Anesth Pain Med.
2024 Apr;19(2):134-143. 10.17085/apm.23161.
Preoperative echocardiography as a predictor of spinal anesthesia-induced hypotension in older patients with mild left ventricular diastolic dysfunction: a retrospective observational study
- Affiliations
-
- 1Department of Anesthesia and Pain Medicine, Medical Research Institute, Pusan National University Hospital, Busan, Korea
- 2Department of Anesthesia and Pain Medicine, School of Medicine, Pusan National University, Yangsan, Korea
- 3Department of Anesthesia and Pain Medicine, School of Dentistry, Kyungpook National University, Daegu, Korea
- 4Department of Anesthesiology and Pain Medicine, Seoul National University Hospital, Seoul, Korea
- KMID: 2555250
- DOI: http://doi.org/10.17085/apm.23161
Abstract
- Background
Spinal anesthesia-induced hypotension (SAH) frequently occurs in older patients, many of whom have mild left ventricular (LV) diastolic dysfunction, often asymptomatic at rest. This study investigated the association between preoperative echocardiographic measurements and SAH in older patients with mild LV diastolic dysfunction.
Methods
We conducted a retrospective observational study using data from electronic medical records. The patients ≥ 65 years old who underwent spinal anesthesia for urologic surgery between January 2016 and December 2017 and whose preoperative echocardiography within 6 months before surgery revealed grade I LV diastolic dysfunction were recruited. SAH was investigated using the anesthesia records. Logistic regression and receiver operating characteristic (ROC) curve analyses were performed.
Results
A total of 163 patients were analyzed. SAH and significant SAH developed in 55 (33.7%) patients. The mitral inflow E velocity was an independent risk factor for SAH (odds ratio [OR], 0.886; 95% confidence interval [CI], 0.845–0.929; P < 0.001). The area under the ROC curve for mitral inflow E velocity to predict SAH was 0.819 (95% CI, 0.752–0.875; P < 0.001). If mitral inflow E velocity was ≤ 60 cm/s, SAH was predicted with a sensitivity of 83.6% and specificity of 70.4%.
Conclusions
The preoperative mitral inflow E velocity demonstrated the greatest predictability of SAH in older patients with mild LV diastolic dysfunction. This may assist in identifying patients at high risk of SAH and guiding preventive strategies in the future.
Keyword
Figure
-
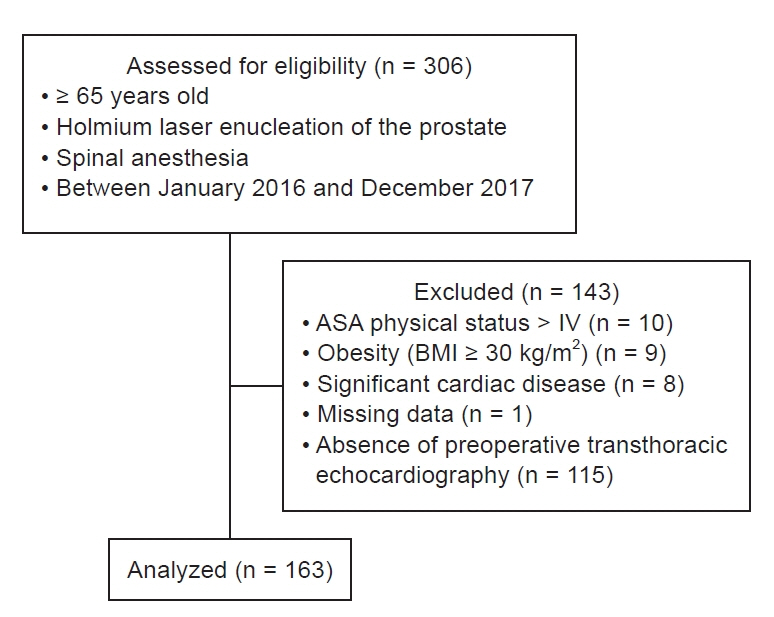
Fig. 1. Flow diagram. ASA: American Society of Anesthesiologists, BMI: body mass index.
