Kosin Med J.
2024 Jun;39(2):127-131. 10.7180/kmj.23.134.
Cardiovascular collapse during transcatheter aortic valve replacement in monitored anesthesia care using an end-tidal carbon dioxide monitor: a case report
- Affiliations
-
- 1Department of Anesthesiology and Pain Medicine, Inje University Busan Paik Hospital, Inje University of College of Medicine, Busan, Korea
- KMID: 2556810
- DOI: http://doi.org/10.7180/kmj.23.134
Abstract
- Capnography is commonly used to monitor respiration during general anesthesia. However, it has limited utility in patients with respiratory distress during sedation. This case report examines capnography use in a transcatheter aortic valve replacement procedure performed on an elderly woman with severe aortic stenosis. A 73-year-old woman with a history of non-ST-elevation myocardial infarction and congenital heart failure presented with severe dyspnea caused by severe aortic stenosis. Transcatheter aortic valve replacement was preferred over surgery due to her comorbidities. Monitored anesthesia care was administered with a capnogram. During the procedure, the patient was sedated with remimazolam, maintaining a bispectral index range of 60–80 and a score of 2 on the Modified Observer’s Assessment of Alertness/Sedation scale. Although irregular breathing patterns and a gradual decrease in oxygen saturation were observed following remimazolam infusion, the patient’s respiration eventually stabilized. However, the patient experienced cardiovascular collapse 45 minutes after sedation began. The arterial carbon dioxide pressure measured by arterial blood gas analysis performed just before resuscitation was 68.4 mmHg. After one cycle of resuscitation, the patient recovered. The procedure was successfully performed under general anesthesia, which was replaced with monitored anesthesia care during resuscitation. Although most monitoring devices have similar utility for both general anesthesia and sedation, capnography has limitations for evaluating respiration during sedation, especially for patients with respiratory distress. Therefore, anesthesiologists or medical staff who provide sedation should not neglect periodical arterial carbon dioxide pressure observations via other methods, such as arterial blood gas analysis.
Keyword
Figure
-
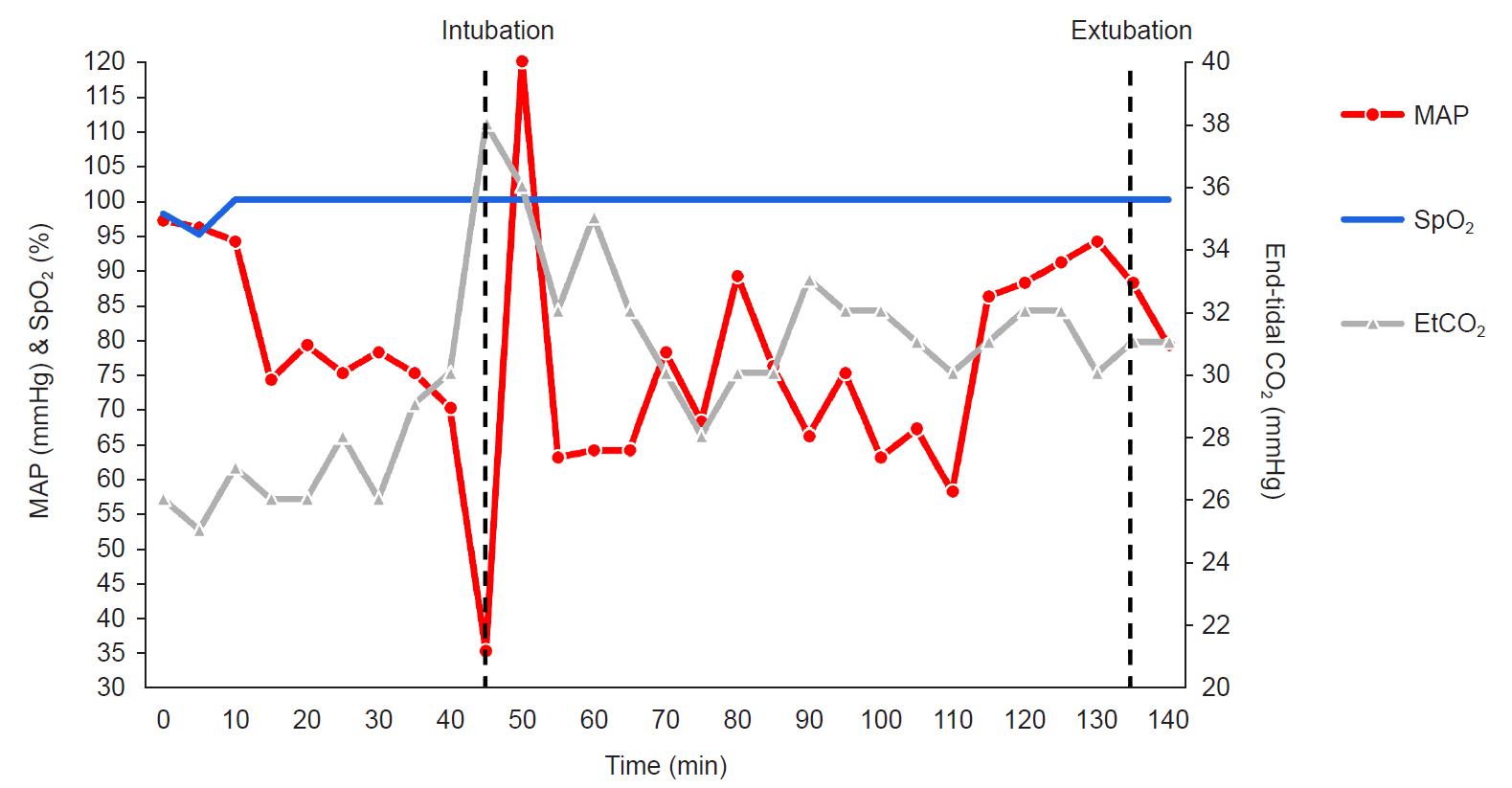
Fig. 1. The MAP gradually decreased until stabilization above 75 mmHg 15 minutes after the initiation of sedation. At 45 minutes after initiation, the MAP decreased to 35 mmHg, at which point the patient required resuscitation. Simultaneously, the patient was intubated, and the EtCO2 value measured using a capnogram was 38 mmHg, whereas the arterial carbon dioxide pressure was 68.4 mmHg. MAP, mean arterial blood pressure; SpO2, pulse oximetry; EtCO2, end-tidal carbon dioxide.
Reference
-
References
