Advantages of laparoscopy in gynecologic surgery in elderly patients
- Affiliations
-
- 1Department of Obstetrics and Gynecology, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea
- 2Department of Obstetrics and Gynecology, Chung-Ang University Gwangmyeong Hospital, Chung-Ang University College of Medicine, Gwangmyeong, Korea
- KMID: 2553432
- DOI: http://doi.org/10.5468/ogs.23238
Abstract
Objective
Geriatric patients requiring gynecological surgery is increasing worldwide. However, older patients are at higher risk of postoperative morbidity and mortality, particularly cardiopulmonary complications. Laparoscopic surgery is widely used as a minimally invasive method for reducing postoperative morbidities. We compared the outcomes of open and laparoscopic gynecologic surgeries in patients older than 55 years.
Methods
We included patients aged >55 years who underwent gynecological surgery at a single tertiary center between 2010 and 2020, excluding vaginal or ovarian cancer surgeries were excluded. Surgical outcomes were compared between the open surgery and laparoscopic groups, with age cutoff was set at 65 years for optimal discriminative power. We performed linear or logistic regression analyses to compare the surgical outcomes according to age and operation type.
Results
Among 2,983 patients, 28.6% underwent open surgery and 71.4% underwent laparoscopic surgery. Perioperative outcomes of laparoscopic surgery were better than those of open surgery in all groups. In both the open and laparoscopic surgery groups, the older patients showed worse overall surgical outcomes. However, age-related differences in perioperative outcomes were less severe in the laparoscopic group. In the linear regression analysis, the differences in estimated blood loss, transfusion, and hospital stay between the age groups were smaller in the laparoscopy group. Similar results were observed in cancer-only and benign-only cohorts.
Conclusion
Although the surgical outcomes were worse in the older patients, the difference between age groups was smaller for laparoscopic surgery. Laparoscopic surgery offers more advantages and safety in patients aged >65 years.
Figure
-
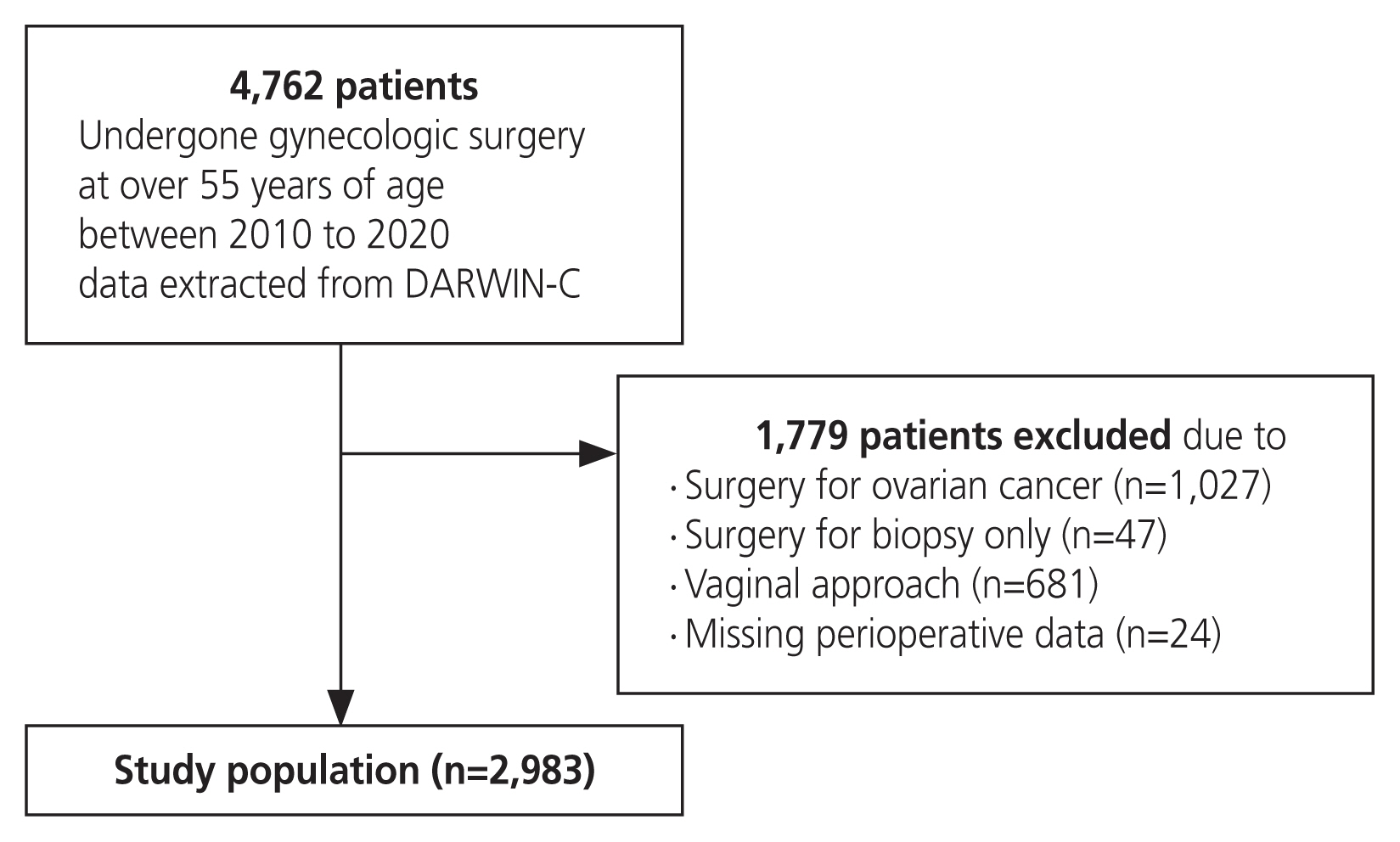
Fig. 1 Flowchart of patient selection. Patient selection was done by DARWIN-C (data analytics and research window for integrated knowledge-clinical data).

