Treatment of Traumatic Direct Carotid-Cavernous Fistula with a BeGraft-Covered Stent
- Seraj FQM
 1
1 - Najafi S1,2
- Raaisi AA3
- Mirbolouk MH4
- Ebrahimnia F1
- Shamsi HP1
- Garivani Y1
- Zabihyan S1
- Mowla A5
- Baharvahdat H1,3
- Affiliations
-
- 1Department of Neurosurgical, Section of Neurovascular, Ghaem Hospital, Mashhad University of Medical Sciences, Mashhad, Iran
- 2Department of Neurosurgery, Emam Hospital, Mazandaran University of Medical Sciences, School of Medicine, Sari, Iran
- 3Department of Interventional Neuroradiology, Rothschild Foundation Hospital, Paris, France
- 4Department of Neurosurgery, Firouzgar Hospital, Iran University of Medical Sciences, School of Medicine, Tehran, Iran
- 5Division of Stroke and Endovascular Neurosurgery, Department of Neurological Surgery, Keck School of Medicine, University of Southern California (USC), Los Angeles, CA, USA
- KMID: 2556663
- DOI: http://doi.org/10.5469/neuroint.2024.00157
Abstract
- The widely accepted option for treating traumatic direct carotid-cavernous fistula (dCCF) has been endovascular treatment using detachable balloons, coils, or embolic agents. Covered stent deployment has been applied by a few operators and has shown promising results. This is a retrospective study on patients with dCCF treated by an endovascular approach using BeGraft, a covered stent. In 4 cases, this device was successfully deployed without any complications. Immediate complete occlusion