1. Butala NM, Chung M, Secemsky EA, Manandhar P, Marquis-Gravel G, Kosinski AS, et al. Conscious sedation versus general anesthesia for transcatheter aortic valve replacement: variation in practice and outcomes. JACC Cardiovasc Interv. 2020; 13:1277–87.2. Kim KM. Remimazolam: pharmacological characteristics and clinical applications in anesthesiology. Anesth Pain Med (Seoul). 2022; 17:1–11.3. Morimoto Y. Efficacy and safety profile of remimazolam for sedation in adults undergoing short surgical procedures. Ther Clin Risk Manag. 2022; 18:95–100.4. American Society of Anesthesiologists (ASA). Standards for basic anesthetic monitoring [Internet]. ASA; c2020 [cited 2023 May 25]. https://www.asahq.org/standards-and-guidelines/standards-for-basic-anesthetic-monitoring.5. Jabre P, Jacob L, Auger H, Jaulin C, Monribot M, Aurore A, et al. Capnography monitoring in nonintubated patients with respiratory distress. Am J Emerg Med. 2009; 27:1056–9.6. Mehta JH, Williams GW 2nd, Harvey BC, Grewal NK, George EE. The relationship between minute ventilation and end tidal CO2 in intubated and spontaneously breathing patients undergoing procedural sedation. PLoS One. 2017; 12:e0180187.7. Ortega R, Connor C, Kim S, Djang R, Patel K. Monitoring ventilation with capnography. N Engl J Med. 2012; 367:e27.8. Chae D, Kim HC, Song Y, Choi YS, Han DW. Pharmacodynamic analysis of intravenous bolus remimazolam for loss of consciousness in patients undergoing general anaesthesia: a randomised, prospective, double-blind study. Br J Anaesth. 2022; 129:49–57.9. Choi BM, Lee JS, Kim KM, Bang JY, Lee EK, Noh GJ. Frequency and characteristics of patients with bispectral index values of 60 or higher during the induction and maintenance of general anesthesia with remimazolam. Sci Rep. 2023; 13:9992.10. Corbo J, Bijur P, Lahn M, Gallagher EJ. Concordance between capnography and arterial blood gas measurements of carbon dioxide in acute asthma. Ann Emerg Med. 2005; 46:323–7.11. Yosefy C, Hay E, Nasri Y, Magen E, Reisin L. End tidal carbon dioxide as a predictor of the arterial PCO2 in the emergency department setting. Emerg Med J. 2004; 21:557–9.12. The Korean Society of Anesthesiologists. Does the measurement of end-tidal carbon dioxide, added to standardized monitoring device for the adult patient during sedation, decrease hypoxia? In: The Korean Society of Anesthesiologists. Clinical Practice Guidelines for Diagnostic and Procedural Sedation. 1st ed. Yeomungak Press; 2022. p. 167-82.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Expanding transcatheter aortic valve replacement into uncharted indications
- The changes of arterial and end-tidal carbon dioxide tension by respiratory rate and tidal volume
- Variation in Arterial to End - Tidal Carbon Dioxide Tension Differences by Duration of Anesthesia and Position during Anesthesia
- Successful Transcatheter Aortic Valve Replacement for Severe Aortic Regurgitation after CARVAR Operation
- The Difference between End-tidal and Arterial PCO2 in Anesthetized Patients
