Leksell Frame-Based Stereotactic Biopsy for Infratentorial Tumor : Practical Tips and Considerations
- Affiliations
-
- 1Department of Neurosurgery, Chonnam National University Hwasun Hospital, Chonnam National University Medical School, Hwasun, Korea
- 2Department of Biomedical Engineering, Chonnam National University Hwasun Hospital, Chonnam National University Medical School, Hwasun, Korea
- KMID: 2553131
- DOI: http://doi.org/10.3340/jkns.2023.0108
Abstract
- The Leksell frame-based transcerebellar approach was proposed with the arc support frame attached upside down to the Z coordinate. This study presented practical tips and considerations for obtaining adequate tissue samples for deep-seated cerebellar lesions or lower brainstem lesions specifically those accessible via the cerebellar peduncle. For practical insights, the Leksell coordinate frame G was fixed to prevent the anterior screw implantation within the temporalis muscle, to avoid interference with the magnetic resonance (MR)-adapter, and taking into account the magnetic field of MR in close proximity to the tentorium. After mounting of indicator box, the MR imaging evaluation should cover both the indicator box and the infratentorial region that deviated from it. The coordinates [X, Y, Za, Arc0, Ringa0] obtained from Leksell SurgiPlan® software (Elekta, Stockholm, Sweden) with arc 00 located on the patient’s right side were converted to [X, Y, Zb=360–Za, Arc0, Ringb0=Ringa0–1800]. The operation was performed in the prone position under general anesthesia in four patients with deep cerebellar (n=3) and brainstem (n=1) tumors. The biopsy results showed two cases of diffuse large B-cell lymphoma, one metastatic braintumor and one glioblastoma. One patient required frame repositioning as a complication. Drawing upon the methodology outlined in existing literature, we anticipate that imparting supplementary expertise could render the stereotactic biopsy of infratentorial tumors more consistent and manageable for the practitioner, thereby facilitating adequate tissue samples and minimizing patient complications.
Keyword
Figure
-
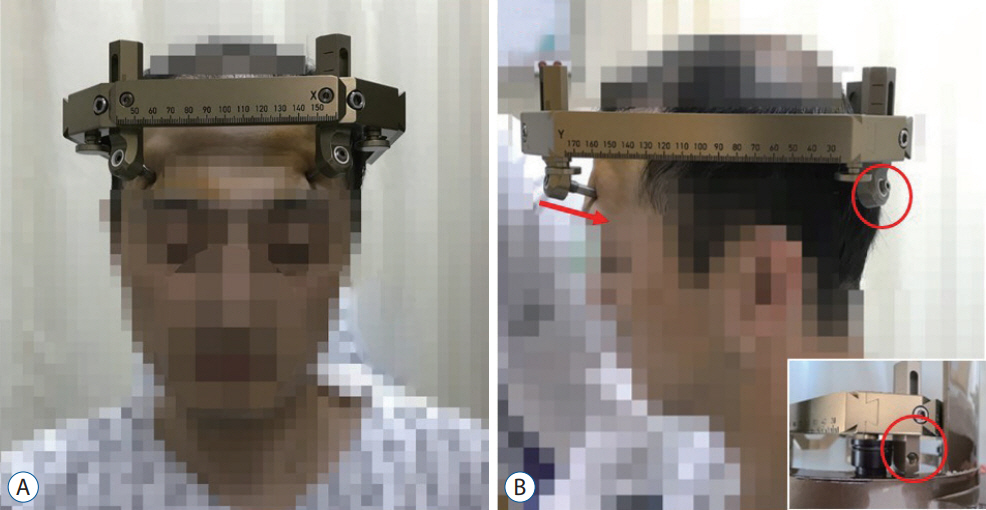
Fig. 1. The fixation of Leksell coordinate frame G. A : The insulated fixation posts must be fixed upside down. B : The anterior fixation screw with downward angulation is fixed not to penetrate too deeply into the temporalis muscle (arrow). The Leksell coordinate from G should be positioned on the supratentorial side, close to the tentorium. The inferior side of the insulated fixation post is set to the shortest length to avoid collision with the magnetic resonance-adapter (circles).
