Acute Crit Care.
2024 Feb;39(1):117-126. 10.4266/acc.2023.00913.
Diagnostic accuracy of left ventricular outflow tract velocity time integral versus inferior vena cava collapsibility index in predicting post-induction hypotension during general anesthesia: an observational study
- Affiliations
-
- 1Department of Anaesthesia, Indira Gandhi Medical College Shimla, India
- KMID: 2555230
- DOI: http://doi.org/10.4266/acc.2023.00913
Abstract
- Background
Point of care ultrasound (POCUS) is being explored for dynamic measurements like inferior vena cava collapsibility index (IVC-CI) and left ventricular outflow tract velocity time integral (LVOT-VTI) to guide anesthesiologists in predicting fluid responsiveness in the preoperative period and in treating post-induction hypotension (PIH) with varying accuracy. Methods: In this prospective, observational study on included 100 adult patients undergoing elective surgery under general anesthesia, the LVOT-VTI and IVC-CI measurements were performed in the preoperative room 15 minutes prior to surgery, and PIH was measured for 20 minutes in the post-induction period. Results: The incidence of PIH was 24%. The area under the curve, sensitivity, specificity, positive predictive value, negative predictive value, and diagnostic accuracy of the two techniques at 95% confidence interval was 0.613, 30.4%, 93.3%, 58.3%, 81.4%, 73.6% for IVC-CI and 0.853, 83.3%, 80.3%, 57.1%, 93.8%, 77.4% for LVOT-VTI, respectively. In multivariate analysis, the cutoff value for IVC-CI was >51.5 and for LVOT-VTI it was ≤17.45 for predicting PIH with odd ratio [OR] of 8.491 (P=0.025) for IVCCI and OR of 17.427 (P<0.001) for LVOT. LVOT-VTI assessment was possible in all the patients, while 10% of patients were having poor window for IVC measurements. Conclusions: We recommend the use of POCUS using LVOT-VTI or