Characteristics of pantaloon inguinal hernia and evaluation of added laparoscopic iliopubic tract repair to transabdominal preperitoneal hernioplasty: a retrospective observational study
- Affiliations
-
- 1Department of Surgery, Damsoyu Hospital, Seoul, Korea
- KMID: 2556328
- DOI: http://doi.org/10.4174/astr.2024.106.6.361
Abstract
- Purpose
Pantaloon hernia (PH), defined as concurrent ipsilateral direct and indirect inguinal hernias, is known for its high postoperative recurrence rate. This study retrospectively investigated the characteristics of PHs and evaluated the safety and efficacy of incorporating laparoscopic iliopubic tract repair (IPTR) into transabdominal preperitoneal (TAPP) hernioplasty.
Methods
A total of 3,355 patients who underwent TAPP hernioplasty for groin hernias between October 2014 and December 2021 were analyzed. These patients were divided into 2 groups: PH (97 patients) and non-PH (3,258 patients). The PH group was further subdivided based on the surgical technique used: TAPP hernioplasty without IPTR (TAPP group, 39 patients) and TAPP hernioplasty with IPTR for defect closure (TAPP + IPTR group, 58 patients).
Results
The study included 93 male and 4 female patients with PH. Patients with PH were generally older and predominantly male compared to the non-PH group. The recurrence rate in the PH group was notably higher than in the non-PH group (2.1% [2 of 97] vs. 0.2% [6 of 3,258], respectively; P = 0.007). Among the PH group, reoperations were more frequent in the TAPP group compared to the TAPP + IPTR group (10.3% [4 of 39] vs. 0% [0 of 58], respectively; P = 0.048). The reasons for reoperation in the PH group included recurrences (2 patients), mesh bulge (1 patient), and chronic seroma (1 patient).
Conclusion
TAPP + IPTR hernioplasty is an acceptable approach in PH treatment, reducing reoperation.
Keyword
Figure
-
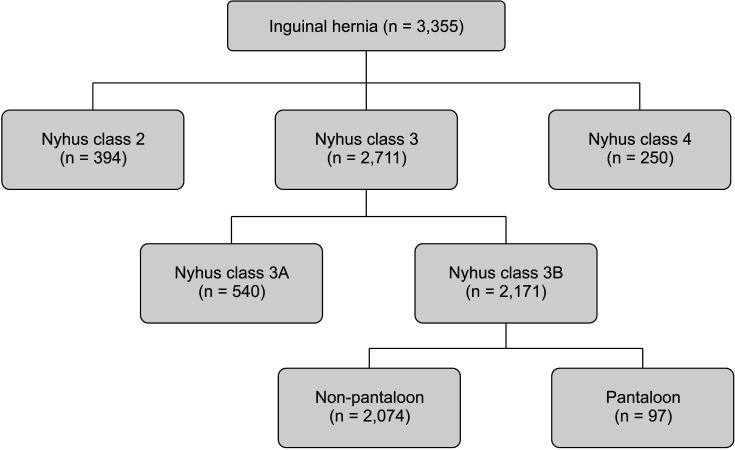
Fig. 1 Flowchart of patient enrollment. Nyhus class 2: indirect inguinal hernia with the internal ring dilated but the posterior inguinal wall intact, and the inferior epigastric vessels not displaced. Nyhus class 3A: direct inguinal hernia. Nyhus class 3B: indirect inguinal hernia with the internal inguinal ring dilated, medially encroaching on or destroying the transversalis fascia of Hesselbach’s triangle (massive scrotal, sliding, or pantaloon hernias). Nyhus class 4: recurrent hernia.