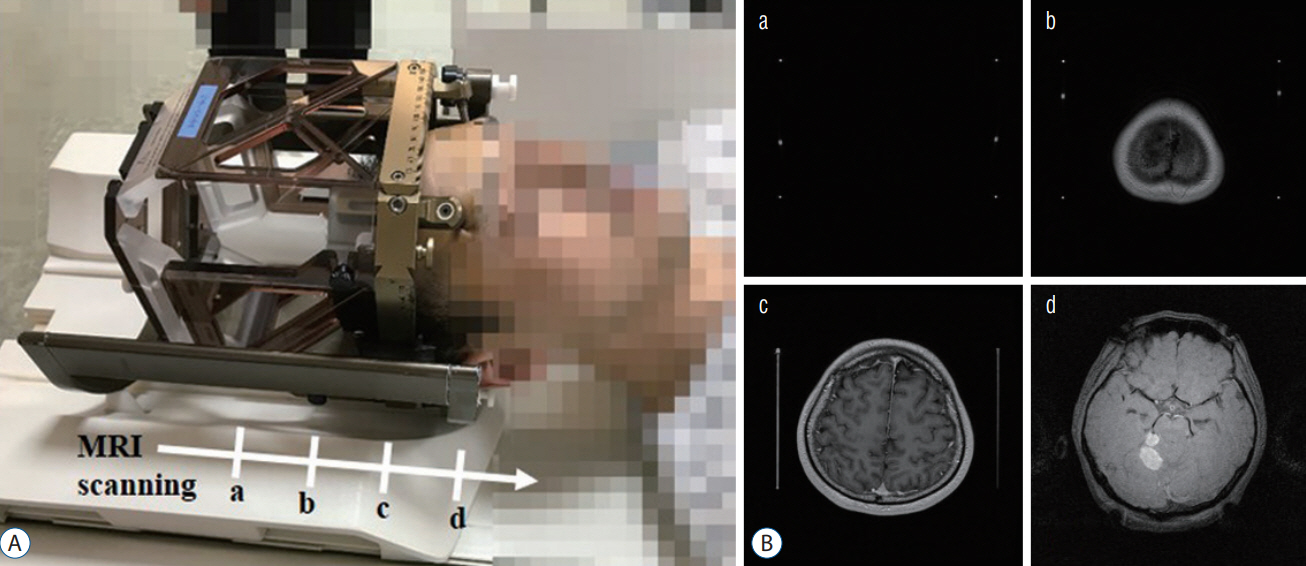
Fig. 2. Mounting of indicator box and acquisition of magnetic resonance imaging (MRI). A : The MR-Indicator box is positioned on top of the head. B : The MRI evaluation should encompass both the indicator box and the infratentorial region that deviated from it. The MRI scanning is on the indicator box only (a), vertex (b), supratentorial area (c), and infratentorial target lesion with weakened magnetic signal (d).
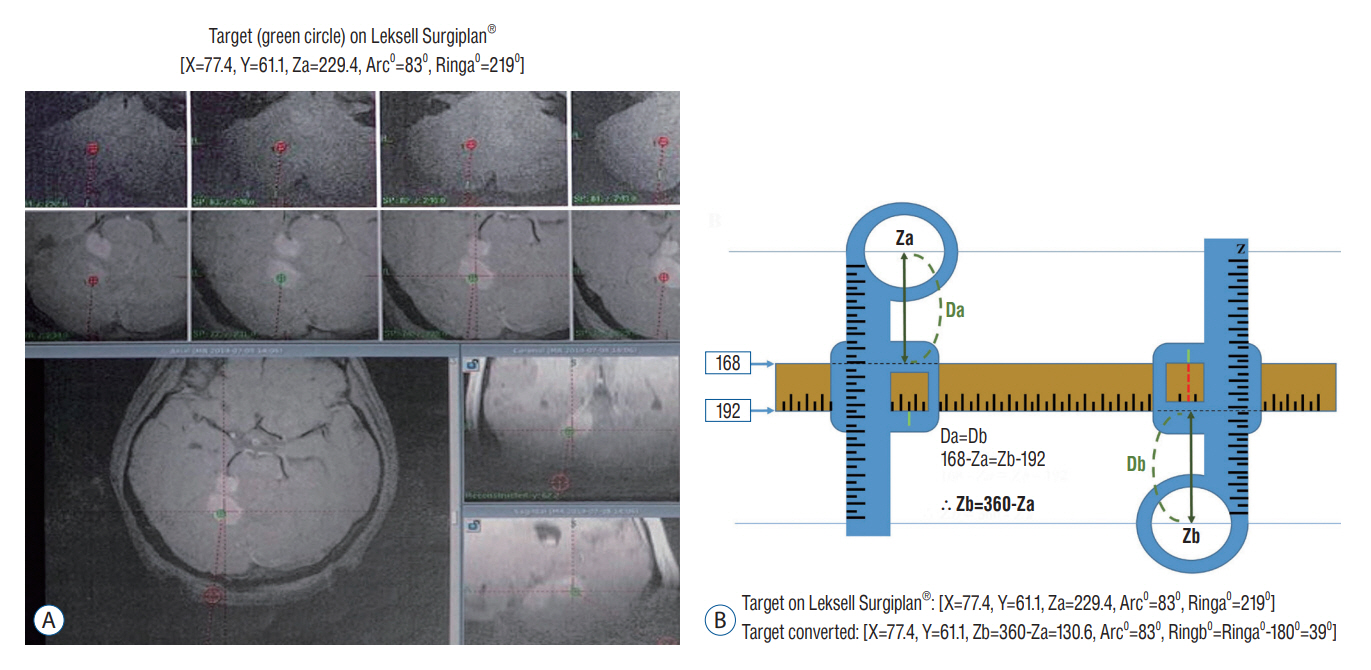
Fig. 3. Calculation of targets. A : The [X=77.4, Y=61.1, Za=229.4, Arc0=830, Ringa0=2190] coordinates of the target point can be calculated using Leksell SurgiPlan® software (elekta, Stockholm, Sweden) with arc 00 located on the patient’s right side. B : The upper and lower values of the Leksell coordinate Y scale are fixed at absolute values of 168 and 192, respectively. Using this, even when the phase is inverted, the distance from the center of the Z scale ring to the Y scale is the same (Da=db, 168–Za=Zb–192, Zb=360–Za). Using this conversion, we converted the coordinates obtained from the program to [X=77.4, Y=61.1, Zb=360–Za=130.6, Arc0=830, Ringb0=Ringa0–1800=390] (Za : Z coordinate on Leksell SurgiPlan®, Zb : Z coordinate calibration for operation target, Ringa0 : Ring angle on Leksell SurgiPlan®, Ringb0 : Ring angle calibration for operation target).