IVC-CI to predict PIH, to decrease the morbidity of patients undergoing surgery. Out of these, we recommend LVOT-VTI measurements as it has showed a better diagnostic accuracy (77.4%) with no failure rate.
Keyword
Figure
-
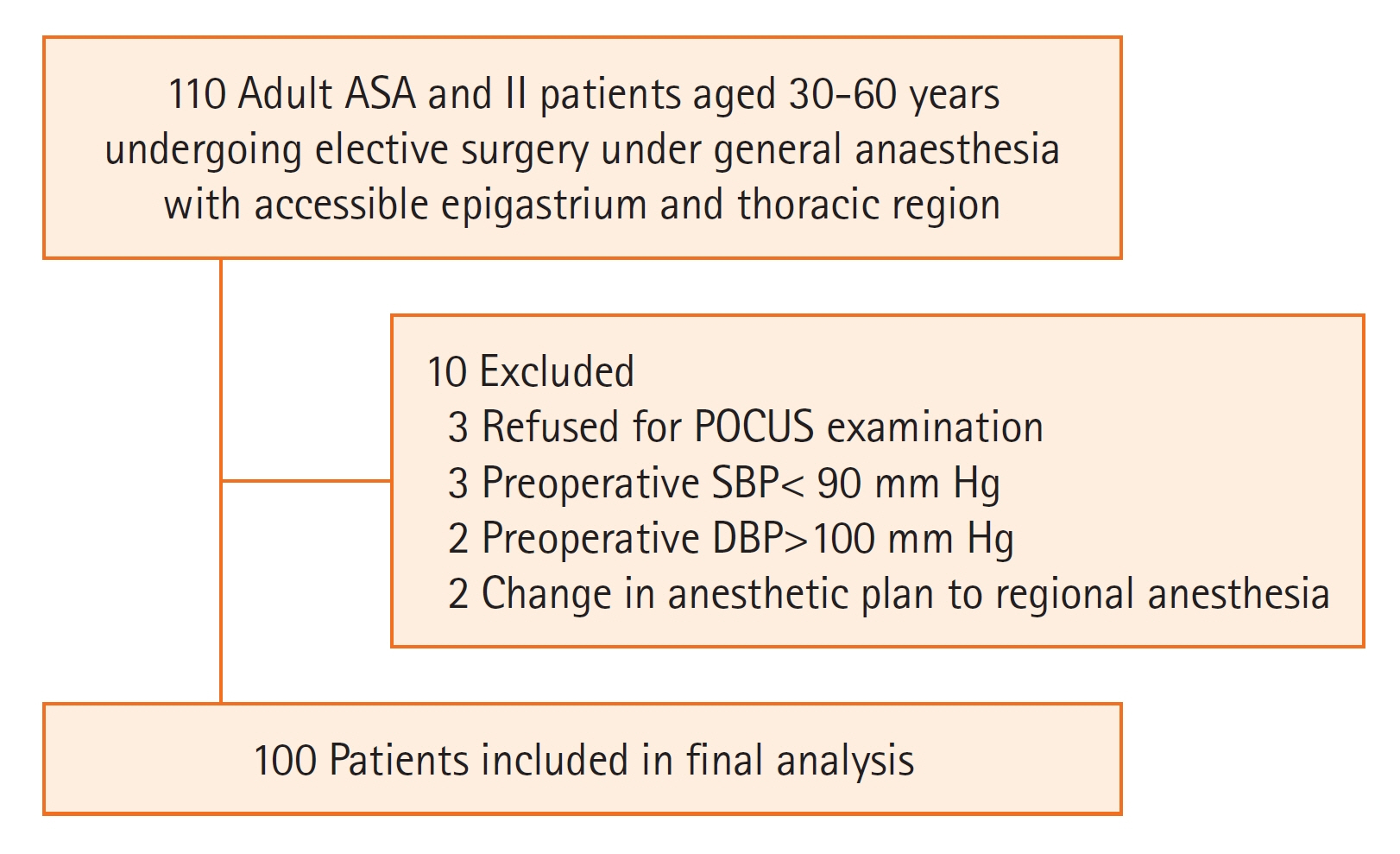
Figure 1. Flow diagram for the patient selection ASA: American Society of Anesthesiologists; POCUS: point of care ultrasound; SBP: systolic blood pressure; DBP: diastolic blood pressure.
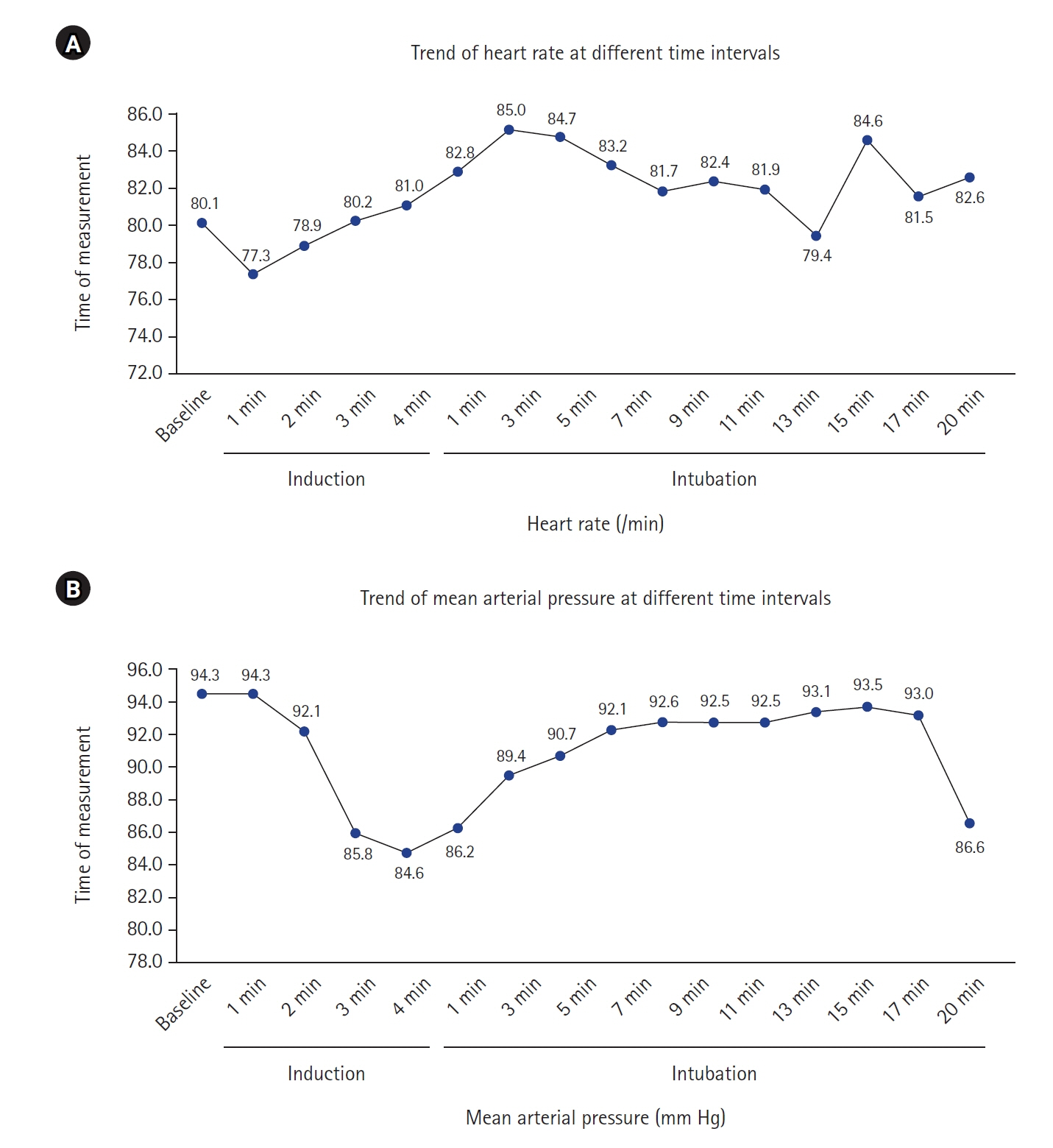
Figure 2. Descriptive statistics of heart rate (A) and mean arterial pressure (B) of study subject.
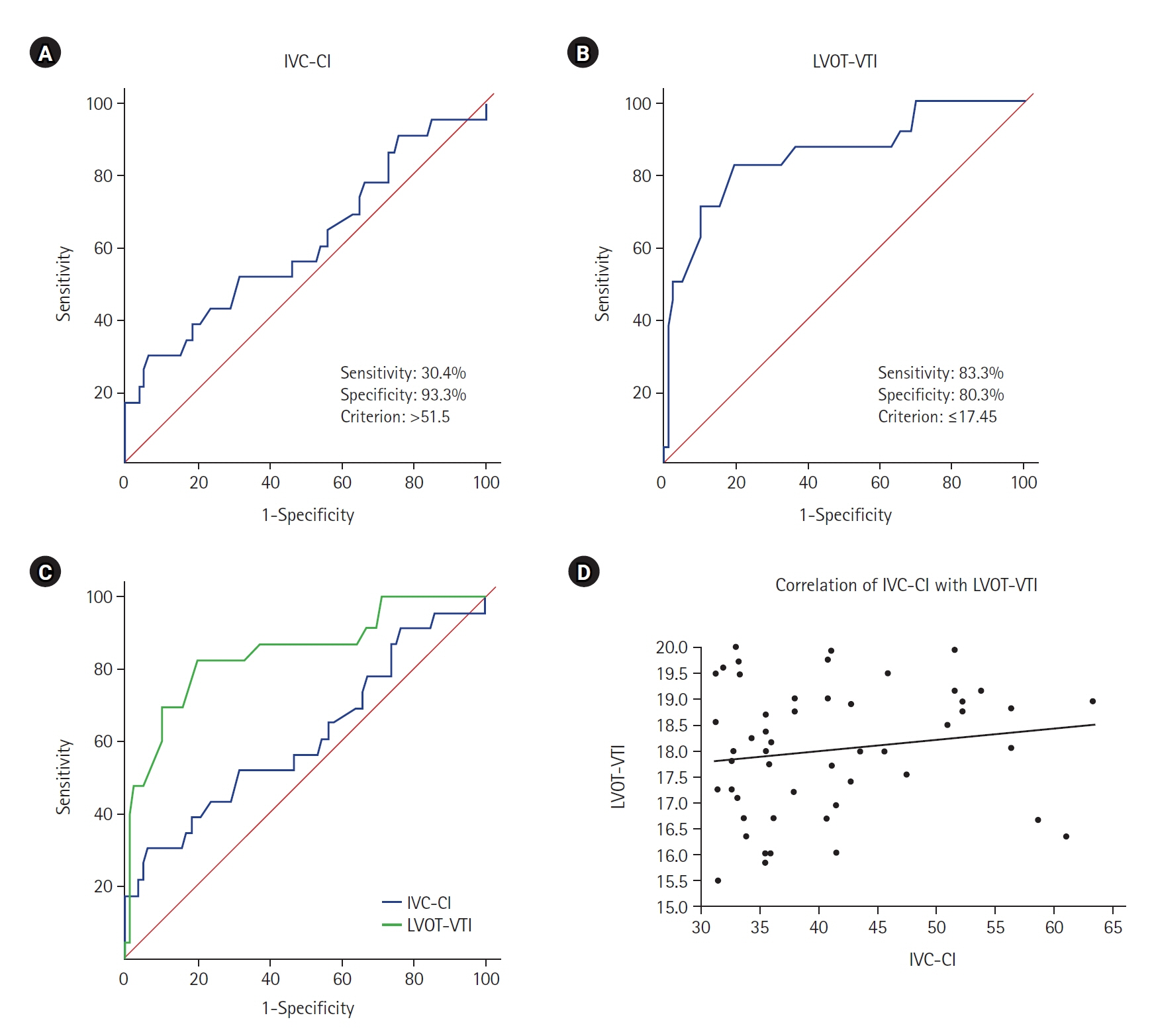
Figure 3. (A) Receiver operating characteristics (ROC) of inferior vena cava collapsibility index (IVC-CI). (B) ROC of left ventricular outflow tract velocity time integral (LVOT-VTI). (C) Comparison of area under the curve (AUC) of IVC-CI and LVOT-VTI. (D) Correlation between IVC-CI and LVOT-VTI. Spearman rank correlation coefficient.
Reference
-
1. Kalagara H, Coker B, Gerstein NS, Kukreja P, Deriy L, Pierce A, et al. Point-of-care ultrasound (POCUS) for the cardiothoracic anesthesiologist. J Cardiothorac Vasc Anesth. 2022; 36:1132–47.
Article2. Spencer KT, Kimura BJ, Korcarz CE, Pellikka PA, Rahko PS, Siegel RJ. Focused cardiac ultrasound: recommendations from the American Society of Echocardiography. J Am Soc Echocardiogr. 2013; 26:567–81.
Article3. Südfeld S, Brechnitz S, Wagner JY, Reese PC, Pinnschmidt HO, Reuter DA, et al. Post-induction hypotension and early intraoperative hypotension associated with general anaesthesia. Br J Anaesth. 2017; 119:57–64.
Article4. Jor O, Maca J, Koutna J, Gemrotova M, Vymazal T, Litschmannova M, et al. Hypotension after induction of general anesthesia: occurrence, risk factors, and therapy: a prospective multicentre observational study. J Anesth. 2018; 32:673–80.
