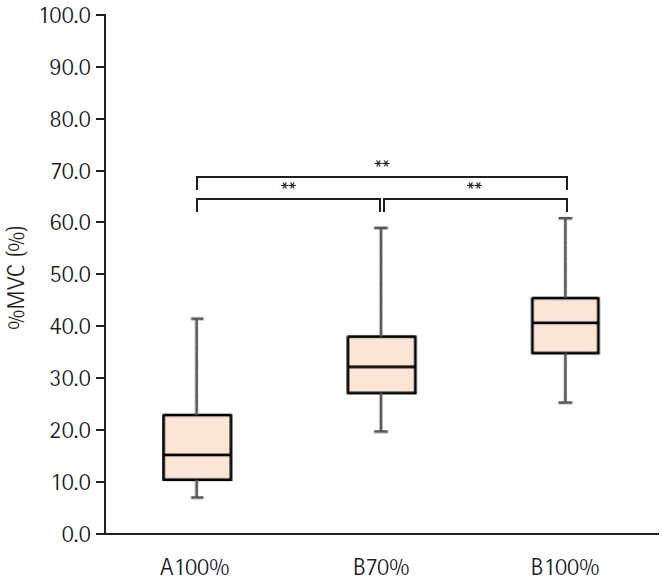
Fig. 4. Comparison of relative value of maximum voluntary contraction (%MVC) during repetitive peripheral magnetic stimulation between each stimulation condition. %MVC was calculated by dividing the knee extensor torque during stimulation by the MVC. A100%, maximum output intensity of the stimulator manufactured by IFG Co. Ltd. (Stim A); B70%, 70% of maximum output intensity of the stimulator manufactured by REMED Co. Ltd. (Stim B); B100%, maximum output intensity of the Stim B. **p<0.01.
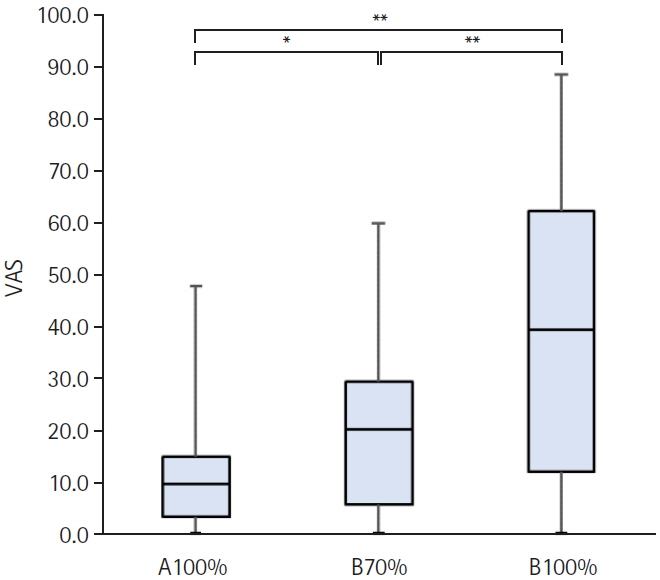
Fig. 5. Comparison of pain during repetitive peripheral magnetic stimulation in each stimulation condition. A100%, maximum output intensity of the stimulator manufactured by IFG Co. Ltd. (Stim A); B70%, 70% of maximum output intensity of the stimulator manufactured by REMED Co. Ltd. (Stim B); B100%, maximum output intensity of the Stim B; VAS, visual analogue scale. *p<0.05, **p<0.01.

Reference
-
1. Peterson MD, Rhea MR, Sen A, Gordon PM. Resistance exercise for muscular strength in older adults: a meta-analysis. Ageing Res Rev. 2010; 9:226–37.
Article2. Peterson MD, Sen A, Gordon PM. Influence of resistance exercise on lean body mass in aging adults: a meta-analysis. Med Sci Sports Exerc. 2011; 43:249–58.3. Manini TM, Hong SL, Clark BC. Aging and muscle: a neuron's perspective. Curr Opin Clin Nutr Metab Care. 2013; 16:21–6.4. Janssen I, Heymsfield SB, Ross R. Low relative skeletal muscle mass (sarcopenia) in older persons is associated with functional impairment and physical disability. J Am Geriatr Soc. 2002; 50:889–96.
Article5. Delmonico MJ, Harris TB, Visser M, Park SW, Conroy MB, Velasquez-Mieyer P, et al. Longitudinal study of muscle strength, quality, and adipose tissue infiltration. Am J Clin Nutr. 2009; 90:1579–85.
Article6. Krenn M, Haller M, Bijak M, Unger E, Hofer C, Kern H, et al. Safe neuromuscular electrical stimulator designed for the elderly. Artif Organs. 2011; 35:253–6.
Article7. Barker AT, Freeston IL, Jalinous R, Jarratt JA. Magnetic stimulation of the human brain and peripheral nervous system: an introduction and the results of an initial clinical evaluation. Neurosurgery. 1987; 20:100–9.8. Barker AT. An introduction to the basic principles of magnetic nerve stimulation. J Clin Neurophysiol. 1991; 8:26–37.
Article9. Ito T, Tsubahara A, Watanabe S. Use of electrical or magnetic stimulation for generating hip flexion torque. Am J Phys Med Rehabil. 2013; 92:755–61.
Article10. Bustamante V, Casanova J, López de Santamaría E, Mas S, Sellarés J, Gea J, et al. Redox balance following magnetic stimulation training in the quadriceps of patients with severe COPD. Free Radic Res. 2008; 42:939–48.