Fig. 4. Surgical procedures with the calculation of targets. A : The operation was performed with the patient in a prone position under general anesthesia. B and C : The converted coordinates [X=77.4, Y=61.1, Zb=360–Za=130.6, Arc0=830, Ringb0=Ringa0–1800=390] were adjusted to the graduations of each scale. The X-coordinate (arrow) was fixed on the right side (circle), whereas the Y and Z-coordinates (arrows) were fixed. The scale of the Y coordinate is hidden; therefore, it must be extended and drawn before installation. The Leksell coordinate slide can be adjusted even if mounted upside down as long as the sticker scale is visible using an adhesive-laminated label printer tape (Brother®; Brother Industries, Nagoya, Japan). D : The Ringb0 (390) was calculated by subtracting 1800 from Ringa0 (2190), and the Ring angle (arrow) was fixed. E : The calculated Arc0 (830) using Leksell SurgiPlan® (Elekta, Stockholm, Sweden) remained the same, and Arc angle (arrow) was fixed.
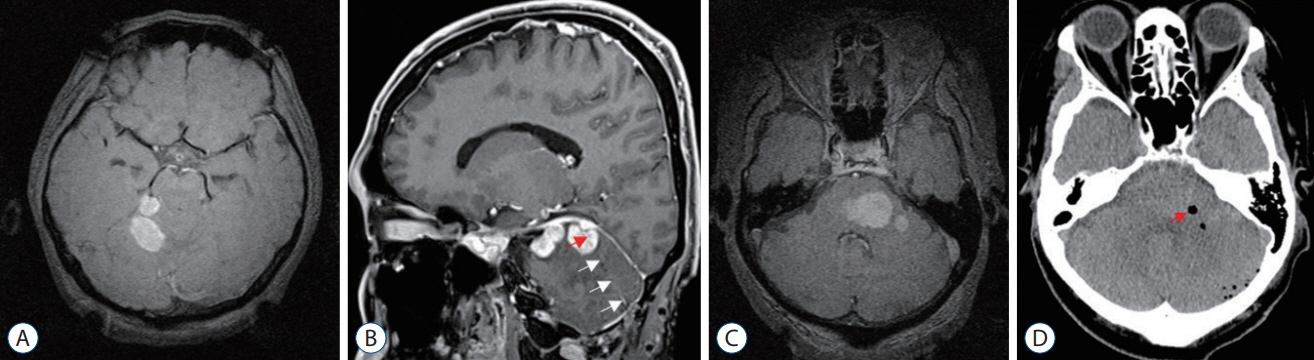
Fig. 5. Radiologic findings before and after biopsy. A : Deep cerebellar mass in case 1. B : The verified trajectory (white arrows) and biopsy target (red arrow) in case 1. C : Brain stem mass in case 2. D : Air (arrow) in the brain stem tumor where tissue was obtained in case 2.
