Coronary Cameral Fistula With Giant Aneurysm
- Affiliations
-
- 1Division of Cardiology, Sant’Andrea Hospital, Rome, Italy
- 2Department of Clinical and Molecular Medicine, Sapienza University of Rome, Italy
- KMID: 2554146
- DOI: http://doi.org/10.4070/kcj.2023.0245
Figure
-
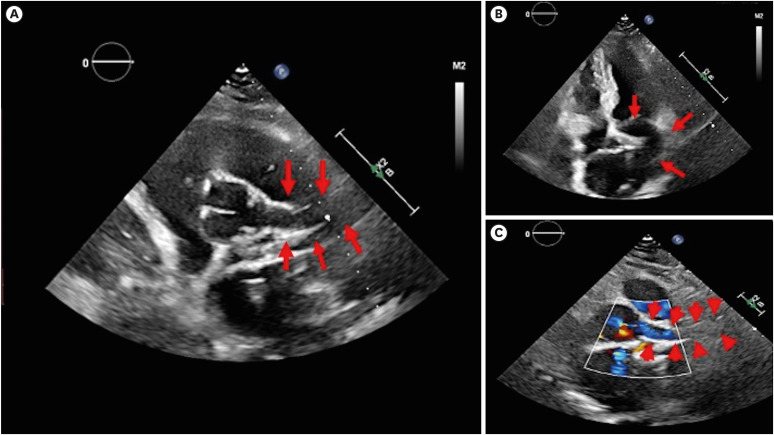
Figure 1 The transthoracic echocardiogram parasternal short axis (A) and apical 4-chamber view (B) showed an anomalous structure (red arrows) connecting from the aortic cusp. Color Doppler short-axis view (C) showed flow from the aortic cusp into an abnormal tract while the normal left coronary artery is not seen, indicating an anomalous origin of the left coronary artery.
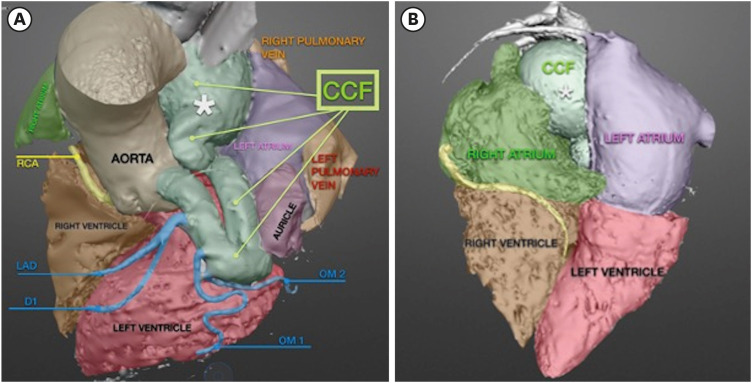
Figure 2 Electrocardiogram-gated coronary computerized tomography angiography volume-rendered images (A, frontal view) show a dilated vascular structure (green) arising from the left coronary sinus and terminating into the RA. The LAD, D1, left circumflex and its OM branch (all blue) arise from the dilated anomalous tract. The posterior view (B) of the volume-rendered image showed the aneurysmal dilatation (*) before it terminates in the RA.CCF = coronary cameral fistula; D1 = diagonal branch; LAD = left anterior descending artery; OM = obtuse marginal; RA = right atrium; RCA = right coronary artery.

Figure 3 Electrocardiogram-gated coronary computerized tomography angiography curved multi-planar reconstruction (A) clearly showed a dilated anomalous vessel (red arrows) from the LCC to the RA. LAD and OM branches emerge from the fistulous tract. Note the aneurysmal dilatation (*) near the RA. Trans-axial image (B) highlights the aneurysmal dilatation of the anomalous vessel, which is measured to have a maximum diameter of 4.27×5.32 cm.CCF = coronary cameral fistula; LAD = left anterior descending artery; LCC = left coronary cusp; OM = obtuse marginal; RA = right atrium; RV = right ventricle.