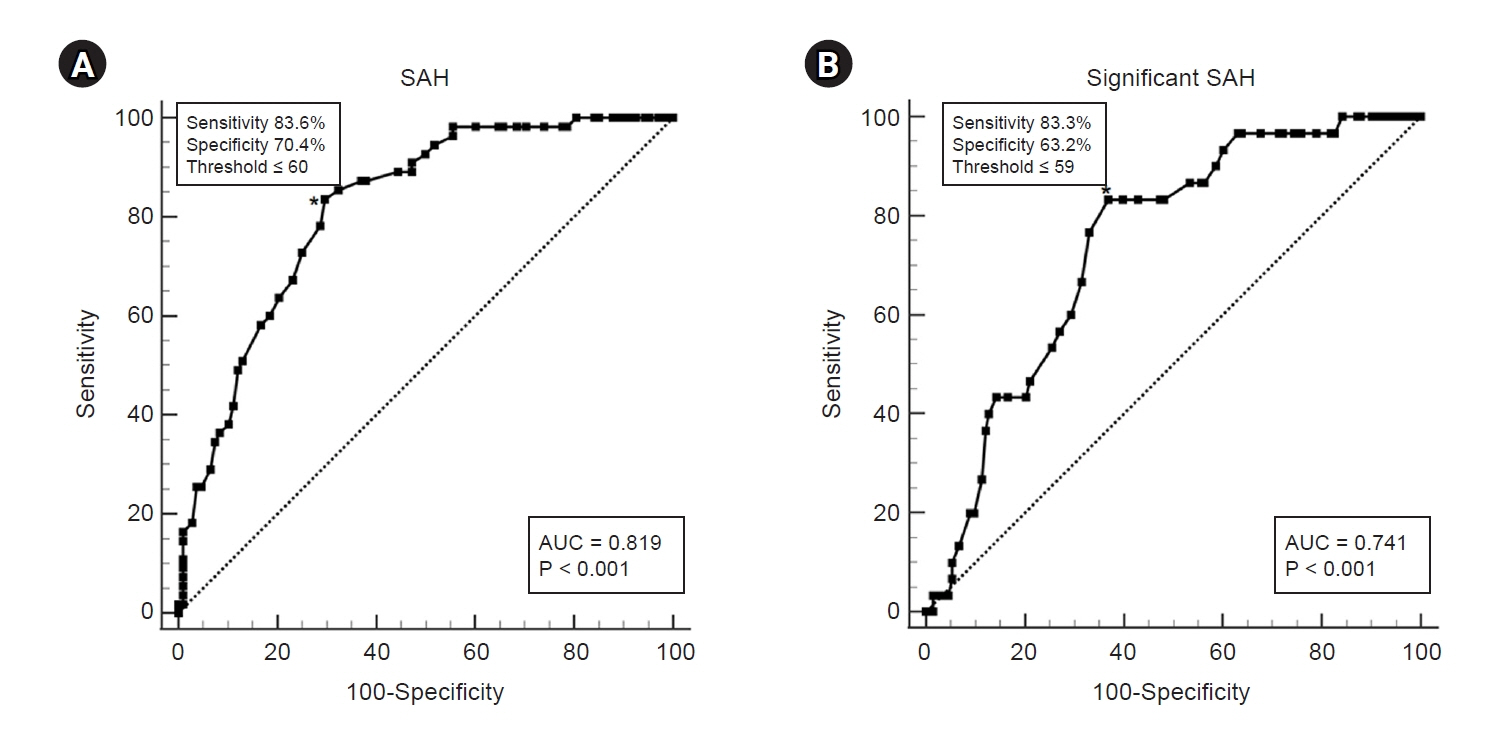
Fig. 2. ROC curve analysis on mitral inflow M velocity for SAH (A) and significant SAH (B). AUC: area under the curve, SAH: spinal anesthesia-induced hypotension; ROC: receiver operating characteristic. *Represents cutoff value.
Reference
-
1. Mascha EJ, Yang D, Weiss S, Sessler DI. Intraoperative mean arterial pressure variability and 30-day mortality in patients having noncardiac surgery. Anesthesiology. 2015; 123:79–91.
Article2. Wesselink EM, Kappen TH, Torn HM, Slooter AJC, Van Klei WA. Intraoperative hypotension and the risk of postoperative adverse outcomes: a systematic review. Br J Anaesth. 2018; 121:706–21.
Article3. Hartmann B, Junger A, Klasen J, Benson M, Jost A, Banzhaf A, et al. The incidence and risk factors for hypotension after spinal anesthesia induction: an analysis with automated data collection. Anesth Analg. 2002; 94:1521–9. table of contents.
