Child Kidney Dis.
2023 Dec;27(2):133-138. 10.3339/ckd.23.013.
Nutcracker syndrome combined with immunoglobulin A nephropathy: two case reports
- Affiliations
-
- 1Department of Pediatrics, Korea University Guro Hospital, Seoul, Republic of Korea
- 2Department of Pediatrics, Korea University Ansan Hospital, Ansan, Republic of Korea
- KMID: 2549746
- DOI: http://doi.org/10.3339/ckd.23.013
Abstract
- Nutcracker syndrome (NCS) is a disease caused by compression of the left renal vein between the superior mesenteric artery and the abdominal aorta. Immunoglobulin A (IgA) nephropathy (IgAN) is characterized by the predominance of IgA deposits in the glomerular mesangial area. Hematuria and proteinuria can be present in both diseases, and some patients can be concurrently diagnosed with NCS and IgAN; however, a causal relationship between the two diseases has not yet been clarified. Here, we report two pediatric cases of NCS combined with IgAN. The first patient presenting with microscopic hematuria and proteinuria was diagnosed with NCS at the initial visit, and the second patient was later diagnosed with NCS when proteinuria worsened. Both patients were diagnosed with IgAN based on kidney biopsy findings and treated with angiotensin-converting enzyme inhibitors and immunosuppressants. A high index of suspicion and timely imaging or biopsy are essential for the proper management of NCS combined with glomerulopathy.
Figure
-

Fig. 1. Renal Doppler ultrasound and clinical course of case 1. (A) Left renal vein (LRV) entrapment between the abdominal aorta and superior mesenteric artery (SMA). (B) Peak velocity at the renal hilum, 23.5 cm/s. (C) Peak velocity at the aortomesenteric portion, 149.8 cm/s. (D) Follow-up 24-hour urine protein and peak velocity ratio (PVR).
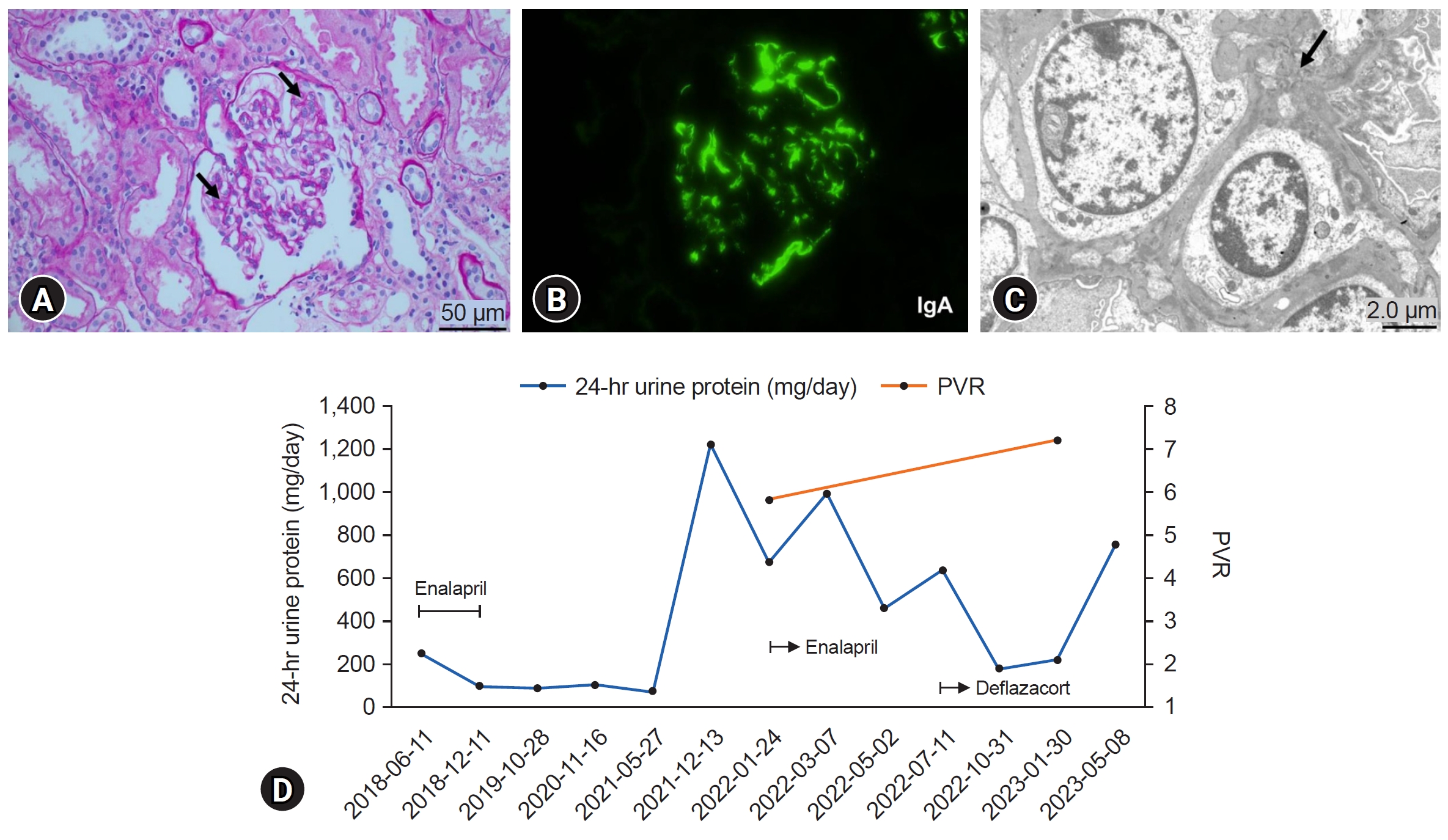
Fig. 2. Renal biopsy findings and clinical course of case 2. (A) A glomerulus with focal to diffuse mesangial proliferation (black arrows) (periodic acid-Schiff stain, ×400). (B) Strong immunoglobulin A (IgA) staining in mesangial regions (×400). (C) Electron-dense deposits in the mesangium (black arrow) (×4,000). (D) Follow-up 24-hour urine protein and peak velocity ratio (PVR).
Reference
-
References
1. Granata A, Distefano G, Sturiale A, Figuera M, Foti PV, Palmucci S, et al. From nutcracker phenomenon to nutcracker syndrome: a pictorial review. Diagnostics (Basel). 2021; 11:10.
