Usefulness of cordless ultrasonic cutting energy devices in endoscopic nipple-sparing mastectomy: a retrospective study
- Affiliations
-
- 1Department of Surgery, School of Medicine, Kyungpook National University, Kyungpook National University Chilgok Hospital, Daegu, Korea
- KMID: 2553383
- DOI: http://doi.org/10.4174/astr.2024.106.3.147
Abstract
- Purpose
Endoscopic nipple-sparing mastectomy (E-NSM) is a minimally invasive surgical technique that shows good results in patients with breast cancer. The authors compared 3 different types of commercial energy devices to examine their efficacy and safety in E-NSM performed with breast reconstruction.
Methods
A total of 36 cases of E-NSM were conducted with either Sonicision (S group, n = 11), Harmonic (H group, n = 6), or Thunderbeat (T group, n = 19). The clinicopathologic factors and postoperative complications, including nipple or skin necrosis and surgical site seroma volume, were evaluated for 3 months after surgery.
Results
The surgical duration of E-NSM was significantly shorter in the S group than in the H group (P = 0.043) and T group (P = 0.037). However, the total surgical duration including E-NSM and breast reconstruction, and the total and daily drainage volume of postoperative seroma did not differ significantly among the 3 groups. Even when the energy devices were compared according to their working principle, i.e., ultrasonic (S and H) vs. hybrid (T), the total breast surgery duration and total and daily drainage volume of seroma showed no difference between the 2 groups. Although surgeon satisfaction did not significantly differ when using 3 devices for E-NSM (P = 0.428), surgeon’s fatigue was found to be lowest in the S group, though it was not significant (P = 0.064).
Conclusion
Any energy device can be safely used for E-NSM with breast reconstruction without causing any major complications. However, cordless ultrasonic energy devices allow greater mobility for the surgeon and, therefore, may shorten surgical time in breast surgery.
Figure
-
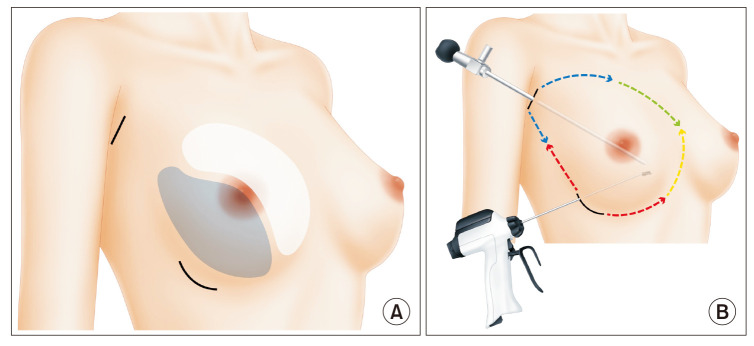
Fig. 1 Surgical process of endoscopic nipple-sparing mastectomy (E-NSM). After dissection of the anterior and posterior aspects of the breast with tumescent solution and scissors, surgery was performed according to the red→blue→green→yellow process. (A) The incisions on the inframammary fold were 5 cm long, whereas those in the axillary area were 4 cm long. Although the inferior and lateral parts (blue area) of the breast can be removed by open surgery, the superior and medial parts (white area) of the breast require endoscopic surgery. (B) Green and yellow areas of the breast required visualization with the endoscopic camera and longer instruments for conducting E-NSM.

Fig. 2 Tips to secure a larger space in the breast cavity during endoscopic nipple-sparing mastectomy. The specimen can be pulled out through the opposite incision. (A) To create a larger space superiorly (blue arrows), the breast specimen can be pulled out (red arrow) through the inframammary fold incision (black line). (B) To secure a larger space inferiorly (blue arrows), the breast specimen can be pulled out (red arrow) through an axillary incision (black line).