Article4. Lairez O, Ferré F, Portet N, Marty P, Delmas C, Cognet T, et al. Cardiovascular effects of low-dose spinal anaesthesia as a function of age: An observational study using echocardiography. Anaesth Crit Care Pain Med. 2015; 34:271–6.
Article5. Carpenter RL, Caplan RA, Brown DL, Stephenson C, Wu R. Incidence and risk factors for side effects of spinal anesthesia. Anesthesiology. 1992; 76:906–16.
Article6. Salama ER, Elkashlan M. Pre-operative ultrasonographic evaluation of inferior vena cava collapsibility index and caval aorta index as new predictors for hypotension after induction of spinal anaesthesia: a prospective observational study. Eur J Anaesthesiol. 2019; 36:297–302.
Article7. Moschovaki N, Saranteas T, Spiliotaki E, Giannoulis D, Anagnostopoulos D, Talliou C, et al. Point of care transthoracic echocardiography for the prediction of post - spinal anesthesia hypotension in elderly patients with cardiac diseases and left ventricular dysfunction : Inferior vena cava and post-spinal anesthesia hypotension in elderly patients. J Clin Monit Comput. 2023; 37:1207–18.
Article8. Jakobsson J, Kalman SH, Lindeberg-Lindvet M, Bartha E. Is postspinal hypotension a sign of impaired cardiac performance in the elderly? an observational mechanistic study. Br J Anaesth. 2017; 119:1178–85.
Article9. Dai X, Hummel SL, Salazar JB, Taffet GE, Zieman S, Schwartz JB. Cardiovascular physiology in the older adults. J Geriatr Cardiol. 2015; 12:196–201.10. Redfield MM, Jacobsen SJ, Burnett JCJ, Mahoney DW, Bailey KR, Rodeheffer RJ. Burden of systolic and diastolic ventricular dysfunction in the community: appreciating the scope of the heart failure epidemic. JAMA. 2003; 289:194–202.
Article11. Rosamond W, Flegal K, Friday G, Furie K, Go A, Greenlund K, et al. Heart disease and stroke statistics--2007 update: a report from the American Heart Association Statistics Committee and Stroke Statistics Subcommittee. Circulation. 2007; 115:e69–171.12. Nicoara A, Swaminathan M. Diastolic dysfunction, diagnostic and perioperative management in cardiac surgery. Curr Opin Anaesthesiol. 2015; 28:60–6.
Article13. Bijker JB, Van Klei WA, Kappen TH, Van Wolfswinkel L, Moons KGM, Kalkman CJ. Incidence of intraoperative hypotension as a function of the chosen definition: Literature definitions applied to a retrospective cohort using automated data collection. Anesthesiology. 2007; 107:213–20.14. Nagueh SF, Smiseth OA, Appleton CP, Byrd BF, Dokainish H, Edvardsen T, et al. Recommendations for the evaluation of left ventricular diastolic function by echocardiography: an update from the American Society of Echocardiography and the European association of cardiovascular imaging. J Am Soc Echocardiogr. 2016; 29:277–314.15. Smiseth OA. Evaluation of left ventricular diastolic function: state of the art after 35 years with doppler assessment. J Echocardiogr. 2018; 16:55–64.16. Ruiz-Nodar JM, Puchades R, Jiménez-Borreguero J, Blanco F, Rodríguez F, Alonso M, et al. Echocardiographic findings in an elderly population. influence of arterial hypertension. the EPICARDIAN study. Rev Esp Cardiol. 2008; 61:881–3.17. Chowdhury SR, Datta PK, Maitra S, Rawat D, Baidya DK, Roy A, et al. The use of preoperative inferior vena cava ultrasound to predict anaesthesia-induced hypotension: a systematic review. Anaesthesiol Intensive Ther. 2023; 55:18–31.18. Chowdhury SR, Baidya DK, Maitra S, Singh AK, Rewari V, Anand RK. Assessment of role of inferior vena cava collapsibility index and variations in carotid artery peak systolic velocity in prediction of post-spinal anaesthesia hypotension in spontaneously breathing patients: an observational study. Indian J Anaesth. 2022; 66:100–6.19. Kimura BJ, Dalugdugan R, Gilcrease GW, Phan JN, Showalter BK, Wolfson T. The effect of breathing manner on inferior vena caval diameter. Eur J Echocardiogr. 2011; 12:120–3.20. Gignon L, Roger C, Bastide S, Alonso S, Zieleskiewicz L, Quintard H, et al. Influence of diaphragmatic motion on inferior vena cava diameter respiratory variations in healthy volunteers. Anesthesiology. 2016; 124:1338–46.