Fig. 2 Comparison of surgical outcomes between the age groups by surgical approach with linear regression analysis. (A) Comparison of EBL (mL) between age groups by surgical approach. (B) Comparison of transfusion (pints) between age groups by surgical approach. (C) Comparison of operation time (minutes) between age groups by surgical approach. (D) Comparison of hospital stay (days) between age groups by surgical approach. EBL, estimated blood loss.

Fig. 3 Comparison of surgical outcomes between the age groups by surgical approach with linear regression analysis (cancer only). (A) Comparison of EBL (mL) between age groups by surgical approach (cancer only). (B) Comparison of transfusion (pints) between age groups by surgical approach (cancer only). (C) Comparison of operation time (minutes) between age groups by surgical approach (cancer only). (D) Comparison of hospital stay (days) between age groups by surgical approach (cancer only). EBL, estimated blood loss.
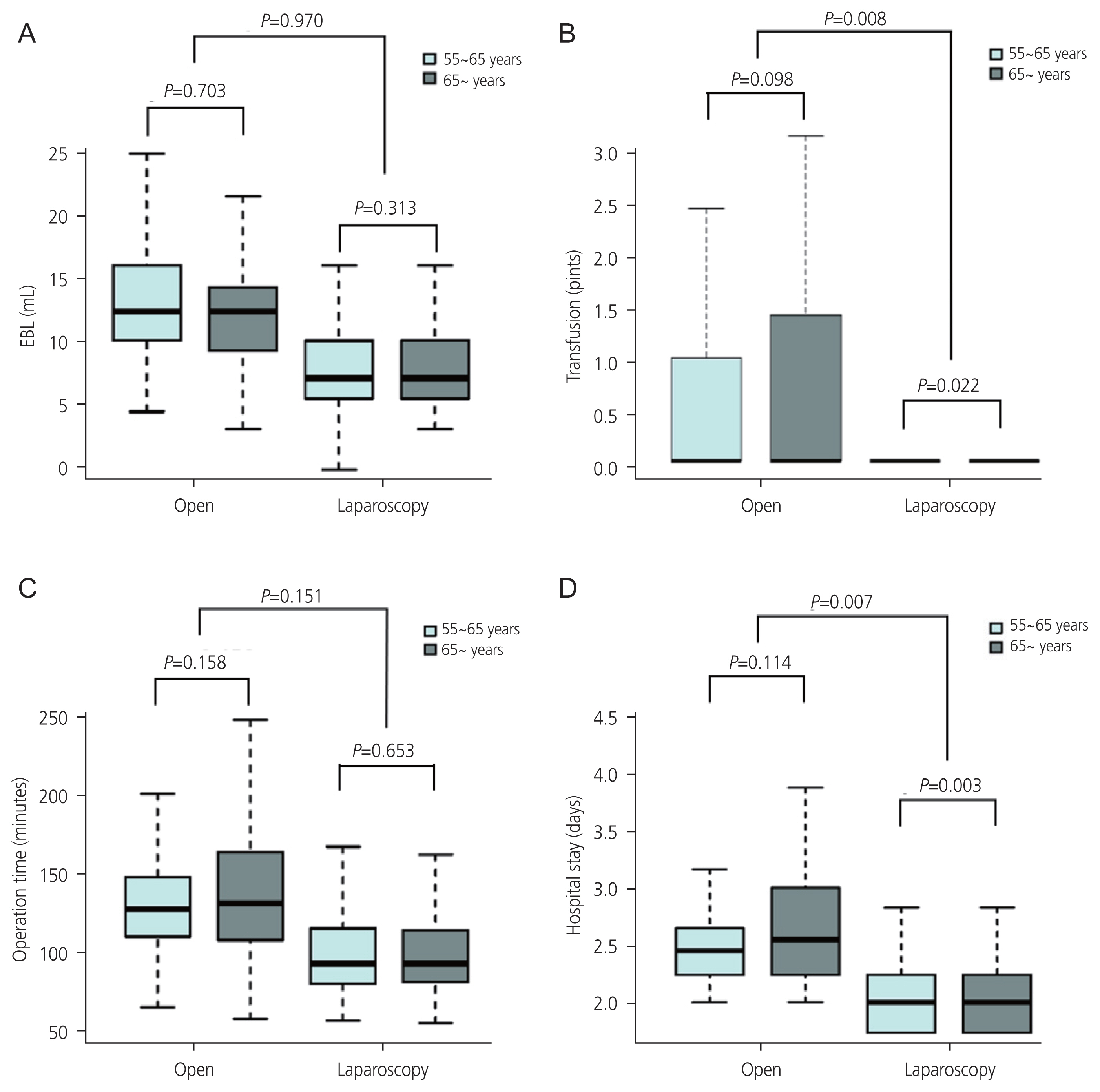
Fig. 4 Comparison of surgical outcomes between the age groups by surgical approach with linear regression analysis (benign only). (A) Comparison of EBL (mL) between age groups by surgical approach (benign only). (B) Comparison of transfusion (pints) between age groups by surgical approach (benign only). (C) Comparison of operation time (minutes) between age groups by surgical approach (benign only). (D) Comparison of hospital stay (days) between age groups by surgical approach (benign only). EBL, estimated blood loss.
Reference
-
References
1. De Marzi P, Ottolina J, Mangili G, Rabaiotti E, Ferrari D, Viganò R, et al. Surgical treatment of elderly patients with endometrial cancer (≥ 65 years). J Geriatr Oncol. 2013; 4:368–73.2. Turrentine FE, Wang H, Simpson VB, Jones RS. Surgical risk factors, morbidity, and mortality in elderly patients. J Am Coll Surg. 2006; 203:865–77.3. Hamel MB, Henderson WG, Khuri SF, Daley J. Surgical outcomes for patients aged 80 and older: morbidity and mortality from major noncardiac surgery. J Am Geriatr Soc. 2005; 53:424–9.4. Caglià P, Tracia A, Buffone A, Amodeo L, Tracia L, Amodeo C, et al. Physiopathology and clinical considerations of laparoscopic surgery in the elderly. Int J Surg. 2016; 33(Suppl 1):S97–102.5. Sultana CJ, Campbell JW, Pisanelli WS, Sivinski L, Rimm AA. Morbidity and mortality of incontinence surgery in elderly women: an analysis of Medicare data. Am J Obstet Gynecol. 1997; 176:344–8.6. Walker JL, Piedmonte MR, Spirtos NM, Eisenkop SM, Schlaerth JB, Mannel RS, et al. Laparoscopy compared with laparotomy for comprehensive surgical staging of uterine cancer: Gynecologic Oncology Group Study LAP2. J Clin Oncol. 