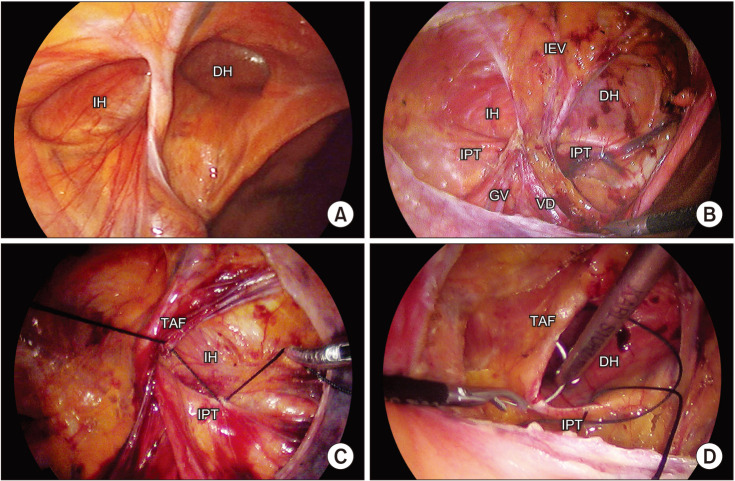
Fig. 2 Anatomy of a pantaloon inguinal hernia. (A) Laparoscopic view. (B) Preperitoneal dissection. (C) Iliopubic tract repair (IPTR) of indirect defect. (D) IPTR of direct defect. IH, indirect hernia; DH, direct hernia; IEV, inferior epigastric vessel; IPT, iliopubic tract; GV, gonadal vessel; VD, vas deferens; TAF, transversus abdominis fascia.
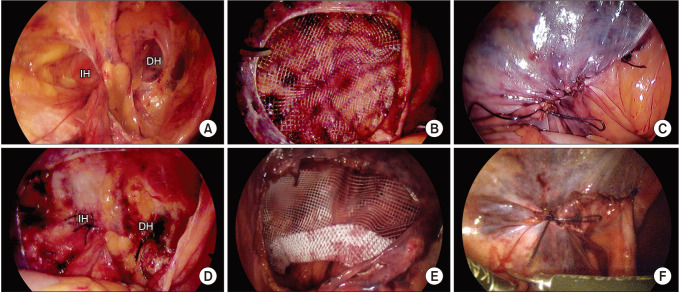
Fig. 3 Transabdominal preperitoneal (TAPP) hernioplasty vs. TAPP + iliopubic tract repair (IPTR). (A) TAPP hernioplasty. (B) Mesh implantation without defect closure. (C) Peritoneal closure. (D) TAPP + IPTR hernioplasty. (E) Mesh implantation with defect closure by IPTR. (F) Peritoneal closure. IH, indirect hernia; DH, direct hernia.
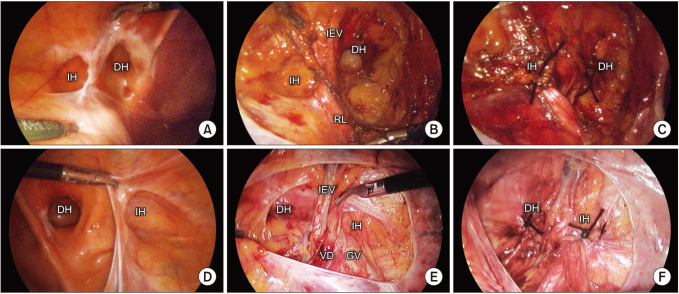
Fig. 4 Transabdominal preperitoneal (TAPP) + iliopubic tract repair (IPTR) hernioplasty of male and female patients. (A) Pantaloon hernia (PH) in a female patient. (B) Anatomy after preperitoneal dissection. (C) IPTR of both hernia defects. (D) PH in a male patient. (E) Peritoneal closure. (F) Anatomy after preperitoneal dissection. IPTR of both hernia defects. IH, indirect hernia; DH, direct hernia; IEV, inferior epigastric vessel; RL, round ligament; VD, vas deferens; GV, gonadal vessel.