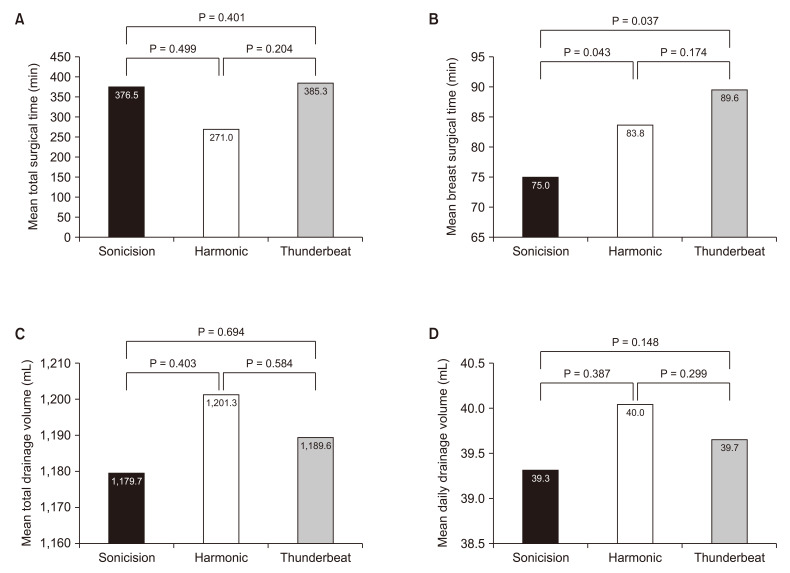
Fig. 3 The mean surgical duration and drainage volume of postoperative seroma. (A) The mean total surgical times among the Sonicision (S), Harmonic (H), and Thunderbeat (T) groups. (B) The mean breast surgery durations among the 3 groups. The S group showed a significantly shorter surgical duration than the other 2 groups (P = 0.043, P = 0.037). (C, D) The mean total drainage volume (C) and the mean daily drainage volume (D) of postoperative seroma among the 3 groups. Sonicision, Medtronic; Harmonic, Ethicon Endo-Surgery, Inc.; Thunderbeat, Olympus Corp.
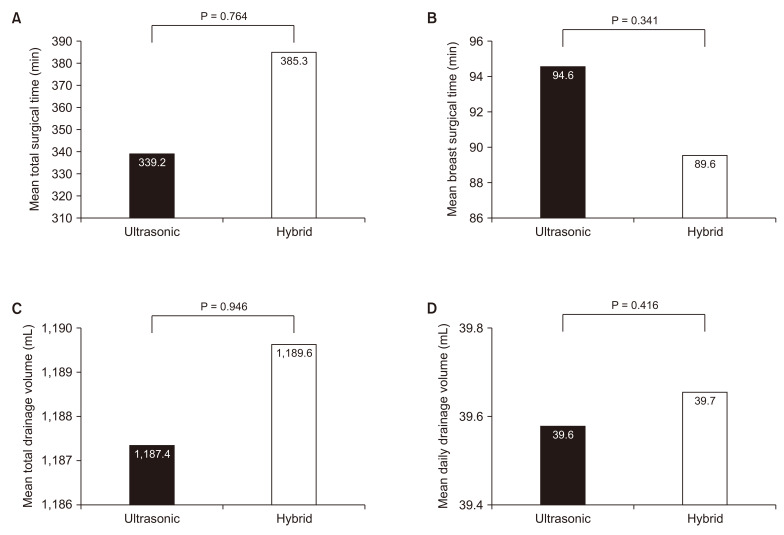
Fig. 4 The mean surgical duration and drainage volume of postoperative seroma. There was no significant difference in these characteristics between ultrasonic and hybrid energy devices. Comparing the mean total surgical duration (A), mean breast surgical duration (B), mean total drainage volume of postoperative seroma (C), and mean daily drainage volume of postoperative seroma (D) between the 2 groups.