Article2. Kolber MK, Cui Z, Chen CK, Habibollahi P, Kalva SP. Nutcracker syndrome: diagnosis and therapy. Cardiovasc Diagn Ther. 2021; 11:1140–9.
Article3. Shin JI, Park JM, Shin YH, Lee JS, Kim MJ, Jeong HJ. Nutcracker syndrome combined with IgA nephropathy in a child with recurrent hematuria. Pediatr Int. 2006; 48:324–6.
Article4. Rajasekaran A, Julian BA, Rizk DV. IgA nephropathy: an interesting autoimmune kidney disease. Am J Med Sci. 2021; 361:176–9.
Article5. Ozono Y, Harada T, Namie S, Ichinose H, Shimamine R, Nishimawa Y, et al. The “nutcracker” phenomenon in combination with IgA nephropathy. J Int Med Res. 1995; 23:126–31.
Article6. Wang C, Wang F, Zhao B, Xu L, Liu B, Guo Q, et al. Coexisting nutcracker phenomenon and superior mesenteric artery syndrome in a patient with IgA nephropathy: a case report. Medicine (Baltimore). 2021; 100:e26611.7. Wang F, Zhu H, Bao S, Qi H, Xu L, Liu X, et al. Associations of left renal vein entrapment with IgA nephropathy and Henoch-Schönlein purpura nephritis. Ren Fail. 2022; 44:1519–2.
Article8. Imai N, Shirai S, Shibagaki Y, Kimura K. Nutcracker phenomenon in IgA nephropathy. Clin Kidney J. 2014; 7:325–6.
Article9. Gulleroglu K, Gulleroglu B, Baskin E. Nutcracker syndrome. World J Nephrol. 2014; 3:277–81.
Article10. Meyer J, Rother U, Stehr M, Meyer A. Nutcracker syndrome in children: appearance, diagnostics, and treatment: a systematic review. J Pediatr Surg. 2022; 57:716–22.11. Park SJ, Lim JW, Cho BS, Yoon TY, Oh JH. Nutcracker syndrome in children with orthostatic proteinuria: diagnosis on the basis of Doppler sonography. J Ultrasound Med. 2002; 21:39–45.12. Ha TS, Lee EJ. ACE inhibition can improve orthostatic proteinuria associated with nutcracker syndrome. Pediatr Nephrol. 2006; 21:1765–8.
Article13. Keane WF, Raij L. Relationship among altered glomerular barrier permselectivity, angiotensin II, and mesangial uptake of macromolecules. Lab Invest. 1985; 52:599–604.14. Shao Y, Saredy J, Yang WY, Sun Y, Lu Y, Saaoud F, et al. Vascular endothelial cells and innate immunity. Arterioscler Thromb Vasc Biol. 2020; 40:e138–52.
Article15. Shimada S, Hirose T, Takahashi C, Sato E, Kinugasa S, Ohsaki Y, et al. Pathophysiological and molecular mechanisms involved in renal congestion in a novel rat model. Sci Rep. 2018; 8:16808.
Article