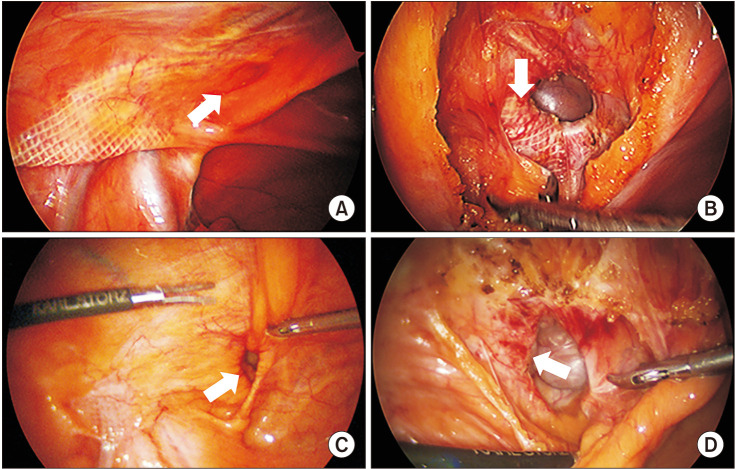
Fig. 5 Recurrence after transabdominal preperitoneal (TAPP) on pantaloon hernia. (A) Direct hernia following TAPP. The indirect area was well covered with mesh, but a direct hernia (arrow) occurred 1 year after surgery. (B) The previously used mesh (arrow) has migrated to the direct defect. (C) Direct hernia following TAPP. The indirect area was well covered with mesh, but a direct hernia (arrow) occurred 6 months after surgery. (D) The previously used mesh (arrow) is attached to the margin of the direct defect.
Reference
-
1. Zollinger RM Jr. An updated traditional classification of inguinal hernias. Hernia. 2004; 8:318–322. PMID: 15221644.2. Erdman S. Inguinal hernia in the male: with regard to post-operative sequelae. Ann Surg. 1917; 66:702–710. PMID: 17863830.3. Kapiris S, Mavromatis T, Andrikopoulos S, Georgiades C, Floros D, Diamantopoulos G. Laparoscopic transabdominal preperitoneal hernia repair (TAPP): stapling the mesh is not mandatory. J Laparoendosc Adv Surg Tech A. 2009; 19:419–422. PMID: 19397396.4. Feng B, He ZR, Li JW, Ling TL, Zhang Y, Chen X, et al. Feasibility of incremental laparoscopic inguinal hernia repair development in China: an 11-year experience. J Am Coll Surg. 2013; 216:258–265. PMID: 23317574.5. Nyhus LM. Individualization of hernia repair: a new era. Surgery. 1993; 114:1–2. PMID: 8356511.6. Litwin DE, Pham QN, Oleniuk FH, Kluftinger AM, Rossi L. Laparoscopic groin hernia surgery: the TAPP procedure: transabdominal preperitoneal hernia repair. Can J Surg. 1997; 40:192–198. PMID: 9194780.7. Thomson A. Cause anatomique de la hernie inguinale externe. J Conn Med Part. 1836; 4:147.8. Teoh LS, Hingston G, Al-Ali S, Dawson B, Windsor JA. The iliopubic tract: an important anatomical landmark in surgery. J Anat. 1999; 194(Pt 1):137–141. PMID: 10227675.9. Nyhus LM. Iliopubic tract repair of inguinal and femoral hernia: the posterior (preperitoneal) approach. Surg Clin North Am. 1993; 73:487–499. PMID: 8497798.10. Scheuermann U, Niebisch S, Lyros O, Jansen-Winkeln B, Gockel I. Transabdominal Preperitoneal (TAPP) versus Lichtenstein operation for primary inguinal hernia repair: a systematic review and meta-analysis of randomized controlled trials. BMC Surg. 2017; 17:55. PMID: 28490321.11. Cheong KX, Lo HY, Neo JX, Appasamy V, Chiu MT. Inguinal hernia repair: are the results from a general hospital comparable to those from dedicated hernia centres? Singapore Med J. 2014; 55:191–197. PMID: 24763834.12. Lee SR, Park SS. The novel technique of transabdominal preperitoneal hernioplasty herniorrhaphy for direct inguinal hernia: suture repair of hernia defect wall. J Laparoendosc Adv Surg Tech A. 2018; 28:83–88. PMID: 28414571.13. Lee SR, Park PJ. Novel transabdominal preperitoneal hernioplasty technique for recurrent inguinal hernia: overlapping of whole posterior wall with newly added mesh and pre-existing mesh by closing hernia defect. J Laparoendosc Adv Surg Tech A. 2018; 28:1503–1509. PMID: 30106640.14. Lee SR. Benefits of laparoscopic posterior wall suture repair in treating adolescent indirect inguinal hernias. Hernia. 