Reference
-
1. Schwartzberg BS, Goates JJ, Kelley WE. Minimal access breast surgery. Surg Clin North Am. 2000; 80:1383–1398. PMID: 11059710.2. Mok CW, Lai HW. Evolution of minimal access breast surgery. Gland Surg. 2019; 8:784–793. PMID: 32042687.3. Soybir G, Fukuma E. Endoscopy assisted oncoplastic breast surgery (EAOBS). J Breast Health. 2015; 11:52–58. PMID: 28331692.4. Lai HW, Chen ST, Tai CM, Lin SL, Lin YJ, Huang RH, et al. Robotic- versus endoscopic-assisted nipple-sparing mastectomy with immediate prosthesis breast reconstruction in the management of breast cancer: a case-control comparison study with analysis of clinical outcomes, learning curve, patient-reported aesthetic results, and medical cost. Ann Surg Oncol. 2020; 27:2255–2268. PMID: 32016631.5. Sakamoto N, Fukuma E, Higa K, Ozaki S, Sakamoto M, Abe S, et al. Early results of an endoscopic nipple-sparing mastectomy for breast cancer. Ann Surg Oncol. 2009; 16:3406–3413. PMID: 19662457.6. Cimino WW. Ultrasonic surgery: power quantification and efficiency optimization. Aesthet Surg J. 2001; 21:233–241. PMID: 19331898.7. Shabbir A, Dargan D. Advancement and benefit of energy sealing in minimally invasive surgery. Asian J Endosc Surg. 2014; 7:95–101. PMID: 24754878.8. Sankaranarayanan G, Resapu RR, Jones DB, Schwaitzberg S, De S. Common uses and cited complications of energy in surgery. Surg Endosc. 2013; 27:3056–3072. PMID: 23609857.9. Chang YW, Kim HS, Jung SP, Woo SU, Lee JB, Bae JW, et al. Comparison of skin-sparing mastectomy using LigaSure™ Small Jaw and electrocautery. World J Surg Oncol. 2017; 15:129. PMID: 28709454.10. Harrell AG, Kercher KW, Heniford BT. Energy sources in laparoscopy. Semin Laparosc Surg. 2004; 11:201–209. PMID: 15510316.11. Lee D, Jung BK, Roh TS, Kim YS. Ultrasonic dissection versus electrocautery for immediate prosthetic breast reconstruction. Arch Plast Surg. 2020; 47:20–25. PMID: 31964119.12. Tupasi TE, Mangubat NV, Sunico ME, Magdangal DM, Navarro EE, Leonor ZA, et al. Malnutrition and acute respiratory tract infections in Filipino children. Rev Infect Dis. 1990; 12 Suppl 8:S1047–S1054. PMID: 2270404.13. Lai HW, Chen ST, Lin YJ, Lin SL, Lin CM, Chen DR, et al. Minimal access (endoscopic and robotic) breast surgery in the surgical treatment of early breast cancer-trend and clinical outcome from a single-surgeon experience over 10 years. Front Oncol. 2021; 11:739144. PMID: 34868935.14. Kell MR, Sharma S. Minimally invasive, maximal outcomes in breast surgery. Surgeon. 2016; 14:174–178. PMID: 26201516.15. Chang J, Rattner DW. History of minimally invasive surgical oncology. Surg Oncol Clin N Am. 2019; 28:1–9. PMID: 30414674.16. Pawlik TM. Minimally invasive oncologic surgery, part II. Surg Oncol Clin N Am. 2019; 28(Suppl 1):xiii–xxiv.17. Patrone R, Gambardella C, Romano RM, Gugliemo C, Offi C, Andretta C, et al. The impact of the ultrasonic, bipolar and integrated energy devices in the adrenal gland surgery: literature review and our experience. BMC Surg. 2019; 18(Suppl 1):123. PMID: 31074403.18. Back K, Hur N, Kim MJ, Choe JH, Kim JH, Kim JS. A prospective, randomized, controlled comparative study of three energy devices in open thyroid surgery: Thunderbeat, Harmonic, and Ligasure. J Endocr Surg. 2019; 19:106–115.19. Tou S, Malik AI, Wexner SD, Nelson RL. Energy source instruments for laparoscopic colectomy. Cochrane Database Syst Rev. 2011; (5):CD007886. PMID: 21563161.20. Harold KL, Pollinger H, Matthews BD, Kercher KW, Sing RF, Heniford BT. Comparison of ultrasonic energy, bipolar thermal energy, and vascular clips for the hemostasis of small-, medium-, and large-sized arteries. Surg Endosc. 2003; 17:1228–1230. PMID: 12799888.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Immediate Breast Reconstruction with TRAM Flap after Nipple-Areolar Sparing Mastectomy
- One-stage nipple and breast reconstruction using a deep inferior epigastric perforator flap after a skin-sparing mastectomy
- Skin-sparing Mastectomy and Immediate Nipple Graft for Large, Ptotic Breast
- Skin - sparing Mastectomy with Circumareolar Incision and Immediate TRAM & One - stage Star Flap Nipple - areolar Complex Reconstruction
- The Effect of Low-Dose Nitroglycerin Ointment on Skin Flap Necrosis in Breast Reconstruction after Skin-Sparing or Nipple-Sparing Mastectomy