was achieved in 3 patients (75%) after deployment of the covered stents. One patient required transvenous coiling for occlusion of the remaining endoleak. Follow-up imaging demonstrated 100% fistula occlusion with complete internal carotid artery patency. No early or late complications occurred following treatment. In conclusion, the BeGraft-covered stent could be a promising safe and effective alternative option for the endovascular treatment of dCCF.
Figure
-
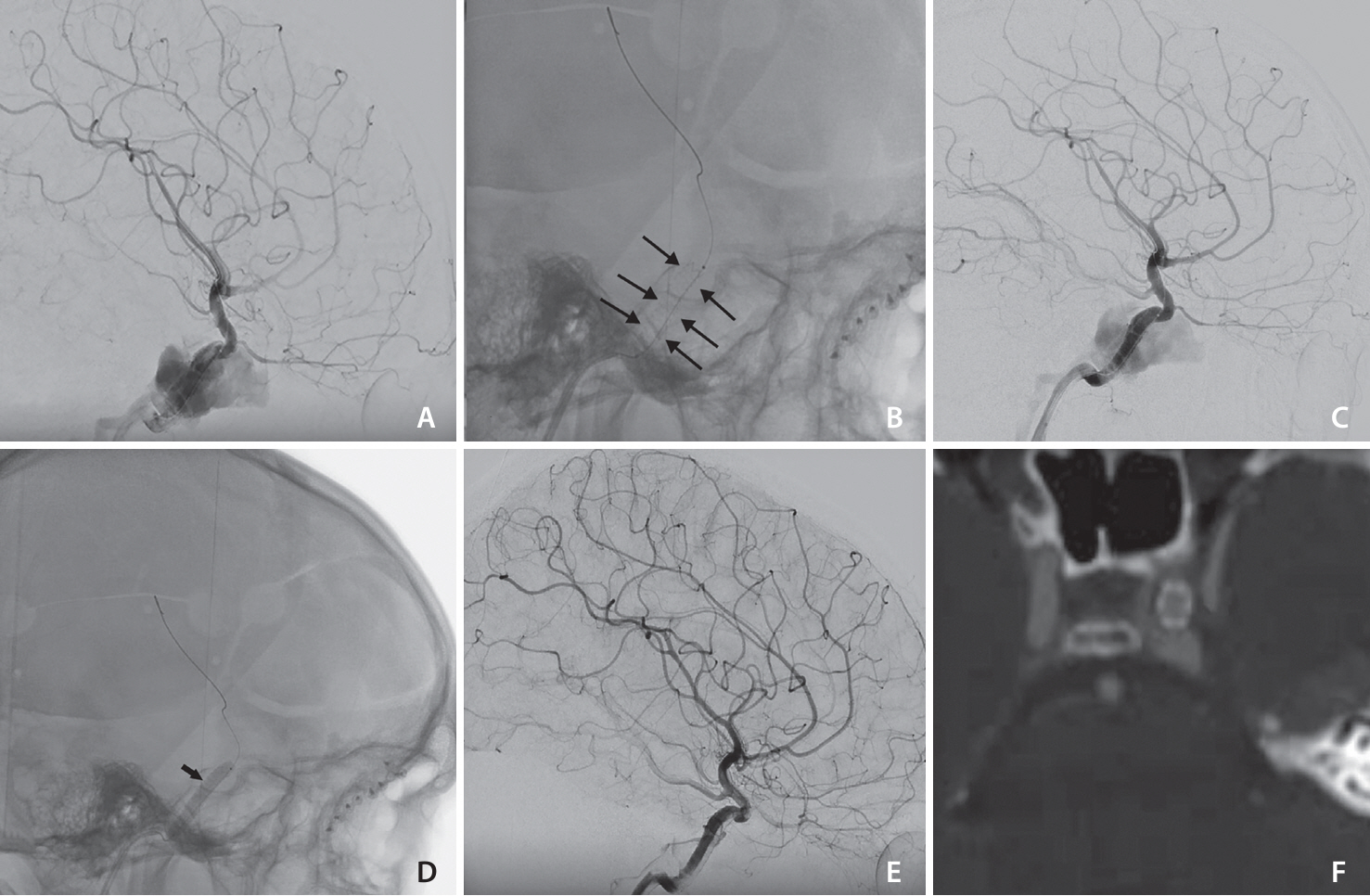
Fig. 1. Patient 4. (A) The lateral view of cerebral digital subtraction angiogram demonstrates direct traumatic carotid-cavernous fistula (CCF). (B) The plain skull lateral view showed the BeGraft stent (between black arrows). (C) The lateral view of the digital subtraction angiography angiogram showed endoleak after stent deployment. (D) The plain skull lateral view showed balloon inflation (arrow) in the BeGraft stent. (E) Final images of the endovascular procedure showed complete resolution of the CCF with preservation of the internal carotid artery. (F) The follow-up computed tomography angiogram showed stent without in-stent stenosis.
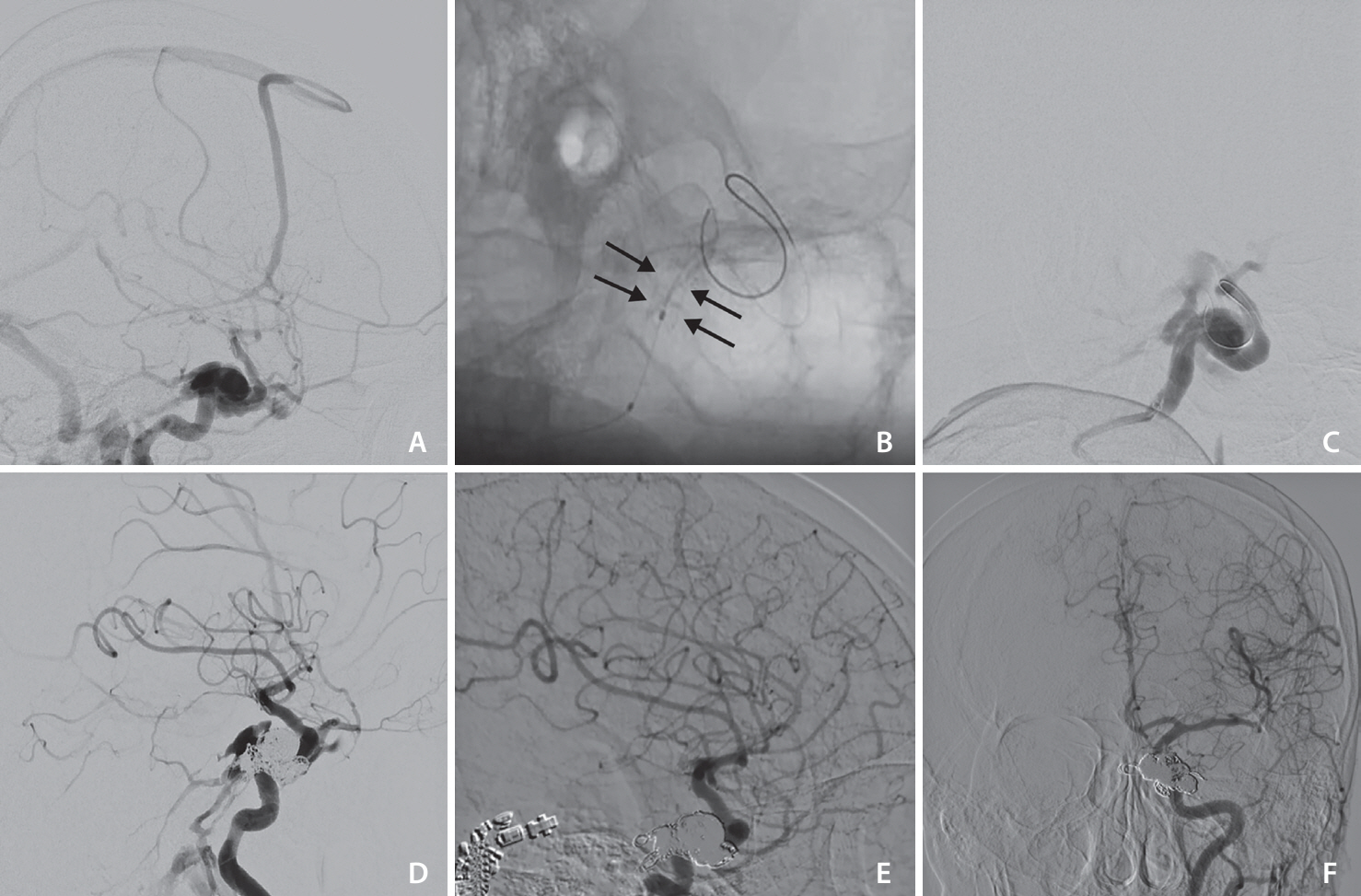
Fig. 2. Patient 3. (A) The cerebral digital subtraction angiography (DSA), lateral view demonstrates traumatic direct carotid-cavernous fistula with cortical venous reflux, the internal carotid artery (ICA) size before fistula was about 5 mm. (B) The plain lateral