2018; 22:653–659. PMID: 29392506.15. Lee SR, Park PJ. Adding iliopubic tract repair to high ligation reduces recurrence risk in pediatric laparoscopic transabdominal inguinal hernia repair. Surg Endosc. 2021; 35:216–222. PMID: 31938927.16. Lee YJ, Kim JH, Kim CH, Lee GR, Lee YS, Kim HJ. Single incision laparoscopic totally extraperitoneal hernioplasty: lessons learned from 1,231 procedures. Ann Surg Treat Res. 2021; 100:47–53. PMID: 33457397.17. Bansal VK, Misra MC, Babu D, Victor J, Kumar S, Sagar R, et al. A prospective, randomized comparison of long-term outcomes: chronic groin pain and quality of life following totally extraperitoneal (TEP) and transabdominal preperitoneal (TAPP) laparoscopic inguinal hernia repair. Surg Endosc. 2013; 27:2373–2382. PMID: 23389072.18. Kald A, Fridsten S, Nordin P, Nilsson E. Outcome of repair of bilateral groin hernias: a prospective evaluation of 1,487 patients. Eur J Surg. 2002; 168:150–153. PMID: 12182239.19. Li W, Sun D, Sun Y, Cen Y, Li S, Xu Q, et al. The effect of transabdominal preperitoneal (TAPP) inguinal hernioplasty on chronic pain and quality of life of patients: mesh fixation versus non-fixation. Surg Endosc. 2017; 31:4238–4243. PMID: 28289971.20. Bittner R, Arregui ME, Bisgaard T, Dudai M, Ferzli GS, Fitzgibbons RJ, et al. Guidelines for laparoscopic (TAPP) and endoscopic (TEP) treatment of inguinal hernia [International Endohernia Society (IEHS)]. Surg Endosc. 2011; 25:2773–2843. PMID: 21751060.21. Wellwood J, Sculpher MJ, Stoker D, Nicholls GJ, Geddes C, Whitehead A, et al. Randomised controlled trial of laparoscopic versus open mesh repair for inguinal hernia: outcome and cost. BMJ. 1998; 317:103–110. PMID: 9657784.22. Roos MM, van Hessen CV, Verleisdonk EJ, Clevers GJ, Davids PH, Voorbrood CE, et al. An 11-year analysis of reoperated groins after endoscopic totally extraperitoneal (TEP) inguinal hernia repair in a high volume hernia center. Hernia. 2019; 23:655–662. PMID: 30244345.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Early outcomes of robotic transabdominal preperitoneal inguinal hernia repair: a retrospective single-institution study in Korea
- Initial experience of single port laparoscopic totally extraperitoneal hernia repair: nearly-scarless inguinal hernia repair
- Single incision laparoscopic totally extraperitoneal hernioplasty: lessons learned from 1,231 procedures
- Laparoscopic repair of inguinal hernias: Risk factors for urinary retention and chronic pain after totally extraperitoneal repair and transabdominal preperitoneal repair
- Left Side Approach in Laparoscopic Transabdominal Preperitoneal Inguinal Herniorrhaphy is Feasible for Any Type of Inguinal Hernia