Article11. Bustamante V, López de Santa María E, Gorostiza A, Jiménez U, Gáldiz JB. Muscle training with repetitive magnetic stimulation of the quadriceps in severe COPD patients. Respir Med. 2010; 104:237–45.
Article12. Yang SS, Jee S, Hwang SL, Sohn MK. Strengthening of quadriceps by neuromuscular magnetic stimulation in healthy subjects. PM R. 2017; 9:767–73.
Article13. Baek J, Park N, Lee B, Jee S, Yang S, Kang S. Effects of repetitive peripheral magnetic stimulation over vastus lateralis in patients after hip replacement surgery. Ann Rehabil Med. 2018; 42:67–75.
Article14. Kinoshita S, Ikeda K, Hama M, Suzuki S, Abo M. Repetitive peripheral magnetic stimulation combined with intensive physical therapy for gait disturbance after hemorrhagic stroke: an open-label case series. Int J Rehabil Res. 2020; 43:235–9.
Article15. Suzuki K, Ito T, Okada Y, Hiraoka T, Hanayama K, Tsubahara A. Preventive effects of repetitive peripheral magnetic stimulation on muscle atrophy in the paretic lower limb of acute stroke patients: a pilot study. Prog Rehabil Med. 2020; 5:20200008.
Article16. Kamiue M, Ito T, Tsubahara A, Kishimoto T. Development of high-frequency magnetic stimulator to induce stronger knee extension torque. Kawasaki J Med Welf. 2022; 28:29–38.17. Tsubahara A, Kamiue M, Ito T, Kishimoto T, Kurozumi C. Measurement of maximal muscle contraction force induced by high-frequency magnetic stimulation: a preliminary study on the identification of the optimal stimulation site. Jpn J Compr Rehabil Sci. 2021; 12:27–31.
Article18. Madariaga VB, Manterola AG, Miró EL, Iturri JB. [Magnetic stimulation of the quadriceps: analysis of 2 stimulators used for diagnostic and therapeutic applications]. Arch Bronconeumol. 2007; 43:411–7. Spanish.
Article19. Tomazin K, Verges S, Decorte N, Oulerich A, Millet GY. Effects of coil characteristics for femoral nerve magnetic stimulation. Muscle Nerve. 2010; 41:406–9.
Article20. Tomazin K, Verges S, Decorte N, Oulerich A, Maffiuletti NA, Millet GY. Fat tissue alters quadriceps response to femoral nerve magnetic stimulation. Clin Neurophysiol. 2011; 122:842–7.
Article21. Amassian VE, Maccabee PJ, Cracco RQ. Focal stimulation of human peripheral nerve with the magnetic coil: a comparison with electrical stimulation. Exp Neurol. 1989; 103:282–9.
Article22. Gerdle B, Karlsson S, Crenshaw AG, Fridén J. The relationships between EMG and muscle morphology throughout sustained static knee extension at two submaximal force levels. Acta Physiol Scand. 1997; 160:341–51.
Article23. Caso G, McNurlan MA, Mileva I, Zemlyak A, Mynarcik DC, Gelato MC. Peripheral fat loss and decline in adipogenesis in older humans. Metabolism. 2013; 62:337–40.
Article24. Moreau NG, Simpson KN, Teefey SA, Damiano DL. Muscle architecture predicts maximum strength and is related to activity levels in cerebral palsy. Phys Ther. 2010; 90:1619–30.
Article25. Strasser EM, Draskovits T, Praschak M, Quittan M, Graf A. Association between ultrasound measurements of muscle thickness, pennation angle, echogenicity and skeletal muscle strength in the elderly. Age (Dordr). 2013; 35:2377–88. Erratum in: Age (Dordr) 2013;35:2025-6.
Article26. Toumi H, Best TM, Mazor M, Coursier R, Pinti A, Lespessailles E. Association between individual quadriceps muscle volume/enthesis and patello femoral joint cartilage morphology. Arthritis Res Ther. 2014; 16:R1.
Article27. Han TR, Shin HI, Kim IS. Magnetic stimulation of the quadriceps femoris muscle: comparison of pain with electrical stimulation. Am J Phys Med Rehabil. 2006; 85:593–9.28. Oh KJ, Kim SH, Lee YH, Kim JH, Jung HS, Park TJ, et al. Pain-related evoked potential in healthy adults. Ann Rehabil Med. 2015; 39:108–15.
Article29. Kremenic IJ, Ben-Avi SS, Leonhardt D, McHugh MP. Transcutaneous magnetic stimulation of the quadriceps via the femoral nerve. Muscle Nerve. 2004; 30:379–81.
Article30. Kremenic IJ, Glace BW, Ben-Avi SS, Nicholas SJ, McHugh MP. Central fatigue after cycling evaluated using peripheral magnetic stimulation. Med Sci Sports Exerc. 2009; 41:1461–6.
Article31. Fukunaga T, Johnson CD, Nicholas SJ, McHugh MP. Muscle hypotrophy, not inhibition, is responsible for quadriceps weakness during rehabilitation after anterior cruciate ligament reconstruction. Knee Surg Sports Traumatol Arthrosc. 2019; 27:573–9.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Effects of Repetitive Sit to Stand Training on the Knee Extensor Strength and Walking Ability in Subject with Total Knee Replacement Patients
- Evaluation of Muscle Strength Using Isokinetic Testing and Functional Result after Total Knee Arthroplasty
- Analysis of Torque Curve in Isokinetic Knee Dynamometer
- Comparison between the Electric and Magnetic Stimulations for a Repetitive Nerve Stimulation Test
- Torque Onset Angle of the Knee Extensor as a Predictor of Walking Related Balance in Stroke Patients