view showed BeGraft stent 5–18 (between arrows), deployed in the cavernous-petrous part of the ICA. (C) Lateral DSA showed endoleak after stent deployment and re-dilatation with balloon, (D) lateral DSA view showed persistent leak into the cavernous sinus despite BeGraft deployment and adding 13 coils in the cavernous sinus pouch, and (E, F) follow-up DSA lateral and anterior posterior view showed complete resolution of endoleak.
Reference
-
1. Serbinenko FA. Balloon catheterization and occlusion of major cerebral vessels. J Neurosurg. 1974; 41:125–145.
Article2. Ide S, Kiyosue H, Tokuyama K, Hori Y, Sagara Y, Kubo T. Direct carotid cavernous fistulas. J Neuroendovasc Ther. 2020; 14:583–592.
Article3. Texakalidis P, Tzoumas A, Xenos D, Rivet DJ, Reavey-Cantwell J. Carotid cavernous fistula (CCF) treatment approaches: a systematic literature review and meta-analysis of transarterial and transvenous embolization for direct and indirect CCFs. Clin Neurol Neurosurg. 2021; 204:106601.
Article4. Farhatnia Y, Tan A, Motiwala A, Cousins BG, Seifalian AM. Evolution of covered stents in the contemporary era: clinical application, materials and manufacturing strategies using nanotechnology. Biotechnol Adv. 2013; 31:524–542.
Article5. Lu D, Ma T, Zhu G, Zhang T, Wang N, Lei H, et al. Willis covered stent for treating intracranial pseudoaneurysms of the internal carotid artery: a multi-institutional study. Neuropsychiatr Dis Treat. 2022; 18:125–135.