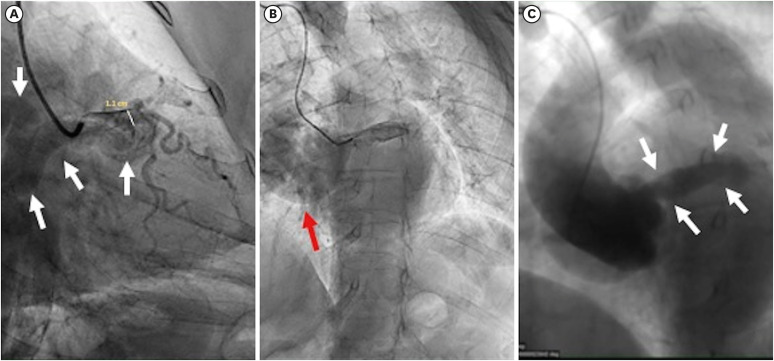
Figure 4 Invasive coronary angiography left anterior oblique projection view (A, B) showed a large anomalous vessel (white arrows in A) originating from the left coronary cusp and draining into the RA. The left main coronary artery was dilated, measuring 1.1 cm (white line in A). An aneurysmal extension (red arrow in B) of this anomalous vessel is observed before it enters the RA. Aortography (C) clearly showed the vessel's origin of the left coronary sinus (white arrows in C) and its drainage into the RA, confirming coronary-cameral fistula.RA = right atrium.
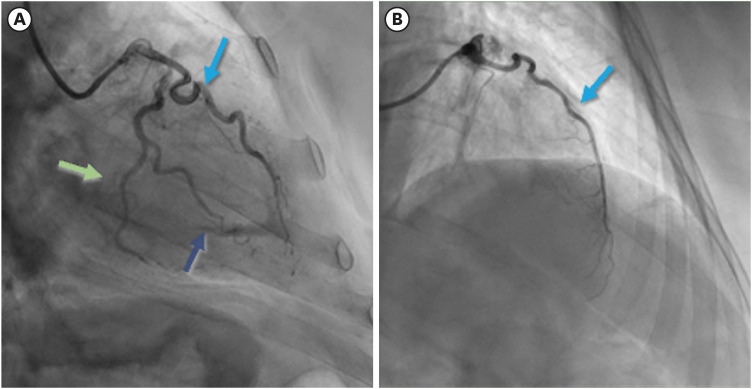
Figure 5 Selective angiography: (A) right caudal projection; (B) cranial anteroposterior projection in dilated fistulous tract showed left anterior descending artery (blue arrow), left circumflex artery (green arrow) and obtuse marginal branch (dark blue arrow). No significant atherosclerotic lesions were observed of all vessels.
Reference
-
1. Said SA, Schiphorst RH, Derksen R, Wagenaar LJ. Coronary-cameral fistulas in adults: acquired types (second of two parts). World J Cardiol. 2013; 5:484–494. PMID: 24432186.2. Mangukia CV. Coronary artery fistula. Ann Thorac Surg. 2012; 93:2084–2092. PMID: 22560322.3. Ata Y, Turk T, Bicer M, Yalcin M, Ata F, Yavuz S. Coronary arteriovenous fistulas in the adults: natural history and management strategies. J Cardiothorac Surg. 2009; 4:62. PMID: 19891792.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Right Coronary Artery to Left Ventricular Fistula with a Giant Right Coronary Artery Aneurysm: A case report
- A Case of Giant Aneurysm of Coronary Arteriovenous Fistula Treated by Percutaneous Deployment of Embolization Coil
- Coronary Artery Fistula with Giant Aneurysm and Coronary Stenosis Treated by Transcatheter Embolization and Stent
- Right Coronary Artery to Left Ventricular Fistula with Giant Right Coronary Artery Aneurysm
- Multiple Giant Coronary Aneurysms Arising from Coronary Fistula to the Pulmonary Artery Revealed in Aorta CT Angiography