2009; 27:5331–6.7. Kolarsick PA, Sacchi M, Spinelli A, Wexner SD. Minimizing the impact of colorectal surgery in the older patient: the role of minimally invasive surgery in the geriatric population. Eur J Surg Oncol. 2020; 46:333–7.8. Weber DM. Laparoscopic surgery: an excellent approach in elderly patients. Arch Surg. 2003; 138:1083–8.9. Myre K, Buanes T, Smith G, Stokland O. Simultaneous hemodynamic and echocardiographic changes during abdominal gas insufflation. Surg Laparosc Endosc. 1997; 7:415–9.10. O’Malley C, Cunningham AJ. Physiologic changes during laparoscopy. Anesthesiol Clin North Am. 2001; 19:1–19.11. Law WL, Chu KW, Tung PH. Laparoscopic colorectal resection: a safe option for elderly patients. J Am Coll Surg. 2002; 195:768–73.12. Frasson M, Braga M, Vignali A, Zuliani W, Di Carlo V. Benefits of laparoscopic colorectal resection are more pronounced in elderly patients. Dis Colon Rectum. 2008; 51:296–300.13. Ciavattini A, Di Giuseppe J, Cecchi S, Tsiroglou D, Mancioli F, Stevenazzi G, et al. Gynecologic laparoscopy in patients aged 65 or more: feasibility and safety in the presence of increased comorbidity. Eur J Obstet Gynecol Reprod Biol. 2014; 175:49–53.14. Buchweitz O, Matthias S, Müller-Steinhardt M, Malik E. Laparoscopy in patients over 60 years old: a prospective, randomized evaluation of laparoscopic versus open adnexectomy. Am J Obstet Gynecol. 2005; 193:1364–8.15. Suh DH, Kang S, Lim MC, Lee TS, Park JY, Kim TJ, et al. Management of the elderly patient with gynecologic cancer: report of the 2011 workshop in geriatric gynecologic oncology. Int J Gynecol Cancer. 2012; 22:161–9.16. Hannan EL, Racz MJ, Walford G, Ryan TJ, Isom OW, Bennett E, et al. Predictors of readmission for complications of coronary artery bypass graft surgery. JAMA. 2003; 290:773–80.17. Bentrem DJ, Cohen ME, Hynes DM, Ko CY, Bilimoria KY. Identification of specific quality improvement opportunities for the elderly undergoing gastrointestinal surgery. Arch Surg. 2009; 144:1013–20.18. Massarweh NN, Legner VJ, Symons RG, McCormick WC, Flum DR. Impact of advancing age on abdominal surgical outcomes. Arch Surg. 2009; 144:1108–14.19. Guy MS, Sheeder J, Behbakht K, Wright JD, Guntupalli SR. Comparative outcomes in older and younger women undergoing laparotomy or robotic surgical staging for endometrial cancer. Am J Obstet Gynecol. 2016; 214:350.e1–10.20. Windberger U, Siegl H, Ferguson JG, Schima H, Függer R, Herbst F, et al. Hemodynamic effects of prolonged abdominal insufflation for laparoscopic procedures. Gastrointest Endosc. 