Article6. Yin B, Sheng HS, Wei RL, Lin J, Zhou H, Zhang N. Comparison of covered stents with detachable balloons for treatment of posttraumatic carotid-cavernous fistulas. J Clin Neurosci. 2013; 20:367–372.
Article7. Liu Q, Qi C, Wang Y, Su W, Li G, Wang D. Treatment of direct carotid-cavernous fistula with Willis covered stent with midterm follow-up. Chin Neurosurg J. 2021; 7:41.
Article8. Li J, Lan ZG, Xie XD, You C, He M. Traumatic carotid-cavernous fistulas treated with covered stents: experience of 12 cases. World Neurosurg. 2010; 73:514–519.
Article9. Archondakis E, Pero G, Valvassori L, Boccardi E, Scialfa G. Angiographic follow-up of traumatic carotid cavernous fistulas treated with endovascular stent graft placement. AJNR Am J Neuroradiol. 2007; 28:342–347.10. Gomez F, Escobar W, Gomez AM, Gomez JF, Anaya CA. Treatment of carotid cavernous fistulas using covered stents: midterm results in seven patients. AJNR Am J Neuroradiol. 2007; 28:1762–1768.
Article11. Li K, Cho YD, Kim KM, Kang HS, Kim JE, Han MH. Covered stents for the endovascular treatment of a direct carotid cavernous fistula: single center experiences with 10 cases. J Korean Neurosurg Soc. 2015; 57:12–18.
Article12. Wang W, Li MH, Li YD, Gu BX, Lu HT. Reconstruction of the internal carotid artery after treatment of complex traumatic direct carotid-cavernous fistulas with the willis covered stent: a retrospective study with long-term follow-up. Neurosurgery. 2016; 79:794–805.
Article13. Wang C, Xie X, You C, Zhang C, Cheng M, He M, et al. Placement of covered stents for the treatment of direct carotid cavernous fistulas. AJNR Am J Neuroradiol. 2009; 30:1342–1346.
Article14. Wang W, Li YD, Li MH, Tan HQ, Gu BX, Wang J, et al. Endovascular treatment of post-traumatic direct carotid-cavernous fistulas: a single-center experience. J Clin Neurosci. 2011; 18:24–28.
Article15. He XH, Li WT, Peng WJ, Lu JP, Liu Q, Zhao R. Endovascular treatment of posttraumatic carotid-cavernous fistulas and pseudoaneurysms with covered stents. J Neuroimaging. 2014; 24:287–291.
Article16. Petrov I, Stankov Z, Boychev D, Klissurski M. Use of coronary stent grafts for the treatment of high-flow carotid cavernous fistula. BMJ Case Rep. 2021; 14:e245922.
Article17. Jeong SH, Lee JH, Choi HJ, Kim BC, Yu SH, Lee JI. First line treatment of traumatic carotid cavernous fistulas using covered stents at level 1 regional trauma center. J Korean Neurosurg Soc. 2021; 64:818–826.
Article18. Wroe WW, Zeineddine HA, Dawes BH, Martinez-Gutierrez JC, Shah M, Spiegel G, et al. Treatment of traumatic direct carotid cavernous fistula with a PK papyrus covered stent: a report of 2 cases. Stroke Vasc Interv Neurol. 2023; 3:e001015.
Article19. Kilic ID, Fabris E, Serdoz R, Caiazzo G, Foin N, Abou-Sherif S, et al. Coronary covered stents. EuroIntervention. 2016; 12:1288–1295.
Article20. Kufner S, Schacher N, Ferenc M, Schlundt C, Hoppmann P, Abdel-Wahab M, et al. Outcome after new generation single-layer polytetrafluoroethylene-covered stent implantation for the treatment of coronary artery perforation. Catheter Cardiovasc Interv. 2019; 93:912–920.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Regional Cerebral Blood Flow Changes in Traumatic Carotid Cavernous Fistula During Trapping Procedure: Case Study, Preliminary Report
- Traumatic Carotid-cavernous Fistula Bringing about Intracerebral Hemorrhage
- Direct Microsurgical Repair of Traumatic Carotid-Cavernous Fistula
- Treatment of High-Flow Carotid Cavernous Fistula Using a Graft Stent: Case Report
- Bilateral Traumatic Carotid-Cavernous Fistula