Reference
-
References
1. Abernathey CD, Camacho A, Kelly PJ. Stereotaxic suboccipital transcerebellar biopsy of pontine mass lesions. J Neurosurg. 70:195–200. 1989.2. Bradac O, Steklacova A, Nebrenska K, Vrana J, de Lacy P, Benes V. Accuracy of varioguide frameless stereotactic system against frame-based stereotaxy: prospective, randomized, single-center study. World Neurosurg. 104:831–840. 2017.3. Chen SY, Chen CH, Sun MH, Lee HT, Shen CC. Stereotactic biopsy for brainstem lesion: comparison of approaches and reports of 10 cases. J Chin Med Assoc. 74:110–114. 2011.4. Coca HA, Cebula H, Benmekhbi M, Chenard MP, Entz-Werle N, Proust F. Diffuse intrinsic pontine gliomas in children: interest of robotic frameless assisted biopsy. A technical note. Neurochirurgie. 62:327–331. 2016.5. Coffey RJ, Lunsford LD. Stereotactic surgery for mass lesions of the mid-brain and pons. Neurosurgery. 17:12–18. 1985.6. Giese H, Hoffmann KT, Winkelmann A, Stockhammer F, Jallo GI, Thomale UW. Precision of navigated stereotactic probe implantation into the brainstem. J Neurosurg Pediatr. 5:350–359. 2010.7. Guthrie BL, Steinberg GK, Adler JR. Posterior fossa stereotaxic biopsy using the Brown-Roberts-Wells stereotaxic system. Technical note. J Neurosurg. 70:649–652. 1989.8. Haegelen C, Touzet G, Reyns N, Maurage CA, Ayachi M, Blond S. Stereotactic robot-guided biopsies of brain stem lesions: experience with 15 cases. Neurochirurgie. 56:363–367. 2010.9. Horisawa S, Nakano H, Kawamata T, Taira T. Novel use of the leksell gamma frame for stereotactic biopsy of posterior fossa lesions. World Neurosurg. 107:1–5. 2017.10. Jung IH, Chang KW, Park SH, Moon JH, Kim EH, Jung HH, et al. Stereotactic biopsy for adult brainstem lesions: a surgical approach and its diagnostic value according to the 2016 World Health Organization Classification. Cancer Med. 10:7514–7524. 2021.11. Lefranc M, Capel C, Pruvot-Occean AS, Fichten A, Desenclos C, Toussaint P, et al. Frameless robotic stereotactic biopsies: a consecutive series of 100 cases. J Neurosurg. 122:342–352. 2015.12. Lu L, Yang X, Raterman B, Jiang X, Meineke M, Grecula J, et al. Assessment of MRI image distortion based on 6 consecutive years of annual QAs and measurements on 14 MRI scanners used for radiation therapy. J Appl Clin Med Phys. 24:e13843. 2023.13. Mathisen JR, Giunta F, Marini G, Backlund EO. Transcerebellar biopsy in the posterior fossa: 12 years experience. Surg Neurol. 28:100–104. 1987.14. Neal JH, Van Norman AS. Transcerebellar biopsy of posterior fossa lesions using the Leksell gamma model stereotactic frame. Neurosurgery. 32:473–474. discussion 474-475. 1993.15. Parker P, Levesque MF, Bittoun J, Doyon D, Tadie M. Stereotactic transcerebellar approach to pontine lesions through the middle cerebellar peduncle. Interv Neuroradiol. 5:19–25. 1999.16. Phi JH, Chung HT, Wang KC, Ryu SK, Kim SK. Transcerebellar biopsy of diffuse pontine gliomas in children: a technical note. Childs Nerv Syst. 29:489–493. 2013.17. Sanai N, Wachhorst SP, Gupta NM, McDermott MW. Transcerebellar stereotactic biopsy for lesions of the brainstem and peduncles under local anesthesia. Neurosurgery. 63:460–466. discussion 466-468. 2008.18. Smith JS, Quiñones-Hinojosa A, Barbaro NM, McDermott MW. Frame-based stereotactic biopsy remains an important diagnostic tool with distinct advantages over frameless stereotactic biopsy. J Neurooncol. 73:173–179. 2005.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Frameless stereotactic brain biopsy: technical considerations and clinical results regarding safety and efficacy
- Application of Leksell Stereotactic Frame Using External Landmarks in Stereotactic Surgery
- Development of a Stereotactic Device for Gamma Knife Irradiation of Small Animals
- A delayed radiation-induced necrotic lesion in the brainstem mimicking tumor recurrence confirmed by stereotactic biopsy: a case report and literature review
- Stereotactic Resection of the Brain Tumor Using 'Tailed Bullets': Technical Note