1995; 41:121–9.21. Jakimowicz J, Stultiëns G, Smulders F. Laparoscopic insufflation of the abdomen reduces portal venous flow. Surg Endosc. 1998; 12:129–32.22. Ball A, Bentley JR, O’Connell C, Kieser KE. Choosing the right patient: planning for laparotomy or laparoscopy in the patient with endometrial cancer. J Obstet Gynaecol Can. 2011; 33:468–74.23. Ramirez PT, Frumovitz M, Pareja R, Lopez A, Vieira M, Ribeiro R, et al. Minimally invasive versus abdominal radical hysterectomy for cervical cancer. N Engl J Med. 2018; 379:1895–904.24. Bishop EA, Java JJ, Moore KN, Spirtos NM, Pearl ML, Zivanovic O, et al. Surgical outcomes among elderly women with endometrial cancer treated by laparoscopic hysterectomy: a NRG/Gynecologic Oncology Group study. Am J Obstet Gynecol. 2018; 218:109e1–11.25. Krause AK, Muntz HG, McGonigle KF. Robotic-assisted gynecologic surgery and perioperative morbidity in elderly women. J Minim Invasive Gynecol. 2016; 23:949–53.26. Madden N, Frey MK, Joo L, Lee J, Musselman K, Chern JY, et al. Safety of robotic-assisted gynecologic surgery and early hospital discharge in elderly patients. Am J Obstet Gynecol. 2019; 220:253.e1–7.27. Oresanya LB, Lyons WL, Finlayson E. Preoperative assessment of the older patient: a narrative review. JAMA. 2014; 311:2110–20.28. Delvecchio A, Conticchio M, Riccelli U, Ferraro V, Ratti F, Gelli M, et al. Laparoscopic versus open liver resection for hepatocellular carcinoma in elderly patients: a propensity score matching analysis. HPB (Oxford). 2022; 24:933–41.29. Manceau G, Brouquet A, Chaibi P, Passot G, Bouché O, Mathonnet M, et al. Multicenter phase III randomized trial comparing laparoscopy and laparotomy for colon cancer surgery in patients older than 75 years: the CELL study, a Fédération de Recherche en Chirurgie (FRENCH) trial. BMC Cancer. 2019; 19:1185.30. Lee SB, Oh JH, Park JH, Choi SP, Wee JH. Differences in youngest-old, middle-old, and oldest-old patients who visit the emergency department. Clin Exp Emerg Med. 2018; 5:249–55.31. Uccella S, Bonzini M, Palomba S, Fanfani F, Malzoni M, Ceccaroni M, et al. Laparoscopic vs. open treatment of endometrial cancer in the elderly and very elderly: an age-stratified multicenter study on 1606 women. Gynecol Oncol. 2016; 141:211–7.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Recent advances of robotic surgery and single port laparoscopy in gynecologic oncology
- An Unsuspected Primary Tubal Carcinoma During Operative Laparoscopy
- Techniques of gynecologic single-port access laparoscopic surgery
- Laparoscopy-Assisted Distal Gastrectomy for Early Gastric Cancer in the Elderly
- The Clinical study of Pelviscopic Surgery