Article5. Blanco P. Rationale for using the velocity-time integral and the minute distance for assessing the stroke volume and cardiac output in point-of-care settings. Ultrasound J. 2020; 12:21.
Article6. Desai N, Garry D. Assessing dynamic fluid-responsiveness using transthoracic echocardiography in intensive care. BJA Educ. 2018; 18:218–26.
Article7. Benes J, Kirov M, Kuzkov V, Lainscak M, Molnar Z, Voga G, et al. Fluid therapy: double-edged sword during critical care? Biomed Res Int. 2015; 2015:729075.
Article8. Reich DL, Hossain S, Krol M, Baez B, Patel P, Bernstein A, et al. Predictors of hypotension after induction of general anesthesia. Anesth Analg. 2005; 101:622–8.
Article9. Aissaoui Y, Jozwiak M, Bahi M, Belhadj A, Alaoui H, Qamous Y, et al. Prediction of post-induction hypotension by point-of-care echocardiography: a prospective observational study. Anaesth Crit Care Pain Med. 2022; 41:101090.
Article10. Wang J, Zhou D, Gao Y, Wu Z, Wang X, Lv C. Effect of VTILVOT variation rate on the assessment of fluid responsiveness in septic shock patients. Medicine (Baltimore). 2020; 99:e22702.
Article11. Szabó M, Bozó A, Darvas K, Horváth A, Iványi ZD. Role of inferior vena cava collapsibility index in the prediction of hypotension associated with general anesthesia: an observational study. BMC Anesthesiol. 2019; 19:139.
Article12. Zhang J, Critchley LA. Inferior vena cava ultrasonography before general anesthesia can predict hypotension after induction. Anesthesiology. 2016; 124:580–9.
Article13. Airapetian N, Maizel J, Alyamani O, Mahjoub Y, Lorne E, Levrard M, et al. Does inferior vena cava respiratory variability predict fluid responsiveness in spontaneously breathing patients? Crit Care. 2015; 19:400.
Article14. Singh Y, Anand RK, Gupta S, Chowdhury SR, Maitra S, Baidya DK, et al. Role of IVC collapsibility index to predict post spinal hypotension in pregnant women undergoing caesarean section: an observational trial. Saudi J Anaesth. 2019; 13:312–7.
Article15. Salama ER, Elkashlan M. Pre-operative ultrasonographic evaluation of inferior vena cava collapsibility index and caval aorta index as new predictors for hypotension after induction of spinal anaesthesia: a prospective observational study. Eur J Anaesthesiol. 2019; 36:297–302.
Article16. Dinh VA, Ko HS, Rao R, Bansal RC, Smith DD, Kim TE, et al. Measuring cardiac index with a focused cardiac ultrasound examination in the ED. Am J Emerg Med. 2012; 30:1845–51.
Article17. Hutchings SD, Rees PS. Trauma resuscitation using echocardiography in a deployed military intensive care unit. J Intensive Care Soc. 2013; 14:120–5.
Article18. Bergenzaun L, Gudmundsson P, Öhlin H, Düring J, Ersson A, Ihrman L, et al. Assessing left ventricular systolic function in shock: evaluation of echocardiographic parameters in intensive care. Crit Care. 2011; 15:R200.
Article19. Nega MH, Ahmed SA, Tawuye HY, Mustofa SY. Incidence and factors associated with post-induction hypotension among adult surgical patients: prospective follow-up study. Int J Surg Open. 2022; 49:100565.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A case of hemiazygos continuation of a left inferior vena cava
- Effect of Changes of Inferior Vena Cava Diameter on Left Ventricular Hypertrophy in Hemodialysis Patients
- Pseudoaneurysm of Surgically Reconstructed Right Ventricular Outflow Tract Complicated by Superior Vena Cava Syndrome
- Left Ventricular Metastasis From Renal Cell Carcinoma Causing Left Ventricular Outflow Tract Obstruction
- A Case of Persistent Left Superior Vena Cava with Interruption of Inferior Vena Cava