Article21. Ginghina C, Beladan CC, Iancu M, Calin A, Popescu BA. Respiratory maneuvers in echocardiography: a review of clinical applications. Cardiovasc Ultrasound. 2009; 7:42.
Article22. Appleton CP, Hatle LK, Popp RL. Relation of transmitral flow velocity patterns to left ventricular diastolic function: new insights from a combined hemodynamic and Doppler echocardiographic study. J Am Coll Cardiol. 1988; 12:426–40.
Article23. Enriquez-Sarano M, Bailey KR, Seward JB, Tajik AJ, Krohn MJ, Mays JM. Quantitative doppler assessment of valvular regurgitation. Circulation. 1993; 87:841–8.
Article24. Lewis JF, Kuo LC, Nelson JG, Limacher MC, Quinones MA. Pulsed doppler echocardiographic determination of stroke volume and cardiac output: clinical validation of two new methods using the apical window. Circulation. 1984; 70:425–31.
Article25. Barberato SH, Pecoits-Filho R. Usefulness of left atrial volume for the differentiation of normal from pseudonormal diastolic function pattern in patients on hemodialysis. J Am Soc Echocardiogr. 2007; 20:359–65.
Article26. Hofhuizen C, Lemson J, Snoeck M, Scheffer GJ. Spinal anesthesia-induced hypotension is caused by a decrease in stroke volume in elderly patients. Local Reg Anesth. 2019; 12:19–26.27. Sohn DW, Chai IH, Lee DJ, Kim HC, Kim HS, Oh BH, et al. Assessment of mitral annulus velocity by doppler tissue imaging in the evaluation of left ventricular diastolic function. J Am Coll Cardiol. 1997; 30:474–80.
Article28. Daimon M, Watanabe H, Abe Y, Hirata K, Hozumi T, Ishii K, et al. Normal values of echocardiographic parameters in relation to age in a healthy japanese population: the JAMP study. Circ J. 2008; 72:1859–66.
Article29. Kim H, Kim WH, Lim HW, Kim JA, Kim D, Shin BS, et al. Obesity is independently associated with spinal anesthesia outcomes: a prospective observational study. PLoS One. 2015; 10:e0124264.
Article30. Sullivan JT, Grouper S, Walker MT, Parrish TB, McCarthy RJ, Wong CA. Lumbosacral cerebrospinal fluid volume in humans using three-dimensional magnetic resonance imaging. Anesth Analg. 2006; 103:1306–10.
Article31. Hogan QH, Prost R, Kulier A, Taylor ML, Liu S, Mark L. Magnetic resonance imaging of cerebrospinal fluid volume and the influence of body habitus and abdominal pressure. Anesthesiology. 1996; 84:1341–9.
Article32. Asehnoune K, Larousse E, Tadié JM, Minville V, Droupy S, Benhamou D. Small-dose bupivacaine-sufentanil prevents cardiac output modifications after spinal anesthesia. Anesth Analg. 2005; 101:1512–5.
Article33. Labbene I, Lamine K, Gharsallah H, Jebali A, Adhoum A, Ghozzi S, et al. Spinal anesthesia for endoscopic urological surgery--low dose vs. varying doses of hyperbaric bupivacaine. Middle East J Anaesthesiol. 2007; 19:369–84.34. Minville V, Fourcade O, Grousset D, Chassery C, Nguyen L, Asehnoune K, et al. Spinal anesthesia using single injection small-dose bupivacaine versus continuous catheter injection techniques for surgical repair of hip fracture in elderly patients. Anesth Analg. 2006; 102:1559–63.
Article35. Olofsson C, Nygårds EB, Bjersten AB, Hessling A. Low-dose bupivacaine with sufentanil prevents hypotension after spinal anesthesia for hip repair in elderly patients. Acta Anaesthesiol Scand. 2004; 48:1240–4.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Study for the Left Ventricular Diastolic Function in Mild to Moderate Hypertensive Patients without Left Ventricular Hypertrophy
- Left Ventricular Diastolic Functions by M-Mode Echocardiogram in Essential Hypertensive Patients
- Evaluation of Diastolic Dysfunction and the Role Thereof in Heart Failure with Preserved Ejection Fraction
- Perioperative management of left ventricular diastolic dysfunction and heart failure: an anesthesiologist's perspective
- Left Ventricular Diastolic Dysfunction: The What, When, and How
